Morel Lavelle lesion what's it causes etiology pathology investigation and treatment explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
Morel-Lavallee lesion etiology pathology investigation treatment 2024
Reading File
Reading File
Reading File
Reading File
Reading Web Page
https://www.pathologyoutlines.com/topic/softtissuemorellaval…
Loading Image
Loading Image
Finding Sources
Searching PubMed
Morel-Lavallee lesion treatment management
Finding Sources
Reading File
Searching PubMed
Morel-Lavallee lesion diagnosis treatment
Finding Sources
Reading File
Reading Article
PMID: 40905976
Loading Image
Loading Image
Finding Sources
Loading Image
I now have all the content needed. Let me compile the comprehensive answer.
Morel-Lavallee Lesion - Comprehensive Review
1. Definition and Historical Note
The Morel-Lavallee lesion (MLL) is a closed degloving injury first described in 1863 by the French surgeon Maurice Morel-Lavallee. It results from traumatic shearing forces that separate the skin and subcutaneous tissue from the underlying deep fascia, creating a potential space that fills with blood, lymph fluid, and liquefied fat debris. Although classically described over the greater trochanter and proximal thigh, it can occur at any site where mobile skin overlies a rigid fascial layer.
2. Etiology
The lesion arises from high-energy tangential/shearing trauma applied to the body surface:
| Cause | Notes |
|---|---|
| Motor vehicle accidents | ~25% of all MLL cases; most common overall cause |
| Crush injuries / run-over injuries | Particularly when a wheel rolls across a limb or pelvis |
| Sports injuries | Tackles, falls during contact sports |
| Mechanical falls | Especially in obese individuals where the subcutaneous tissue is abundant |
| Associated fractures | Pelvis, acetabulum, proximal femur - approximately 1.7% of pelvic fracture patients develop a clinically significant MLL |
Risk factors: Obesity significantly increases risk, as greater trochanteric shear forces are amplified by increased subcutaneous fat mass. The lesion is frequently missed in the acute setting because attention is directed toward distracting fractures.
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 58
- StatPearls - Morel-Lavallee Lesion, NCBI Bookshelf
3. Pathophysiology
The Shearing Mechanism
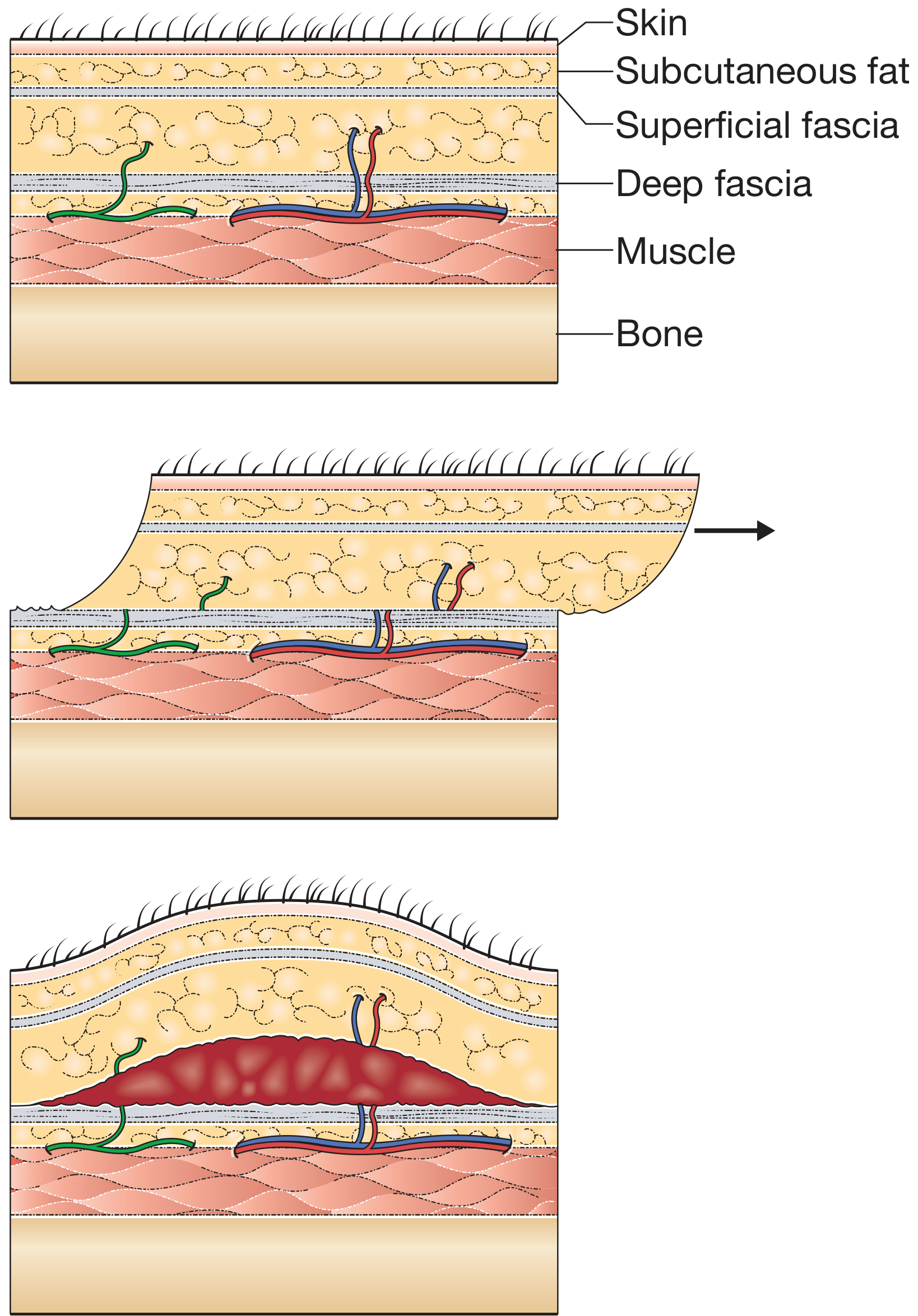
Figure 1 - Mechanism of injury. Top: Normal tissue layers (skin → subcutaneous fat → superficial fascia → deep fascia → muscle → bone). Middle: A tangential shearing force displaces the mobile skin/fat laterally over the fixed deep fascia. Bottom: Disruption of perforating arteries, veins, and lymphatics creates a hemolymphatic cavity in the pre-fascial plane. (Bailey and Love's Short Practice of Surgery 28th Ed, Fig. 3.12)
The MLL forms in areas where:
- The overlying skin is highly mobile (thigh, hip, knee, lumbar back, shoulder)
- The underlying fascia is tough and adherent to bone (quadriceps fascia, fascia lata, iliotibial band)
The shearing force disrupts:
- Transaponeurotic perforating capillaries - causing hemorrhage
- Lymphatic vessels - causing lymphorrhea
- Subdermal fat lobules - causing fat necrosis
Stages of Evolution
| Stage | Time | Pathological Changes |
|---|---|---|
| Acute | < 1 week | Fresh hemorrhage + lymph in the potential space; irregular, heterogeneous collection |
| Subacute | 1 - 6 weeks | Hemolysis, enzymatic liquefaction of fat; collection becomes more homogeneous |
| Chronic | > 6 weeks | Body attempts resorption via chronic inflammatory reaction; fibrous pseudocapsule forms around the cavity preventing further resorption; up to 46% of "closed" lesions culture positive at debridement |
The fibrous capsule is the key feature of the chronic/mature lesion - it seals off the cavity content, prevents healing, and sets the stage for recurrence and infection if not surgically managed.
- PathologyOutlines.com, Morel-Lavallee lesions, 2024
- Campbell's Operative Orthopaedics 15th Ed 2026
4. Common Anatomical Locations
| Location | Frequency |
|---|---|
| Greater trochanter / lateral thigh | > 60% of all cases - most common |
| Proximal thigh / quadriceps region | Very common, especially after pelvic fractures |
| Knee / popliteal area | Less common; sports-related |
| Buttock / sacral region | Associated with acetabular fractures |
| Lumbar dorsum | Less common; crush/fall injury |
| Shoulder, breast, cervical spine | Rare; reported in case literature |
Approximately 8% of patients who sustain a blow to the greater trochanter have a clinically significant MLL. - Campbell's Operative Orthopaedics 15th Ed 2026
5. Clinical Presentation
Symptoms:
- Swelling - often disproportionate to the apparent surface injury
- Ecchymosis / skin bruising and discoloration
- Fluctuance - a "fluid wave" palpable in the subcutaneous tissue
- Skin hypermobility - skin slides freely over the deeper tissue
- Pain / tenderness (variable; may be surprisingly mild)
- In late presentations: skin necrosis, tense bullae, wound breakdown

Figure 2 - Clinical appearance. A: Large Morel-Lavallee lesion of the thigh after pelvic fracture showing ecchymosis and hemorrhagic skin changes. B: View from behind showing asymmetric swelling. (Campbell's Operative Orthopaedics 15th Ed 2026, Fig. 58.11A-B)
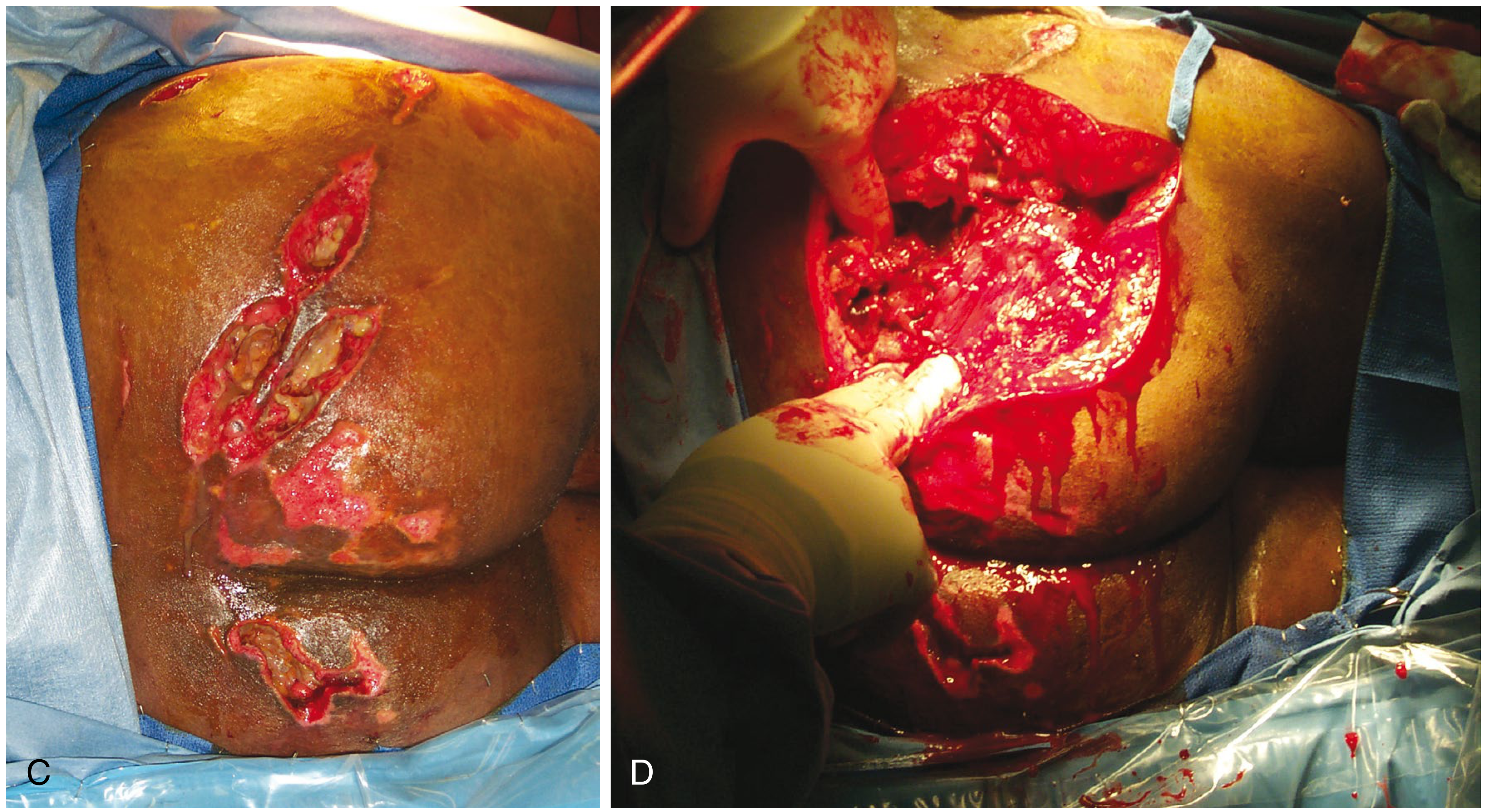
Figure 3 - C: Large MLL of the buttock with skin necrosis and multiple wound breakdowns. D: Operative exposure showing the depth and extent of the lesion cavity. (Campbell's Operative Orthopaedics 15th Ed 2026, Fig. 58.11C-D)
Key clinical sign: "A significant Morel-Lavallee lesion should be suspected in any patient with hypermobility of the skin or a fluid wave in the subcutaneous tissue." - Campbell's Operative Orthopaedics
6. Pathological Features (Histology)
On histopathological examination, the excised specimen shows:
- Reactive fibroadipose tissue with fibrosis
- Fat necrosis
- Hemorrhage (acute and hemosiderin-laden macrophages in chronic lesions)
- Pseudocyst formation lined by granulation tissue with reactive myofibroblasts
- The pseudocyst contains fibrin bands and hemorrhage
- No evidence of neoplasm or malignancy
Sample pathology report text: "Reactive fibroadipose tissue with associated fat necrosis, fibrous scar tissue and pseudocyst formation. The pseudocyst contains fibrin bands, hemorrhage and has granulation tissue with reactive myofibroblasts at the periphery." - PathologyOutlines.com
7. Investigations
7.1 Plain Radiography
- Limited utility for the lesion itself
- Important for detecting associated fractures (pelvis, acetabulum, femur)
- May show soft-tissue swelling
7.2 Ultrasonography
- Rapid, bedside-available, no radiation
- Can show: fluid collection in the pre-fascial plane, internal echogenicity, fat globules
- Point-of-care ultrasound (POCUS) is valuable in acute trauma settings
- Useful for guiding aspiration
- Less specific than MRI for lesion characterization
7.3 CT Scan
- Often the first imaging obtained in polytrauma patients
- Shows a hypodense, lens-shaped or elliptical fluid collection in the subcutaneous plane
- Can detect associated fractures simultaneously
- Should be "scrutinized for a fluid collection in the subcutaneous tissues" in any pelvic fracture patient
7.4 MRI - Investigation of Choice
MRI is the gold standard - it defines size, shape, contents, and chronicity of the lesion.
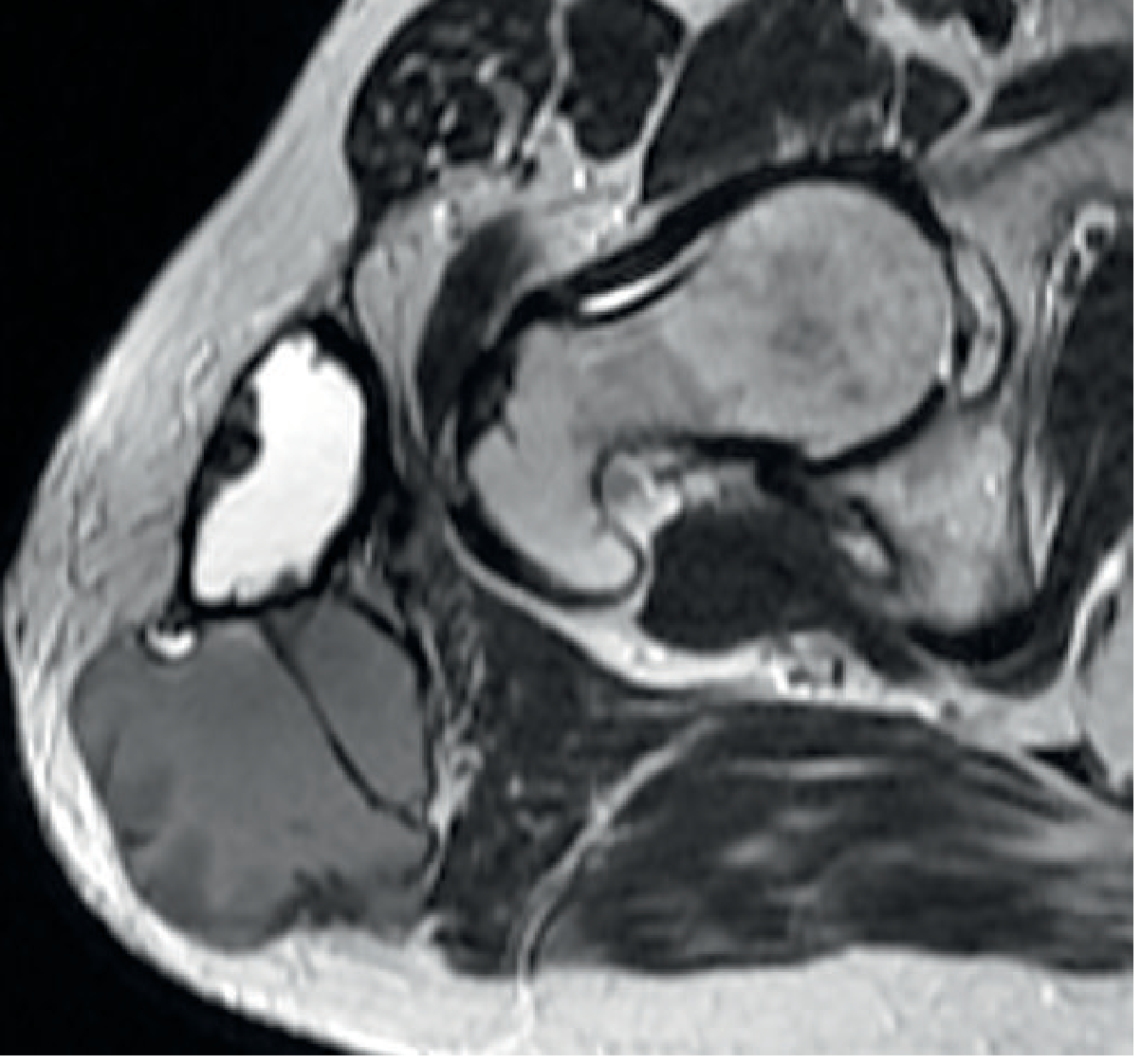
Figure 4 - MRI of Morel-Lavallee Lesion. Axial T2-weighted image of the right hip showing a heterogeneous, lobular mass in the deep subcutaneous fat at the lateral aspect. Low signal posteriorly is consistent with chronic haemorrhage. A thick, irregular low signal wall is visible anteriorly. The lesion was also hyperintense on T1 and showed rim enhancement on contrast sequences. (Grainger & Allison's Diagnostic Radiology, Fig. 42.31)
MRI Signal Characteristics by Phase:
| Phase | T1 | T2 | Features |
|---|---|---|---|
| Acute (< 1 week) | Hypointense | Hyperintense | Heterogeneous, irregular borders |
| Subacute (1-6 weeks) | Hyperintense | Hyperintense | More homogeneous; fluid-fluid levels |
| Chronic (> 6 weeks) | Variable | Variable | Hypointense rim (hemosiderin + fibrous capsule); internal heterogeneity; rim enhancement on contrast |
The hypointense rim on both T1 and T2 in chronic lesions is a hallmark - it represents a combination of hemosiderin deposition and fibrosis forming the pseudocapsule. The lesion is also typically an elliptical shape with tapering edges.
8. Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Simple hematoma | No fibrous capsule; smaller; no disruption of fascial plane |
| Bursitis | Located at specific bursae; fluid inside bursa, not pre-fascial plane |
| Soft-tissue sarcoma | Solid mass components, internal vascularity, perilesional edema |
| Abscess | Systemic infection signs; restricted diffusion on DWI-MRI |
| Lymphocele | Post-surgical; no trauma history |
9. Treatment
Treatment is selected based on lesion size, chronicity, and whether infection is present.
9.1 Conservative Management
- Observation with compression bandaging
- Suitable for very small, acute lesions (< 50 mL)
- Risk of recurrence is high; infection rate ~19% even with observation
- Not recommended for large or chronic lesions
9.2 Percutaneous Aspiration
- Needle/catheter aspiration of the fluid collection
- Quick and minimally invasive
- High recurrence rate
- Infection rate of 56% with aspiration alone vs. 19% with observation vs. 15% with excision
- Appropriate only for very small, acute collections
9.3 Percutaneous Drainage (Tseng-Tornetta Technique)
As described in Campbell's Operative Orthopaedics:
- Position patient to expose the lesion
- Make a 2-cm incision over the distal aspect of the lesion
- Make a second 2-cm incision at the superior/posterior extent
- Determine extent with a suction tip
- Additional incisions as needed for large lesions
- Send fluid for culture and sensitivity
- Drain the hematoma with suction
- Debride loose fat with a plastic brush
- Irrigate with pulsed lavage until fluid is clear
- Place a medium closed suction drain throughout the cavity
- Close incisions tightly
- Connect drain to wall suction until output < 30 mL/24 hours (may take up to 8 days)
- Continue IV cephalosporin or specific antibiotics for 24 hours post drain removal
Tseng and Tornetta reported good results in 19 patients using this percutaneous technique performed within 3 days of admission.
9.4 Sclerotherapy
- Aspiration followed by injection of a sclerosing agent into the cavity
- Common agents: doxycycline, ethanol, talc
- Effective for lesions up to 400 mL
- Prevents recurrence by obliterating the cavity
- Risk: contour deformities at the injection site
- Increasingly used as a minimally invasive first-line option
9.5 Fibrin Sealant Injection
- After aspiration, fibrin glue is injected to seal the space
- Limited evidence; used in selected cases
9.6 Open Surgical Debridement and Excision
- Preferred for large (> 50 mL), chronic, recurrent, or infected lesions
- Includes complete excision of the fibrous pseudocapsule
- Higher morbidity but lowest recurrence rate
- Negative pressure wound therapy (NPWT) may be used post-operatively
- Infection rate reported as high as 12% with repeated postoperative debridement when operating through an infected MLL
9.7 Endoscopic Debridement
- Emerging technique combining endoscopic debridement with percutaneous cutaneo-fascial suture
- Allows thorough cavity debridement via small portals
- Reported 3-year follow-up data shows favorable outcomes with rapid return to activity (Injury, 2024)
Treatment Algorithm Summary:
Acute / Small (< 50 mL) → Observation + compression
Acute / Small, persistent → Percutaneous aspiration ± sclerotherapy
Acute / Large (> 50 mL) → Percutaneous drainage (Tseng-Tornetta) or sclerotherapy
Subacute / Chronic, non-infected → Open drainage + debridement + excision of capsule
OR endoscopic debridement
Infected → Urgent open debridement + IV antibiotics
+ delayed fracture fixation (24h after drain removed,
output < 30 mL/day)
10. Complications
| Complication | Notes |
|---|---|
| Infection / Sepsis | Up to 46% of lesions culture positive at debridement |
| Skin necrosis | Due to devascularization; requires skin grafting |
| Surgical site infection after fracture fixation | MLLs are an independent risk factor; infection rate after ORIF through an MLL is ~12% |
| Recurrence | Especially with aspiration alone |
| Pseudocapsule formation | Prevents healing; requires excision |
| Seroma | Persistent fluid re-accumulation |
| Contour deformity | After sclerotherapy |
11. Special Considerations in Fracture Surgery
In patients with acetabular fractures and concomitant MLL, the infection risk of operating through the lesion is high. Recommended approach:
- Perform percutaneous decompression and debridement first
- Wait at least 24 hours after drain removal with output < 30 mL/day
- Consider using an anterior approach to avoid the affected lateral hip area
- Do not proceed with posterior ORIF through an active/infected MLL
12. Key Takeaways
- MLL is a closed degloving injury from shearing trauma - skin/fat separated from deep fascia
- Most common at the greater trochanter and proximal lateral thigh (> 60% of cases)
- Frequently missed or delayed in diagnosis due to distracting fractures
- MRI is the investigation of choice - elliptical subcutaneous collection with hypointense rim in chronic lesions
- Collections > 50 mL are at high risk of infection and should be managed surgically
- Definitive treatment for chronic lesions is open debridement with complete excision of the fibrous capsule
- Operating through an undebrided MLL significantly increases surgical site infection risk
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 58 (Soft Tissue Injury) and Chapter on Acetabular Fractures
- Bailey and Love's Short Practice of Surgery 28th Ed, Chapter 3 (Degloving)
- Grainger & Allison's Diagnostic Radiology, Chapter 42 (Traumatic Lesions)
- Rockwood and Green's Fractures in Adults 10th Ed 2025, Chapter 16 (Degloving Injuries)
- Sarani N et al. "Morel-Lavallée lesion: What you need to know." J Trauma Acute Care Surg. 2026. [PMID: 40905976] (Systematic Review, Level I evidence)
- PathologyOutlines.com, Morel-Lavallée lesions, 2024
This is a shared conversation. Sign in to Orris to start your own chat.