
Does all this cause bilateral hand wasting
BL Hand Muscle Wasting — Does Everything on This Diagram Cause It?
LEFT BRANCH: UMN Signs (+) → Mixed UMN + LMN
| # | Condition | Causes Bilateral Hand Wasting? |
|---|---|---|
| ① | Syringomyelia | ✅ Yes — cavity destroys anterior horn cells at C8–T1, causing bilateral, suspended/cape distribution wasting with dissociated sensory loss |
| ② | Cervical Spondylitic Myelopathy | ✅ Yes — cord compression at C5–C6 or C3–C4 can cause bilateral intrinsic hand wasting (C8–T1 myotomes) + long tract signs. Harrison's confirms: "The diagnosis should always be considered in cases of progressive cervical myelopathy… or wasting of the hands" |
| ③ | Intramedullary Tumours | ✅ Yes — same mechanism as syringomyelia (central cord expansion destroys anterior horn cells bilaterally) |
| ④ | MND → ALS | ✅ Yes — classic presentation. ALS causes split-hand pattern (preferential thenar > hypothenar wasting). "As the weeks and months pass, the other hand and arm become similarly affected" — Adams & Victor's Neurology |
RIGHT BRANCH: Pure LMN Type
Anterior Horn Cell
| Condition | Bilateral Hand Wasting? |
|---|---|
| PMA (Progressive Muscular Atrophy) | ✅ Yes — pure LMN MND, bilateral wasting |
| Kennedy's Disease | ✅ Yes — X-linked bulbospinal muscular atrophy, bilateral proximal > distal wasting |
| Hirayama Disease | ⚠️ Typically unilateral or asymmetric — juvenile muscular atrophy of the distal upper limb. Characteristically unilateral (dominant side), though bilateral cases exist. This is a notable exception |
| Polio / Enterovirus / Coxsackievirus | ⚠️ Can be bilateral but typically asymmetric/patchy, not symmetrically bilateral |
Root (C8–T1 Radiculopathy)
| Condition | Bilateral Hand Wasting? |
|---|---|
| Cervical Spondylosis (radiculopathy) | ⚠️ Usually unilateral — C8/T1 root compression is typically on one side. Bilateral only if multilevel stenosis affects both sides |
| Cervical Rib / TOS | ⚠️ Usually unilateral |
Plexus
| Condition | Bilateral Hand Wasting? |
|---|---|
| Pancoast Tumour | ⚠️ Unilateral — involves lower trunk (C8/T1) of one brachial plexus only |
| Lower Trunk Brachial Plexopathy | ⚠️ Usually unilateral |
| Thoracic Outlet Syndrome | ⚠️ Usually unilateral |
Peripheral Nerve
| Condition | Bilateral Hand Wasting? |
|---|---|
| Median Neuropathy (bilateral CTS) | ✅ Yes — bilateral carpal tunnel syndrome is common; causes thenar wasting bilaterally |
| Ulnar Neuropathy | ⚠️ Usually unilateral; bilateral possible but less common |
| Combined Neuropathy | ✅ Yes |
| CMT (Charcot–Marie–Tooth) | ✅ Yes — hereditary motor and sensory neuropathy, classically bilateral and symmetric |
| mmNCB (likely MMN — Multifocal Motor Neuropathy with Conduction Block) | ⚠️ Typically asymmetric/multifocal, not symmetrically bilateral |
| Leprosy | ✅ Yes — bilateral ulnar + median nerve involvement causes bilateral hand wasting in endemic regions |
Muscle
| Condition | Bilateral Hand Wasting? |
|---|---|
| Distal Myopathy / Miyoshi | ✅ Yes — Miyoshi myopathy affects distal limbs bilaterally (though primarily lower limb in Miyoshi) |
| LGCOE (likely LGMD — Limb Girdle CMD/Myopathy?) | ⚠️ Primarily proximal; distal hand wasting is not a major feature |
| IBM (Inclusion Body Myositis) | ✅ Yes — IBM is unique among myopathies in causing finger flexor and quadriceps wasting bilaterally |
| Myotonic Dystrophy | ✅ Yes — distal wasting, bilateral hand/forearm involvement is characteristic |
Bottom Left: Disuse Atrophy → RA
| Condition | Bilateral Hand Wasting? |
|---|---|
| RA + Disuse Atrophy | ✅ Yes — rheumatoid arthritis causes interosseous wasting from a combination of disuse atrophy, vasculitis, and entrapment neuropathy (median/ulnar). Classically bilateral and symmetric |
Summary
- Typically unilateral (unless bilateral disease): Pancoast tumour, lower trunk plexopathy, TOS, C8–T1 radiculopathy, ulnar neuropathy
- Characteristically unilateral/asymmetric: Hirayama disease, MMN (multifocal motor neuropathy)
- Bilateral but primarily proximal (hand wasting not a main feature): LGMD
60 Yr with female with pancerebellar symp with wt loss 10 kg what other history to ask
History to Ask — Structured Approach
🔴 The Working Diagnosis: Paraneoplastic Cerebellar Degeneration (PCD)
| Cancer | Antibody |
|---|---|
| Ovarian / Uterine | Anti-Yo (PCA-1) — most common in women |
| Breast | Anti-Yo, Anti-Ri |
| Small Cell Lung (SCLC) | Anti-Hu, Anti-Zic4, Anti-VGCC |
| Hodgkin Lymphoma | Anti-Tr (mGluR1) |
"Paraneoplastic cerebellar degeneration associated with breast and gynecologic (ovaries, uterus) carcinomas — anti-Yo, anti-Ri antibodies" — Localization in Clinical Neurology, 8e
1. History of Presenting Illness — Cerebellar Symptoms
- Onset and progression — subacute onset over weeks to months is a red flag for PCD (vs. slow years-long course of hereditary ataxia)
- Sequence — which came first: gait unsteadiness, limb ataxia, slurred speech, double vision, oscillopsia?
- Any nystagmus / oscillopsia noticed?
- Dysphagia or dysphonia — brainstem involvement (paraneoplastic encephalomyelitis overlap)
- Cognitive changes / memory problems — limbic encephalitis component?
- Sensory symptoms in limbs — sensory neuronopathy (anti-Hu)
- Autonomic symptoms — postural dizziness, constipation, gastroparesis (anti-Hu PEM)
2. Gynecological / Oncological History ← Most Critical in a 60F
- Last Pap smear / cervical screening — when was it done?
- Postmenopausal bleeding — endometrial/uterine carcinoma
- Breast lump, nipple discharge, last mammogram — breast cancer (anti-Yo)
- Ovarian symptoms — bloating, early satiety, pelvic fullness (ovarian carcinoma)
- Family history of breast, ovarian, or colorectal cancer (BRCA risk)
3. Weight Loss Characterisation
- Duration — how long for 10 kg loss?
- Associated anorexia vs. normal appetite (anorexia + weight loss = malignancy)
- Night sweats — lymphoma (Hodgkin's → anti-Tr cerebellar degeneration)
- Dysphagia / odynophagia — oesophageal/gastric malignancy
- Haemoptysis / chronic cough / smoker — SCLC (anti-Hu)
- Change in bowel habits, rectal bleeding — colorectal cancer
4. Smoking & Substance History
- Smoking pack-years — SCLC most associated with PCD via anti-Hu; also risk for paraneoplastic encephalomyelitis
- Alcohol — chronic alcohol use is a major non-paraneoplastic cause of cerebellar degeneration (vermis predominant, but can be pancerebellar)
- Alcohol quantity and duration — vermis atrophy, thiamine deficiency (Wernicke's)
5. Medication & Toxic History
- Phenytoin — classic cause of cerebellar atrophy/toxicity
- Chemotherapy (prior cancer treatment) — cytarabine, 5-FU, methotrexate can cause cerebellar syndrome
- Lithium toxicity
- Heavy metals — mercury, lead
6. Family History
- Hereditary ataxias (SCA — spinocerebellar ataxia types): onset at 60 is late but possible for SCA3/SCA6
- Family history of ataxia, Parkinson's, tremor
7. Past Medical History
- Prior malignancy (even if "cured" — recurrence can present with PCD, including Hodgkin's)
- Hypothyroidism — cause of cerebellar syndrome (ask about fatigue, cold intolerance, constipation)
- Coeliac disease — ask about chronic diarrhoea, bloating (gluten ataxia)
- Diabetes — non-ketotic hyperglycaemia can cause cerebellar signs; also peripheral neuropathy
- Autoimmune disease — SLE, Sjögren's (anti-Ro antibodies linked to cerebellar ataxia)
8. Systems Review
- Rash — dermatitis herpetiformis (gluten ataxia), or paraneoplastic
- Uveitis / vision changes
- Myoclonus / jerks — opsoclonus-myoclonus (anti-Ri, breast/gynaecological)
- Psychiatric symptoms — depression, anxiety, personality change (limbic involvement)
Bottom Line for Exam
- Gynaecological cancer (ovary/uterus → anti-Yo) — most likely in this demographic
- Breast cancer screening history
- Smoking/SCLC (anti-Hu)
- Lymphoma (night sweats, nodes → anti-Tr)
- Alcohol (non-paraneoplastic cause to exclude)
- Subacute onset (weeks–months) — confirms paraneoplastic pattern vs. hereditary (years)
Differential for temporal hyperintensity and approch
Temporal Lobe Hyperintensity on MRI — Differentials & Approach
DIFFERENTIALS
🔴 Category 1: Infectious / Inflammatory
| Diagnosis | Key Features |
|---|---|
| Herpes Simplex Encephalitis (HSE-1) | Most important to exclude — haemorrhagic necrosis of medial temporal lobe + insula + cingulate. Unilateral → bilateral. Fever, personality change, seizures, aphasia. Spares basal ganglia |
| HHV-6 Encephalitis | Symmetric bilateral medial temporal hyperintensity; post-bone marrow / stem cell transplant setting |
| Autoimmune / Limbic Encephalitis | Unilateral or bilateral mesial temporal FLAIR/T2 signal, best seen on coronal sequences; subacute amnesia, seizures, psychiatric features |
| Tuberculous/Fungal encephalitis | Often with leptomeningeal enhancement; basal ganglia involvement also |
🟠 Category 2: Autoimmune / Paraneoplastic Limbic Encephalitis
| Antibody | Clinical Clue | Associated Tumour |
|---|---|---|
| Anti-Hu | Sensory neuronopathy + limbic encephalitis | SCLC |
| Anti-Ma2 | Young man + upper brainstem + limbic | Testicular germ cell |
| Anti-LGI1 | Faciobrachial dystonic seizures (FBDS), hyponatraemia | Thymoma (minor) |
| Anti-CASPR2 | Morvan syndrome, neuromyotonia | Thymoma |
| Anti-AMPA-R | Relapsing course | Lung, breast, thymoma |
| Anti-GABA-B | Prominent seizures | SCLC |
| Anti-NMDAR | Young female, psychiatric → movement disorder → coma | Ovarian teratoma |
"Typical MRI findings include unilateral or bilateral mesial temporal lobe abnormalities best seen on T2-weighted and FLAIR images. The temporal-limbic regions may be hypointense on T1 and rarely enhance with contrast." — Bradley & Daroff's Neurology
🟡 Category 3: Vascular
| Diagnosis | Key Features |
|---|---|
| PCA territory infarct | Acute DWI restriction + FLAIR; ipsilateral field defect; look for contralateral peduncle (Wernicke haemianopia) |
| CADASIL | Temporal pole white matter involvement is pathognomonic (distinguishes from other small vessel disease). NOTCH3 mutation, migraine, lacunar strokes, family history |
| Cerebral venous sinus thrombosis | FLAIR hyperintensity ± haemorrhage; does not respect arterial territories |
| Vasculitis (CNS) | Multifocal, bilateral; headache, CSF pleocytosis |
🟢 Category 4: Tumour
| Diagnosis | Key Features |
|---|---|
| Low-grade glioma | FLAIR hyperintensity without enhancement; slow expansion; often incidental or seizures |
| DNET / Ganglioglioma | Young patient with chronic temporal lobe epilepsy; bubbly T2, cortical-based |
| GBM | Ring enhancement, mass effect, oedema; older adult |
| Lymphoma | Periventricular/deep; may involve temporal lobe; enhancing |
| Metastasis | Usually cortical/grey-white junction; multiple; known primary |
🔵 Category 5: Metabolic / Toxic / Genetic
| Diagnosis | Key Features |
|---|---|
| MELAS | Stroke-like episodes; posterior > anterior; crosses vascular territories; maternal inheritance, young age, lactic acidosis |
| Wernicke Encephalopathy | Medial thalami + mammillary bodies + periaqueductal grey; temporal involvement less typical |
| Hypoglycaemia | Can mimic stroke; posterior temporal/parietal; DWI changes |
| Status epilepticus | Post-ictal/peri-ictal FLAIR hyperintensity in the hippocampus; transient; resolves |
| Hippocampal Sclerosis | Unilateral hippocampal FLAIR hyperintensity + volume loss; longstanding TLE history |
APPROACH
Step 1 — Characterise the MRI Signal
| Feature | Implication |
|---|---|
| Medial temporal (hippocampus, amygdala, parahippocampus) | HSE, limbic encephalitis, hippocampal sclerosis |
| Medial + insula + cingulate | HSE (classic triad) |
| Temporal pole white matter | CADASIL |
| Bilateral symmetric mesial | Autoimmune limbic encephalitis, HHV-6 |
| Unilateral + cortical | Infarct (PCA), HSE, low-grade glioma |
| Swelling + mass effect | HSE (haemorrhagic), high-grade glioma, abscess |
| DWI restriction | Acute infarct, HSE, status epilepticus |
| Enhancement | Tumour, abscess, HSE (late), autoimmune (rare) |
Step 2 — Clinical Context (History + Exam)
| Feature | Points Toward |
|---|---|
| Fever + rapid onset | HSE |
| Subacute amnesia + psychiatric symptoms | Limbic encephalitis |
| Faciobrachial dystonic seizures | Anti-LGI1 |
| Hyponatraemia | Anti-LGI1 |
| Known malignancy | Paraneoplastic |
| Young woman + psych features | Anti-NMDAR |
| Migraine + strokes + family history | CADASIL |
| Immunocompromised | HHV-6, opportunistic infection |
| Post-ictal state | Peri-ictal changes |
| Chronic seizures + atrophy | Hippocampal sclerosis |
Step 3 — Investigations
- FBC, CRP, ESR
- Electrolytes (hyponatraemia → LGI1)
- Serum autoimmune encephalitis panel: Anti-NMDAR, LGI1, CASPR2, AMPAR, GABA-B, Hu, Ma2
- Paraneoplastic screen (Anti-Hu, Yo, Ri)
- Lactic acid (MELAS)
- Thyroid (Hashimoto encephalopathy)
- Opening pressure, cells, protein, glucose
- HSV PCR ← start empirical aciclovir BEFORE result
- VZV, EBV, HHV-6, CMV PCR
- Oligoclonal bands
- CSF autoimmune antibodies (more sensitive than serum for some)
- Cytology (if malignancy suspected)
- Temporal lobe epileptiform activity supports limbic encephalitis or TLE
- Periodic lateralising discharges (PLEDs) → HSE
- MRI with contrast — enhancement pattern
- MR spectroscopy — if tumour vs. inflammation unclear
- PET/CT whole body — if autoimmune/paraneoplastic (find hidden primary)
- CT chest/abdomen/pelvis — tumour screen
Step 4 — Management Principle
Temporal lobe hyperintensity → fever/acute onset?
↓ YES → Start IV Aciclovir immediately (HSE treatment)
↓ NO → Subacute? → Autoimmune workup + paraneoplastic screen
→ Seizures only? → Consider status/postictal change
→ Structural/chronic? → Tumour / hippocampal sclerosis workup
What CSF findings differentiate HSE from limbic encephalitis?
CSF Findings: HSE vs Limbic Encephalitis
| Parameter | HSE | Autoimmune Limbic Encephalitis |
|---|---|---|
| Opening pressure | Elevated (180–400 mmH₂O) | Usually normal |
| Appearance | Clear or xanthochromic (if haemorrhagic) | Clear |
| White cells | 10–1,000 cells/µL, predominantly lymphocytes | Mild lymphocytic pleocytosis or normal (up to 50% normal) |
| Red blood cells | ✅ Present — up to 500 RBC/µL; reflects haemorrhagic necrosis | ❌ Absent |
| Protein | Elevated — typically 50–200 mg/dL (up to 870 mg/dL reported) | Mildly elevated or normal (>50 mg/dL) |
| Glucose | Usually normal; low in ~5% | Normal |
| HSV PCR | ✅ Positive (sens ~96%, spec ~99%) — diagnostic | Negative |
| Specific antibodies | Negative | Positive — Anti-LGI1, NMDAR, CASPR2, GABA-B, Hu, Ma2, etc. |
| Oligoclonal bands | May be present (non-specific) | May be present (non-specific) |
Key Differentiating Points
1. RBCs in CSF — the single most useful bedside discriminator
"Up to 500 red cells/mm³ are common [in HSE], and the CSF protein content is usually elevated." — Plum & Posner's Diagnosis & Treatment of Stupor and Coma
2. Pleocytosis is variable in both — but more marked in HSE
- HSE: typically 50–200 WBC/µL, can be up to 1,000
- Limbic encephalitis: mild or absent — the CSF can be entirely normal in up to 50% of autoimmune cases
"CSF often demonstrates findings consistent with inflammation (protein >50 mg/dL or lymphocytic pleocytosis >5 cells/µL) but can be normal." — Washington Manual of Medical Therapeutics
3. HSV PCR — definitive test, but timing matters
- Sensitivity 96%, specificity 99% when tested at 48–72 hrs after symptom onset
- Can be falsely negative in the first 24–48 hours — a negative early PCR does NOT rule out HSE
- If strong clinical suspicion + negative PCR < 72 hrs → repeat LP at 72–96 hrs
- Never stop aciclovir based on a single negative early PCR
4. Antibody testing in CSF vs serum
- For autoimmune encephalitis, CSF antibodies are more sensitive than serum for some (e.g., anti-NMDAR)
- Must be sent specifically; not part of routine CSF biochemistry
- Some antibodies (Anti-LGI1, CASPR2) are more reliably detected in serum than CSF
Practical Algorithm
CSF Result
│
├─ RBCs present + lymphocytic pleocytosis + elevated protein
│ → HSE most likely → CONTINUE aciclovir, await PCR
│
├─ Lymphocytic pleocytosis, NO RBCs, normal glucose
│ → HSE still possible (early) OR autoimmune
│ → Send HSV PCR + autoimmune antibody panel
│
└─ Completely NORMAL CSF
→ Does NOT exclude autoimmune limbic encephalitis
→ Does make HSE less likely (but not impossible early)
→ Send serum + CSF antibody panel
Important Caveat — Post-HSE Autoimmune Encephalitis
"Late autoimmune encephalitis can occur 1 to 7 weeks after herpes simplex encephalitis, associated with NMDA-receptor antibodies in the spinal fluid." — Goldman-Cecil Medicine
Images of both and Differential
MRI Images: HSE vs Limbic Encephalitis
🔴 Herpes Simplex Encephalitis (HSE)
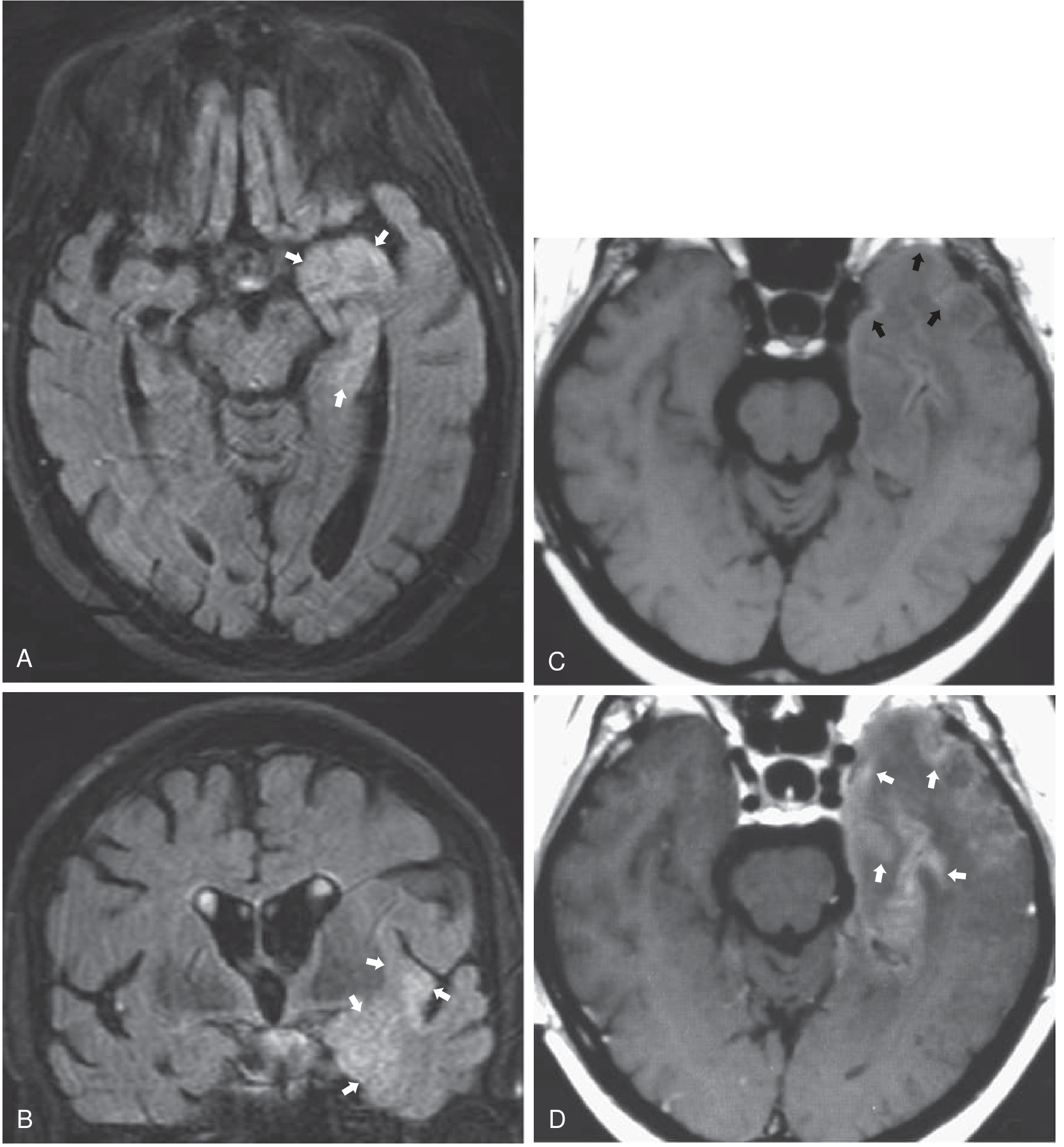
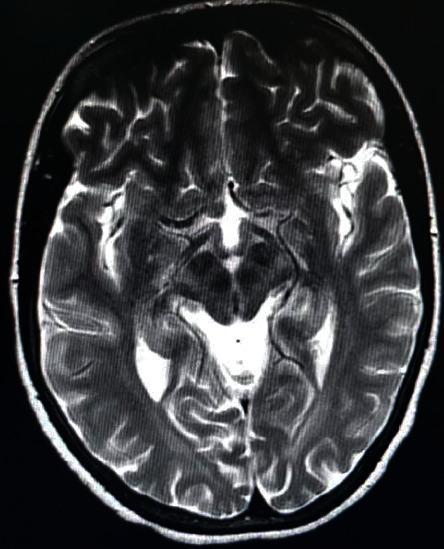
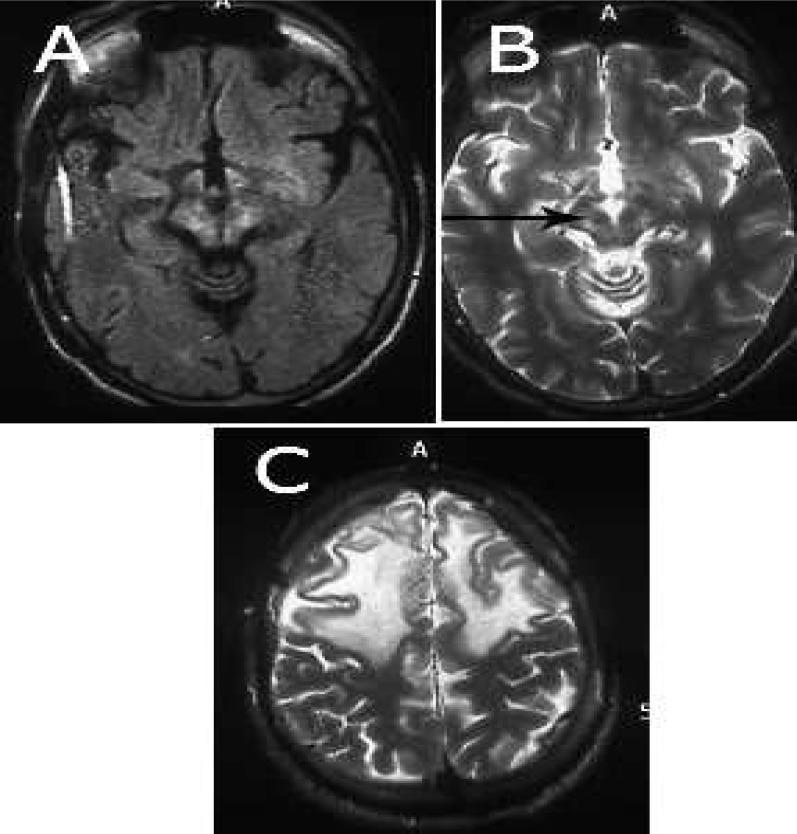
- A & B (Case 1): Axial + coronal FLAIR — hyperintense signal in the left medial temporal lobe and insula (arrows), with cortical swelling. Classic HSE territory.
- C (Case 2): T1 non-contrast — swollen left temporal lobe with faint cortical hyperintensity indicating haemorrhage (black arrows).
- D: T1 post-contrast — gyriform enhancement (white arrows) — a pattern highly suggestive of HSE.
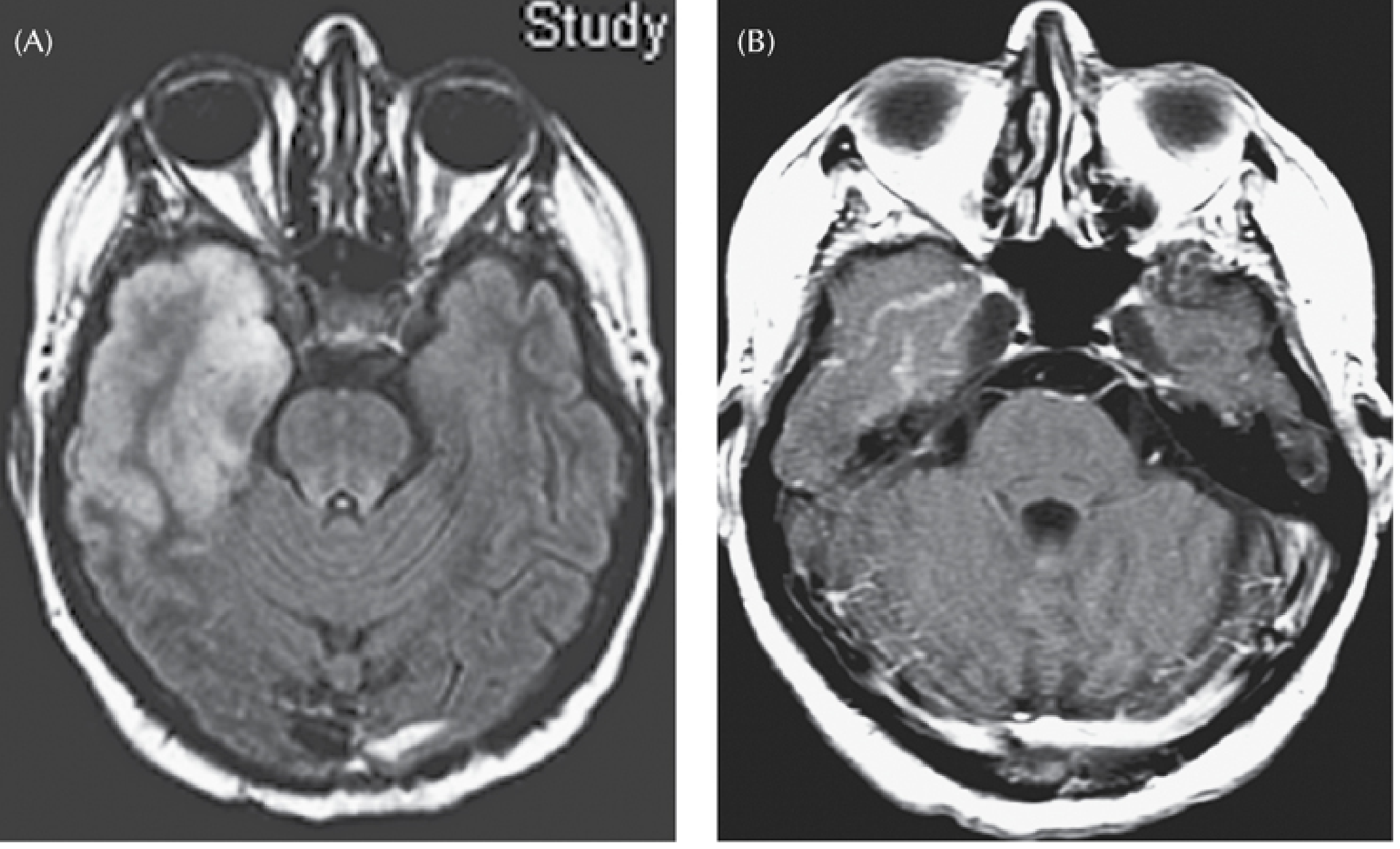
- (A) FLAIR: massive bilateral temporal lobe hyperintensity — confluent and asymmetric, consistent with fulminant HSE. Note the left temporal lobe is more severely affected.
- (B) Post-contrast T1: bilateral enhancement pattern with associated swelling.
Key radiological hallmarks of HSE: medial temporal + insula + cingulate + orbitofrontal involvement; haemorrhagic component; gyriform enhancement; grey matter > white matter.
🟠 Autoimmune / Limbic Encephalitis
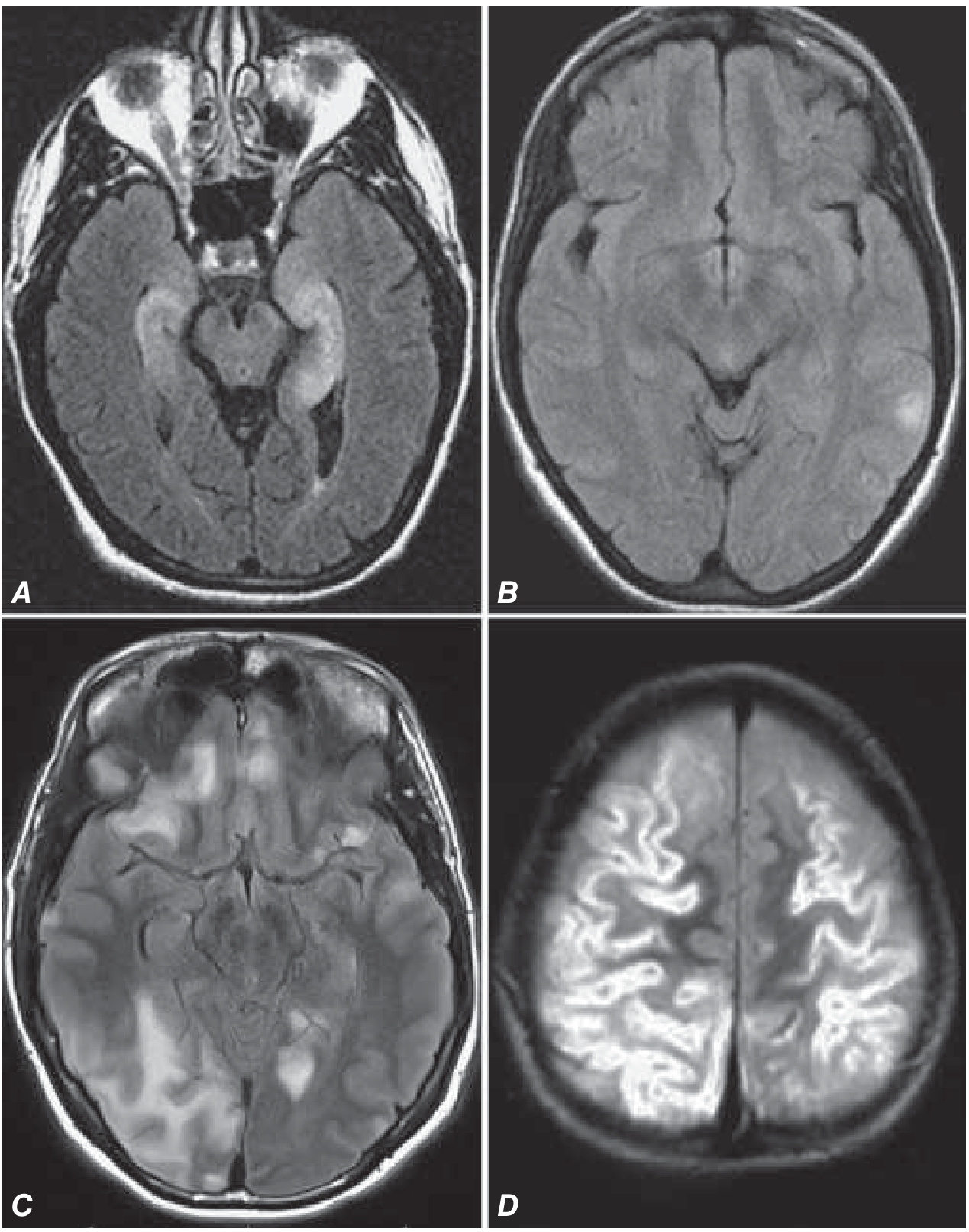
- A — Limbic Encephalitis (anti-Hu, Ma2, AMPAR, GABA-B, LGI1, Caspr2): Bilateral medial temporal lobe FLAIR hyperintensity — confined, symmetric, no haemorrhage, no gyriform enhancement. Clean signal restricted to hippocampus/amygdala.
- B — Anti-NMDAR encephalitis: Often normal MRI or only mild, subtle FLAIR changes — despite severe clinical syndrome.
- C — Anti-GABA-B encephalitis: Multiple cortical-subcortical FLAIR changes, more widespread than classic limbic encephalitis.
- D — MOG-antibody encephalitis (paediatric): Extensive cortical T2 signal, diffuse cortical involvement.
Side-by-Side Differentiating Features on MRI
| Feature | HSE | Autoimmune Limbic Encephalitis |
|---|---|---|
| Distribution | Medial temporal + insula + cingulate + orbitofrontal | Medial temporal only (hippocampus/amygdala) |
| Laterality | Unilateral → bilateral (asymmetric) | Often bilateral and symmetric |
| Haemorrhage | ✅ Frequent — T1 cortical bright spots, blooming on SWI | ❌ Absent |
| Swelling/mass effect | ✅ Marked temporal lobe swelling, can herniate | Mild or none |
| Enhancement | ✅ Gyriform / leptomeningeal (after day 3–5) | ❌ Rarely enhances |
| Grey vs white matter | Grey matter predominant (cortex + hippocampus) | Hippocampus (grey matter, but less cortical spread) |
| DWI restriction | ✅ Common (cortical restricted diffusion early) | Mild or absent |
| Insula involvement | ✅ Characteristic | ❌ Typically spared |
| Progression | Rapid (hours to days) | Subacute (days to weeks) |
| MRI may be normal | ❌ Rarely (very early) | ✅ Up to 50% initially normal |
Memory Hook
HSE = Haemorrhage + Swelling + Enhancement (gyriform) + Insula involved
Limbic Encephalitis = Limited to mesial temporal, Enhancement absent, Bilateral and symmetric
Painfull vision loss causes
Painful Vision Loss — Causes
🔴 Category 1: Eye/Orbital Pain + Vision Loss
1. Acute Angle-Closure Glaucoma
- Most dramatic — excruciating periorbital/frontal pain, nausea, vomiting
- Sudden vision loss + coloured halos around lights
- Signs: red eye, hazy/steamy cornea, mid-dilated non-reactive pupil, rock-hard globe, shallow anterior chamber
- RAPD variable; fundus difficult to visualise due to corneal oedema
- Emergency — requires immediate IOP reduction
"Distinguishing characteristics include the severity of pain (which can be excruciating), presence of visual halos, and an injected eye with an enlarged, nonreactive pupil." — Bradley & Daroff's Neurology
2. Optic Neuritis
- Periorbital/retrobulbar pain, worse on eye movement — in ~90% of cases
- Subacute monocular vision loss over hours–days (nadir at ~1 week)
- RAPD present; colour desaturation (red desaturation earliest finding)
- Young female; strongly associated with MS
- Disc may appear normal (retrobulbar) or swollen (papillitis)
- Pain with eye movement is the clinical hallmark distinguishing it from other causes
3. Anterior Uveitis (Iritis/Iridocyclitis)
- Deep aching eye pain + photophobia + blurred vision
- Ciliary flush (perilimbal injection), cells and flare in anterior chamber, consensual photophobia
- Miosis (not mydriasis)
- Associated with HLA-B27 conditions (AS, reactive arthritis, psoriatic arthritis), sarcoidosis, Behçet's
4. Scleritis
- Severe boring/boring pain — often worst at night, may radiate to face/jaw
- Deep red/violaceous hue (not relieved by topical vasoconstrictors)
- Necrotising scleritis: may cause vision loss through secondary uveal or corneal involvement
- Strongly associated with rheumatoid arthritis, ANCA vasculitis, SLE
5. Endophthalmitis
- Severe pain + profound vision loss + hypopyon
- Post-operative (most common) or endogenous (haematogenous — IV drug users, immunocompromised)
- Vitritis, anterior chamber cells, swollen lids — ocular emergency
6. Corneal Pathology (Ulcer / Keratitis)
- Sharp, surface pain + photophobia + tearing
- Herpes simplex keratitis: dendritic ulcer on fluorescein
- Acanthamoeba keratitis: contact lens wearer, disproportionate pain
- Bacterial corneal ulcer: hypopyon possible
7. Orbital Cellulitis
- Periorbital pain + proptosis + restricted painful eye movements + chemosis
- Vision loss if optic nerve compressed (surgical emergency)
- Fever + signs of sinusitis
- Distinguish from preseptal (periorbital) cellulitis — the latter does not threaten vision
🟠 Category 2: Headache/Retro-orbital Pain + Vision Loss
8. Giant Cell Arteritis (Temporal Arteritis)
- Age >50 (usually >70), female predominance
- Jaw claudication + scalp tenderness + temporal headache — then sudden, profound, painless or mildly painful vision loss
- Ischaemic optic neuropathy: swollen pale disc, RAPD
- Contralateral eye involved in days if untreated
- ESR >50, CRP elevated — start high-dose steroids immediately, before biopsy
9. Pituitary Apoplexy
- Sudden severe headache ("thunderclap") + bitemporal visual field loss + diplopia (CN III palsy)
- Haemorrhage/infarction into pituitary adenoma
- Cavernous sinus involvement → III, IV, VI nerve palsies
10. Cavernous Sinus Thrombosis
- Periorbital pain + proptosis + chemosis + ophthalmoplegia + fever
- Vision loss from optic nerve/retinal vein compromise
- Post-septal spread from sinusitis (sphenoid/ethmoid)
11. Migraine (Retinal/Ocular Migraine)
- Retro-orbital pain + transient monocular vision loss (scintillating scotoma)
- Fully reversible; younger patients; personal/family history of migraine
- Rare but can cause permanent retinal infarction
12. Carotid-Cavernous Fistula
- Pulsatile proptosis + ocular bruit + chemosis + elevated IOP → vision loss
- High-flow (post-traumatic) or low-flow (spontaneous, dural)
🟡 Category 3: Acute Retinal Necrosis / Inflammatory
- Acute Retinal Necrosis (ARN): retinal arteriolar sheathing + peripheral retinal opacification + uveitis + pain
- Caused by VZV (>HSV) in immunocompetent; CMV in immunocompromised
Summary Table
| Cause | Pain Character | Onset | Key Sign | RAPD |
|---|---|---|---|---|
| Acute angle-closure glaucoma | Excruciating periorbital | Sudden | Hazy cornea, mid-dilated pupil, firm globe | +/− |
| Optic neuritis | Retrobulbar, worse on movement | Subacute | Young F, colour desaturation | ✅ Yes |
| Anterior uveitis | Deep ache + photophobia | Subacute | Ciliary flush, cells/flare | ❌ No |
| Scleritis | Boring, nocturnal | Subacute | Violaceous sclera, RA association | Variable |
| Endophthalmitis | Severe | Acute | Hypopyon, post-op/IV drug use | Variable |
| Orbital cellulitis | Periorbital | Acute | Proptosis, restricted EOM, fever | Variable |
| Giant cell arteritis | Temporal headache, jaw claudication | Sudden | Swollen pale disc, ESR↑ | ✅ Yes |
| Pituitary apoplexy | Thunderclap headache | Sudden | Bitemporal hemianopia + CN III palsy | Variable |
| Corneal ulcer/keratitis | Sharp, surface | Acute | Fluorescein staining, dendritic ulcer | ❌ No |
| Migraine | Retro-orbital | Transient | Fully reversible | ❌ No |
Memory Framework
PAINFUL Vision Loss
│
├── Eye pain → ACG, Uveitis, Scleritis, Keratitis, Endophthalmitis, Orbital cellulitis
│
├── Pain on eye movement → OPTIC NEURITIS (MS)
│
└── Headache + pain → GCA, Pituitary apoplexy, Cavernous sinus thrombosis, Migraine
Mild painfully loss of vision 4-5 days without fever trauma seizures Differential
Mild Painful Vision Loss Over 4–5 Days — Differential Diagnosis
The Clinical Profile Points To:
- Subacute onset (days, not seconds/minutes) → excludes vascular (CRAO, AION)
- Pain present → excludes most retinal pathology
- No fever → makes infection/endophthalmitis less likely
- No trauma → excludes traumatic causes
- No seizures → not post-ictal cortical visual loss
- Mild → not fulminant (not angle-closure crisis)
Top Differentials
🥇 1. Optic Neuritis — Most Likely
- Pain: retrobulbar/periorbital, worse on eye movement — present in >90%
- Pain typically precedes or accompanies vision loss and lasts a few days
- Vision loss progresses over several days to 3 weeks, nadir at ~1 week
- Usual VA: 6/18–6/60 (mild to moderate)
- Colour desaturation (red colour looks washed out) — often more impaired than acuity suggests
- RAPD present
- Disc: normal in 2/3 (retrobulbar) OR swollen in 1/3 (papillitis)
- Age 20–50 years, female predominance
"Discomfort or pain in or around the eye is present in over 90% and typically exacerbated by ocular movement. It may precede or accompany the visual loss and usually lasts a few days." — Kanski's Clinical Ophthalmology
| Type | Clue |
|---|---|
| MS-associated (typical) | Young white female, previous neurological episodes |
| NMOSD (anti-AQP4/anti-MOG) | More severe, poor recovery, may be bilateral, non-white |
| Isolated/idiopathic | No systemic disease found |
| Sarcoidosis | Bilateral, uveitis, systemic features |
🥈 2. Anterior Uveitis (Iritis)
- Deep aching eye pain + photophobia + blurred vision over days
- No fever typically in idiopathic/HLA-B27 associated forms
- Ciliary flush (ring of injection around limbus)
- Cells and flare in anterior chamber on slit lamp
- Posterior synechiae (iris stuck to lens)
- Consensual photophobia (shining light in good eye hurts the bad eye)
- Vision loss is usually mild-moderate; rarely severe unless complicated by cataract, macular oedema, or hypopyon
🥉 3. Posterior Uveitis / Intermediate Uveitis
- Less prominent external pain but dull ache + vitreous floaters + blurred vision
- Progressive over days–weeks
- Vitritis on fundoscopy; may see choroidal/retinal lesions
- Causes: sarcoidosis, toxoplasmosis (reactivation), TB, syphilis, idiopathic
4. Scleritis (Posterior)
- Posterior scleritis can be deceptive — less visible redness but significant dull, boring pain, often worse at night or on eye movement
- Proptosis, choroidal effusion, reduced motility, subretinal fluid
- Vision loss from retinal/choroidal involvement
- Associated with RA, vasculitis
"Posterior scleritis is more difficult to diagnose because some patients do not have anterior signs of inflammation." — Rosen's Emergency Medicine
5. Acute Angle-Closure Glaucoma (Subacute/Intermittent form)
- The intermittent/subacute variant presents less dramatically than the acute crisis
- Episodes of mild pain, coloured halos, mildly blurred vision — coming and going over days
- No nausea/vomiting in mild form
- Narrow anterior chamber on exam; IOP elevated during episodes
- Risk: hypermetropes, Asian ethnicity, elderly females, dim-light exposure, mydriatics
6. Corneal Pathology (Keratitis)
- Surface/foreign body pain (sharp, gritty) + photophobia + lacrimation
- Herpes simplex keratitis: recurrent, dendritic ulcer on fluorescein staining
- Vision blurred by corneal oedema/opacity
- No fever unless bacterial superinfection
7. Optic Perineuritis
- Inflammation of the optic nerve sheath (not the nerve itself)
- Pain on eye movement similar to optic neuritis but vision relatively preserved
- Usually idiopathic; also with sarcoidosis, IgG4 disease, GPA
- Disc may be swollen; MRI shows nerve sheath enhancement ("tram-track" sign)
8. Leber's Hereditary Optic Neuropathy (LHON) — Atypical Presentation
- Usually painless, but mild periocular discomfort occasionally reported
- Young male (maternal inheritance), subacute central visual loss
- Typically bilateral (fellow eye affected weeks–months later)
- Central scotoma, disc hyperaemia/pseudoedema in early phase
- If mild pain present: easy to confuse with optic neuritis
Ranked by Probability for This Scenario
| Rank | Diagnosis | Key Discriminating Feature |
|---|---|---|
| 1 | Optic Neuritis | Pain on eye movement, RAPD, colour desaturation, young F |
| 2 | Anterior Uveitis | Ciliary flush, photophobia, cells/flare, no RAPD |
| 3 | Subacute angle-closure glaucoma | Haloes, narrow chamber, IOP spike |
| 4 | Posterior Scleritis | Deep boring pain, proptosis, normal anterior segment |
| 5 | Posterior/Intermediate Uveitis | Floaters, vitritis, no anterior signs |
| 6 | Corneal keratitis | Surface pain, fluorescein staining |
| 7 | Optic Perineuritis | Pain on movement, good acuity, MRI sheath enhancement |
Bedside Examination Steps
- Visual acuity (each eye separately)
- Colour vision (Ishihara — red desaturation in optic neuritis)
- RAPD (swinging torch test) — present in optic neuritis, absent in uveitis
- IOP — elevated in ACG
- Slit lamp — anterior chamber cells/flare (uveitis), corneal staining, depth of anterior chamber
- Fundoscopy — disc swollen (papillitis) vs normal (retrobulbar neuritis) vs vitritis (posterior uveitis)
- Pain on eye movement — strongly suggests optic neuritis
Unilateral hand muscle weakness differentials
Unilateral Hand Muscle Weakness — Differentials
Anatomical Framework
Cortex → Corticospinal tract → Cervical cord (C8/T1 segments)
↓
Anterior horn cell
↓
C8/T1 nerve roots
↓
Lower trunk of brachial plexus
↓
Medial cord → Ulnar nerve
→ Median nerve (partly)
Level 1: Cortical / UMN
Contralateral Cortex / Corticospinal Tract
- Stroke (MCA territory — hand knob area)
- Brain tumour (cortical/subcortical)
- Cortical vein thrombosis
- Multiple sclerosis (cervical cord or cortical lesion)
Level 2: Cervical Cord
C8/T1 Cord Segment
| Cause | Clue |
|---|---|
| Syringomyelia | Bilateral (but can be asymmetric early); suspended sensory loss; dissociation (pain/temp lost, touch preserved) |
| Intramedullary tumour | Progressive, bilateral later; long tract signs below |
| Cervical cord compression | UMN signs in legs + LMN in hands |
| ALS | Mixed UMN + LMN; fasciculations; no sensory loss |
| Anterior spinal artery occlusion | Acute; bilateral; spares dorsal columns |
Level 3: Anterior Horn Cell (LMN Pure)
| Cause | Clue |
|---|---|
| Hirayama Disease (Monomelic Amyotrophy) | Young male (15–25 yrs); unilateral or asymmetric distal arm/hand wasting; hallmark: cold paresis (worsens in cold); self-limiting; MRI shows anterior cord flattening on flexion |
| Progressive Muscular Atrophy (PMA) | Pure LMN MND variant; wasting + fasciculations; no sensory loss |
| ALS (focal onset) | Begins unilateral hand; asymmetric early; eventually bilateral |
| Poliomyelitis / post-polio | History of polio; acute flaccid paralysis; asymmetric |
Level 4: C8/T1 Nerve Root
| Cause | Clue |
|---|---|
| Cervical disc herniation (C7/T1) | Neck pain radiating to medial forearm/4th–5th fingers; C8 radiculopathy |
| Cervical spondylosis (C8/T1 foraminal stenosis) | Older age; chronic; neck stiffness |
| Cervical rib | Young female; medial arm/forearm paresthesia; pulse may be reduced |
| Tumour (metastasis, meningioma) | Progressive; no remission |
Level 5: Brachial Plexus (Lower Trunk / Medial Cord)
| Cause | Clue |
|---|---|
| Pancoast Tumour (superior sulcus tumour) | Shoulder/medial arm pain; Horner's syndrome (ptosis, miosis, anhidrosis); rib destruction on CXR; smoker |
| Neuralgic Amyotrophy (Parsonage-Turner) | Sudden severe shoulder pain → weakness; patchy; any trunk; post-viral/post-vaccination |
| Traumatic lower trunk injury | Klumpke's palsy; birth injury or arm traction |
| Radiation plexopathy | History of radiotherapy to axilla/chest; painless (cf. tumour = painful) |
| Thoracic outlet syndrome (TOS) | Medial arm/hand paresthesia on overhead use; positive Adson's/Roos test |
| Cervical rib | Also compresses lower trunk; young female |
Level 6: Peripheral Nerve
Ulnar Nerve
| Site | Cause |
|---|---|
| Elbow (cubital tunnel — most common) | Prolonged elbow flexion/leaning; numbness 4th–5th fingers; weakness interossei, hypothenar; claw hand (ring + little fingers) |
| Wrist (Guyon's canal) | Deep branch: pure motor (no sensory); superficial branch: pure sensory; hook of hamate fracture |
Median Nerve
| Site | Cause |
|---|---|
| Wrist (Carpal Tunnel Syndrome) | Nocturnal pain/tingling; lateral 3½ fingers; thenar wasting (opponens, abductor pollicis brevis) |
| Anterior Interosseous Nerve (AIN) | Pure motor; no sensory loss; OK sign failure (cannot make O with thumb + index = flexor pollicis longus + FDP to index weakness) |
| Pronator teres syndrome | Proximal median entrapment; all median muscles weak + sensory loss |
Radial Nerve
- Wrist drop (extensor weakness) ± finger drop; sensory loss dorsum hand
- Saturday night palsy (spiral groove), posterior interosseous nerve syndrome (no sensory loss, finger/thumb extension weak)
Summary Localisation Table
| Level | Wasting | Sensory Loss | Reflexes | Extra Clue |
|---|---|---|---|---|
| Cortex/UMN | Late/none | Contralateral | ↑ Brisk, extensor plantar | Spasticity |
| C8/T1 cord | Yes (hand) | Dissociated (cord) | ↓ hands, ↑ legs | Long tract signs in legs |
| Anterior horn | Yes + fasciculations | None | ↓ | Hirayama, ALS |
| C8/T1 root | Yes | Dermatomal (medial forearm, 4–5) | ↓ finger flexors | Neck pain |
| Lower trunk plexus | Yes | Medial forearm + 4–5 | ↓ | Horner's, Pancoast |
| Ulnar nerve | Yes (hypothenar, interossei) | 4–5 digits + medial palm | ↓ finger jerk | Claw hand (ring/little) |
| Median nerve | Yes (thenar) | Lateral 3½ digits | ↓ (if proximal) | Thenar wasting, CTS |
High-Yield Unilateral Causes to Remember
| Diagnosis | Key Feature |
|---|---|
| Hirayama Disease | Young male, cold paresis, self-limiting, MRI diagnostic |
| Pancoast Tumour | Horner's + lower trunk + shoulder pain + smoker |
| Ulnar neuropathy at elbow | Most common peripheral nerve cause; claw hand |
| Carpal tunnel | Thenar wasting; nocturnal symptoms |
| C8 disc herniation | Neck pain + medial forearm sensory loss |
| Neuralgic amyotrophy | Sudden severe pain then patchy weakness |
| ALS (focal onset) | Split-hand pattern; fasciculations; no sensory loss |
| Cervical rib / TOS | Young female; overhead provocation |
Strictly give causes which causes unilateral hand wasting
Causes of Strictly Unilateral Hand Wasting
1. Anterior Horn Cell
| Cause | Why Unilateral |
|---|---|
| Hirayama Disease (Monomelic Amyotrophy) | Hallmark — unilateral or markedly asymmetric wasting of C7–T1 muscles; young male 15–25 yrs; cold paresis; self-limiting at 3–5 yrs |
| ALS / PMA (focal onset) | Often begins strictly unilateral hand ("split-hand" pattern — thenar > hypothenar wasting); fasciculations; no sensory loss |
| Poliomyelitis / Post-polio | Asymmetric flaccid wasting; childhood history |
| Spinal cord tumour (intramedullary, eccentric) | Unilateral anterior horn cell compression |
| Syringomyelia (early/asymmetric) | Can be unilateral early before crossing midline |
2. C8/T1 Nerve Root (Radiculopathy)
| Cause | Clue |
|---|---|
| Cervical disc herniation C7–T1 | Neck/medial arm pain; dermatomal sensory loss 4th–5th fingers |
| Cervical spondylosis (foraminal stenosis) | Older age; unilateral C8/T1 root compression |
| Cervical rib | Young female; subclavian artery compression; positive Adson's |
| Tumour / metastasis at C8/T1 | Progressive; no remission |
3. Brachial Plexus — Lower Trunk / Medial Cord
| Cause | Clue |
|---|---|
| Pancoast Tumour | Horner's syndrome + shoulder/medial arm pain + smoker; chest X-ray shows apical opacity |
| Klumpke's Palsy (traumatic) | Traction injury to lower trunk (arm pulled upward); claw hand + Horner's |
| Neuralgic Amyotrophy (Parsonage-Turner) | Sudden severe pain → wasting; patchy; one limb; post-viral |
| Radiation plexopathy | Post-radiotherapy; painless wasting; history of breast/lung cancer treatment |
| Thoracic Outlet Syndrome | Neurogenic TOS — lower trunk compression; medial forearm + hand intrinsic wasting |
| Cervical rib (neurogenic) | Lower trunk compression; medial forearm sensory loss |
4. Peripheral Nerve
| Nerve | Cause | Wasting Pattern |
|---|---|---|
| Ulnar nerve (elbow — cubital tunnel) | Prolonged elbow flexion; leaning on elbow | Hypothenar + interossei + 4th/5th lumbrical wasting; claw hand |
| Ulnar nerve (wrist — Guyon's canal) | Ganglion, hook of hamate fracture, cyclist's palsy | Hypothenar ± interossei depending on branch |
| Median nerve (wrist — CTS) | Repetitive strain, hypothyroidism, pregnancy, RA | Thenar wasting (APB, opponens) |
| Median nerve (AIN — pure motor) | No wasting of intrinsics but FPL/FDP wasting | |
| Combined ulnar + median | Leprosy (unilateral early), vasculitis, deep laceration | Pan-intrinsic wasting — "main en griffe" |
5. Disuse Atrophy (Non-neurological)
| Cause | Clue |
|---|---|
| Rheumatoid Arthritis (unilateral early) | Dorsal interosseous wasting from disuse + joint destruction; usually bilateral eventually |
| Immobilisation / cast | History of prolonged immobilisation |
| Complex Regional Pain Syndrome (CRPS) | Post-injury; trophic changes; allodynia |
Memory Scaffold
UNILATERAL hand wasting — level by level:
CORD: Hirayama ← young male, most important cause
Syringomyelia (early/asymmetric)
ALS focal onset
ROOT (C8/T1): Cervical disc C7-T1
Cervical spondylosis
Cervical rib
PLEXUS: Pancoast (+ Horner's)
Klumpke's (trauma)
Neuralgic amyotrophy
Radiation plexopathy
TOS / cervical rib
NERVE: Ulnar (elbow > wrist) → hypothenar/interossei
Median (CTS) → thenar only
Leprosy → combined
The Single Most Important Discriminator
- No sensory loss → anterior horn cell (Hirayama, ALS, PMA, polio)
- Medial forearm + 4/5 fingers → lower trunk plexus or C8 root (Pancoast, disc, cervical rib)
- 4/5 fingers only (no forearm) → ulnar nerve at wrist
- Lateral 3½ fingers → median nerve (CTS)
- Dissociated (pain/temp lost, touch preserved) → cord (syringomyelia)
Leprosy types and clinical features , hand wasting , facies diagnosis treatment lepra reaction all related to leprosy in crisp
Leprosy (Hansen's Disease) — Complete Crisp Summary
Classification
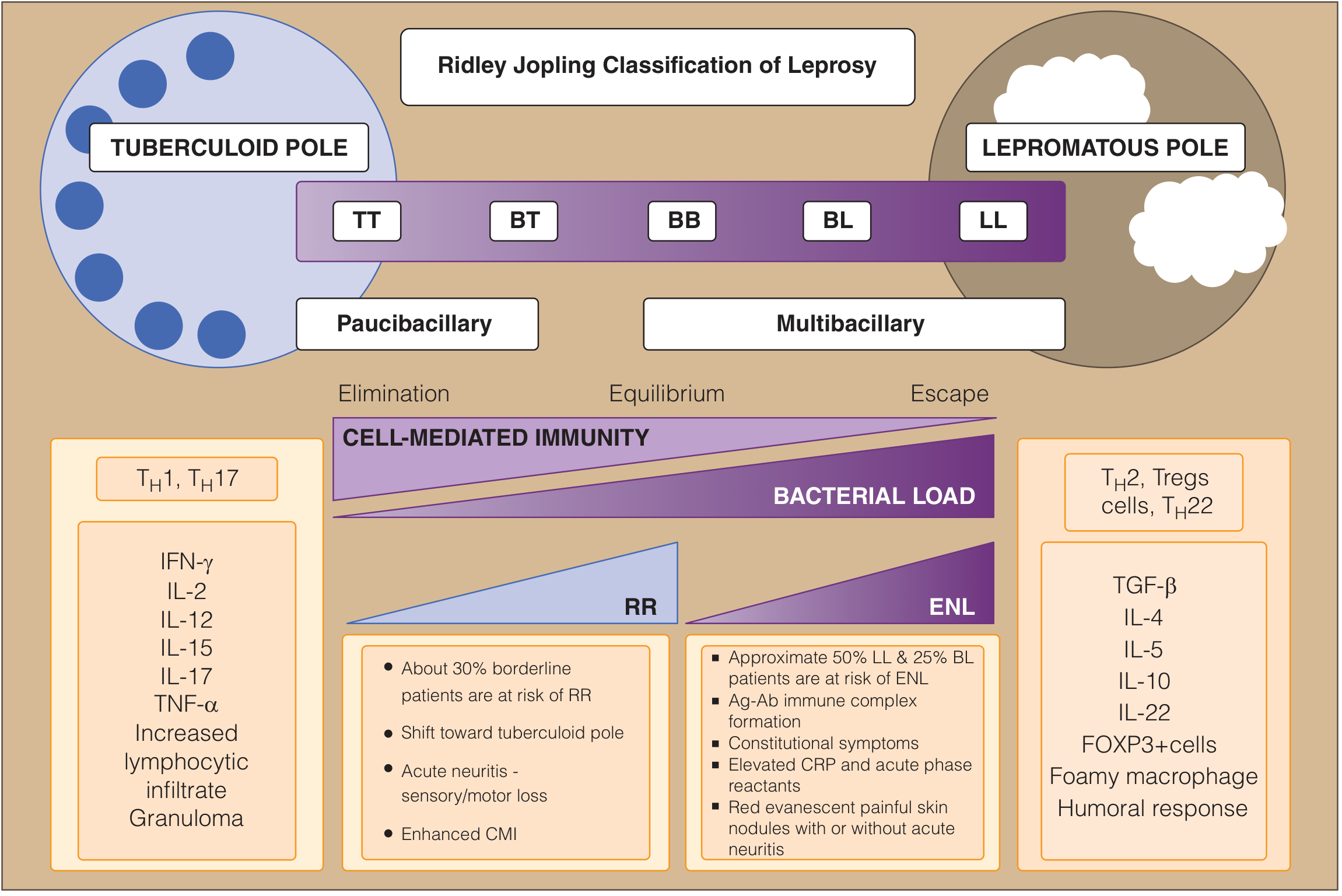
| TT | BT | BB | BL | LL | |
|---|---|---|---|---|---|
| Skin lesions | 1–3 | Up to 10 | 10–30 | Many >30, asymmetric | Innumerable, symmetric |
| Lesion type | Well-defined erythematous plaque, dry, scaly | Similar to TT, slightly less defined | Intermediate | Multiple, less defined | Diffuse infiltration, nodules, plaques |
| Sensation in lesion | Anaesthetic | Reduced | Variable | Mildly reduced | Near normal initially |
| Nerve thickening | Single, marked | Few | Multiple | Multiple | Multiple, mild |
| Bacteriological Index (BI) | 0 | 0–1+ | 2+ | 3–4+ | 5–6+ |
| Lepromin test | +++ | ++ | +/− | − | − |
| Stability | Stable | May upgrade/downgrade | Unstable | Downgrade tendency | Stable |
- Paucibacillary (PB) = 1–5 lesions, no bacilli on smear → TT + BT
- Multibacillary (MB) = >5 lesions OR nerve trunk involvement OR bacilli on smear → BB + BL + LL
Clinical Features by Type
Tuberculoid Leprosy (TT)
- 1–3 well-defined hypopigmented or erythematous plaques
- Raised edges sloping inward (punched-out appearance)
- Skin: dry, scaly, anhidrotic, anaesthetic, hairless
- One peripheral nerve thickened (commonly ulnar)
- Good prognosis; self-limiting in some
Lepromatous Leprosy (LL)
- Innumerable, symmetric, poorly defined lesions — macules, papules, nodules
- Skin: shiny, "succulent" texture
- Leonine facies — diffuse facial skin infiltration, thickened ear lobes, nodules (see image below)
- Madarosis — loss of lateral eyebrows and eyelashes
- Nasal involvement — saddle nose deformity, epistaxis, nasal stuffiness
- Gynecomastia, testicular atrophy, sterility (in males)
- Lagophthalmos — inability to close eyelids → corneal exposure → blindness
- Bilateral, symmetric peripheral neuropathy (both sensory and motor)
- High bacterial load — smear teeming with acid-fast bacilli
Facies of Leprosy
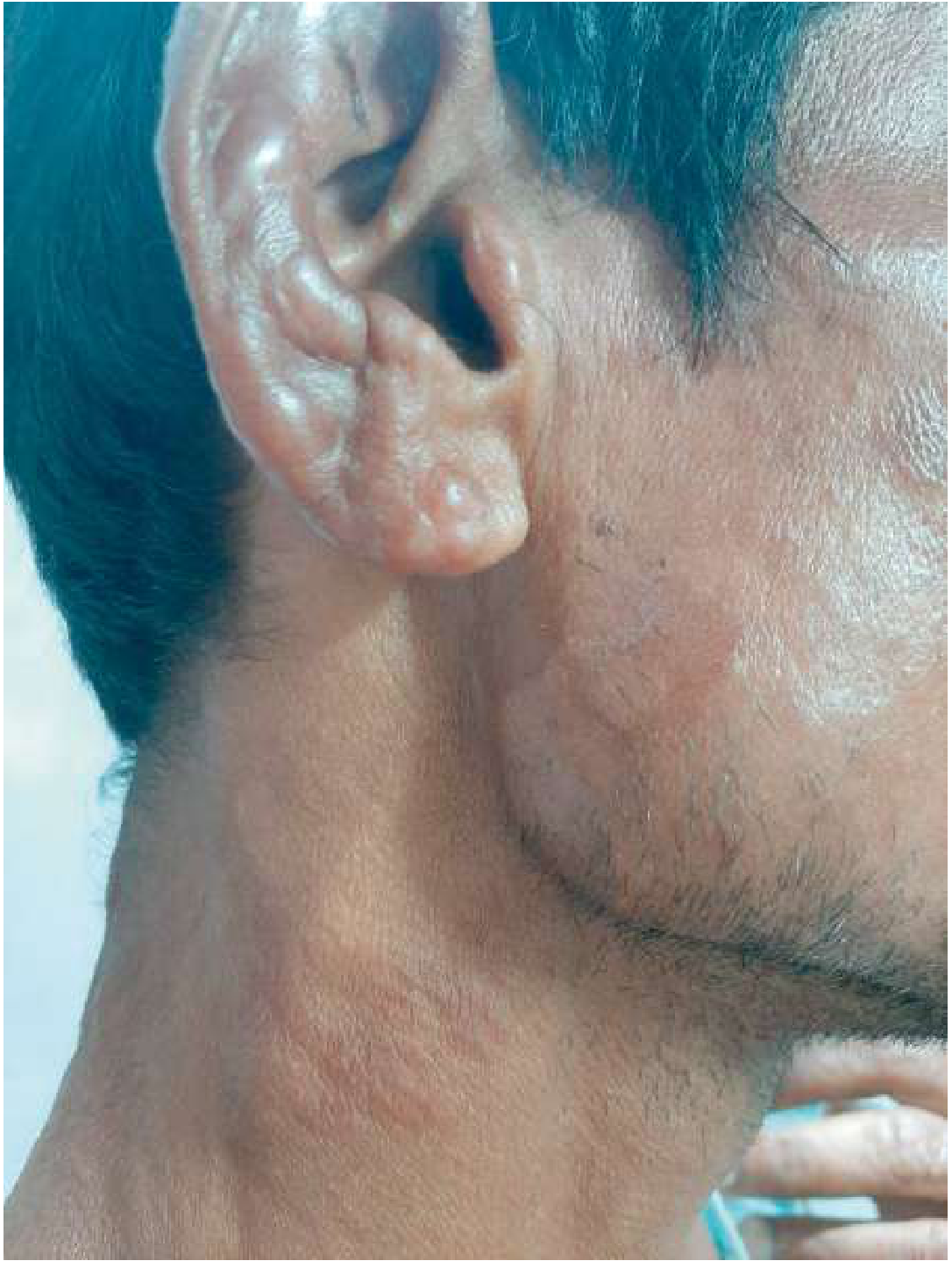

- Diffuse facial infiltration → skin folds deepened → lion-like face
- Earlobe nodules (pathognomonic — earlobe hangs low, succulent)
- Madarosis — loss of lateral eyebrows (outer 1/3 first)
- Saddle-nose deformity (nasal cartilage collapse)
- Supraorbital ridging
- Lagophthalmos → corneal exposure → blindness
- Greater auricular nerve visible/palpable as thickened cord
Hand Wasting in Leprosy
Nerves Commonly Affected
| Nerve | Entrapment Site | Result |
|---|---|---|
| Ulnar nerve (most common) | Medial epicondyle | Hypothenar + interossei wasting → Claw hand (ring + little fingers) |
| Median nerve | Carpal tunnel | Thenar wasting → simian/ape hand (flattened thenar eminence) |
| Both ulnar + median | Combined | Pan-intrinsic wasting — "main en griffe" (all fingers clawed) |
| Radial nerve (less common) | Spiral groove / wrist drop | Extensor weakness |
Hand Deformities
- Claw hand (Griffe) — ulnar claw (4th/5th fingers clawed due to interossei weakness)
- Ape/simian hand — thenar flat, thumb adducted (median nerve)
- Drop wrist — radial nerve
- Trophic ulcers — anaesthetic palm + pressure + trauma → perforating ulcers
- Absorption of digits — longstanding untreated LL — bones resorb
- Lagophthalmos from facial nerve involvement
Diagnosis
Cardinal Signs (any ONE = diagnose leprosy)
- Hypopigmented/erythematous skin lesion with loss of sensation
- Thickened peripheral nerve (ulnar, common peroneal, great auricular, posterior tibial, radial cutaneous, supra-orbital, facial nerve)
- Acid-fast bacilli (AFB) in slit-skin smear
Investigations
| Test | Purpose |
|---|---|
| Slit-skin smear (AFB, Ziehl-Neelsen) | BI (Bacteriological Index) and MI (Morphological Index); positive in MB leprosy |
| Lepromin (Mitsuda) test | Measures CMI; positive TT, negative LL; NOT diagnostic but helps classify |
| Skin biopsy | Granulomas in TT; foamy macrophages (Virchow cells) in LL; histology confirms |
| PCR | Detects M. leprae DNA; useful in seronegative or paucibacillary |
| ELISA (anti-PGL-1 antibodies) | Elevated in MB leprosy; supports diagnosis |
| Nerve conduction studies | Assess nerve damage extent |
Lepra Reactions (Immunological Emergencies)
Type 1 Reaction — Reversal Reaction (RR)
- Occurs in borderline types (BT, BB, BL)
- Sudden upgrade in cell-mediated immunity
- Existing lesions become acutely inflamed — erythematous, oedematous, warm, may ulcerate
- Neuritis — acute painful nerve swelling → may cause sudden motor/sensory loss
- Triggered by: pregnancy, MDT, infections, stress
- Treatment: Prednisolone 40–60 mg/day, tapered over 3–6 months; MDT continued
Type 2 Reaction — Erythema Nodosum Leprosum (ENL)
- Occurs in LL and BL (multibacillary, high antigen load)
- Immune complex (Type III hypersensitivity) — Ag-Ab complexes, complement activation
- New painful red nodules (not pre-existing lesions) over face, limbs, trunk
- Systemic features: fever, malaise, lymphadenopathy, iridocyclitis, orchitis, arthritis, neuritis, nephritis
- Treatment: Thalidomide (drug of choice — 100–400 mg/day; teratogenic — not in women of childbearing age) OR prednisolone; MDT continued
- Clofazimine also has anti-ENL activity (used for chronic/recurrent ENL)
Comparison
| Feature | Type 1 (RR) | Type 2 (ENL) |
|---|---|---|
| Type | Borderline (BT/BB/BL) | LL/BL |
| Immunology | CMI upregulation (Type IV) | Immune complex (Type III) |
| Lesions | Existing lesions inflame | New nodules appear |
| Fever | Absent or mild | Prominent |
| Neuritis | Common, severe | Yes, but less acute |
| Systemic | No | Yes (eyes, testes, kidneys) |
| Treatment | Prednisolone | Thalidomide or Prednisolone |
Treatment — WHO MDT Regimens
Paucibacillary (PB) — 1–5 lesions
| Drug | Dose | Schedule |
|---|---|---|
| Rifampicin | 600 mg | Monthly supervised |
| Dapsone | 100 mg | Daily self-administered |
| Duration: 6 months |
Multibacillary (MB) — >5 lesions or nerve involvement
| Drug | Dose | Schedule |
|---|---|---|
| Rifampicin | 600 mg | Monthly supervised |
| Dapsone | 100 mg | Daily |
| Clofazimine | 300 mg monthly + 50 mg daily | Monthly (supervised) + daily |
| Duration: 12 months |
Drug Side Effects
| Drug | Key Side Effect |
|---|---|
| Rifampicin | Red-orange urine/secretions; hepatitis; enzyme inducer (reduces OCP efficacy) |
| Dapsone | Haemolysis (especially G6PD deficiency); methaemoglobinaemia; Dapsone hypersensitivity syndrome (fever, rash, hepatitis at 4–6 weeks) |
| Clofazimine | Orange-brown skin/mucosa discolouration (reversible); crystal enteropathy at high dose |
Memory Framework
LEPROSY
Spectrum: TT ←→ BT ←→ BB ←→ BL ←→ LL
↑ CMI ↓ CMI
Paucibacillary Multibacillary
Diagnosis = ANY 1 of 3 cardinal signs
Hand: Ulnar → claw hand (4,5)
Median → ape hand (thenar flat)
Both → pan-intrinsic wasting
Facies: LL = Leonine + Madarosis + Earlobe nodules + Saddle nose
Reactions:
Type 1 (RR) = Borderline → existing lesions inflame → Steroids
Type 2 (ENL) = LL/BL → new painful red nodules + systemic → Thalidomide
MDT:
PB = Rifampicin + Dapsone × 6 months
MB = Rifampicin + Dapsone + Clofazimine × 12 months
Wilson disease mri and Differential and KF ring and clinical features with rx and high yeild points to be asked in neurology viva in crisp
Wilson disease MRI basal ganglia T2 hyperintensity panda sign
Wilson's Disease — Complete Neurology Viva Guide
1. Basics (Viva Opener)
| Gene | ATP7B — chromosome 13q14 |
| Protein | Copper-transporting P-type ATPase |
| Inheritance | Autosomal recessive |
| Defect | Failure of hepatic biliary copper excretion → copper accumulates in liver → spills into blood → deposits in brain, eye, kidney, joints |
| Eponym | "Hepatolenticular Degeneration" — S.A.K. Wilson, 1912 |
| Age of onset | Liver disease: <30 yrs; Neurological: 1st–5th decade |
2. Clinical Features
Neurological (40–50% present neurologically first)
- Tremor — "wing-beating tremor" (coarse, proximal, intention tremor with arms outstretched)
- Dysarthria — often the first sign; slurred, scanning speech
- Dystonia — generalised or focal; grimacing, abnormal postures
- Rigidity — Parkinsonian type
- Chorea / athetosis
- Dysphagia
- Gait ataxia
- Seizures (rare)
Psychiatric (20% present psychiatrically)
- Personality change (irritability, aggression)
- Depression, anxiety
- Psychosis (rare)
- Declining school/work performance in adolescents
Hepatic
- Jaundice, hepatomegaly, splenomegaly
- Chronic hepatitis → cirrhosis
- Acute liver failure with Coombs-negative haemolytic anaemia — classic/emergency presentation
Systemic
- Renal: Fanconi syndrome — aminoaciduria, phosphaturia, haematuria, nephrolithiasis
- Haematological: Coombs-negative haemolytic anaemia (copper → RBC oxidative damage)
- Musculoskeletal: osteoporosis, arthritis (large joints), rickets
- Endocrine: amenorrhoea, infertility, hypoparathyroidism
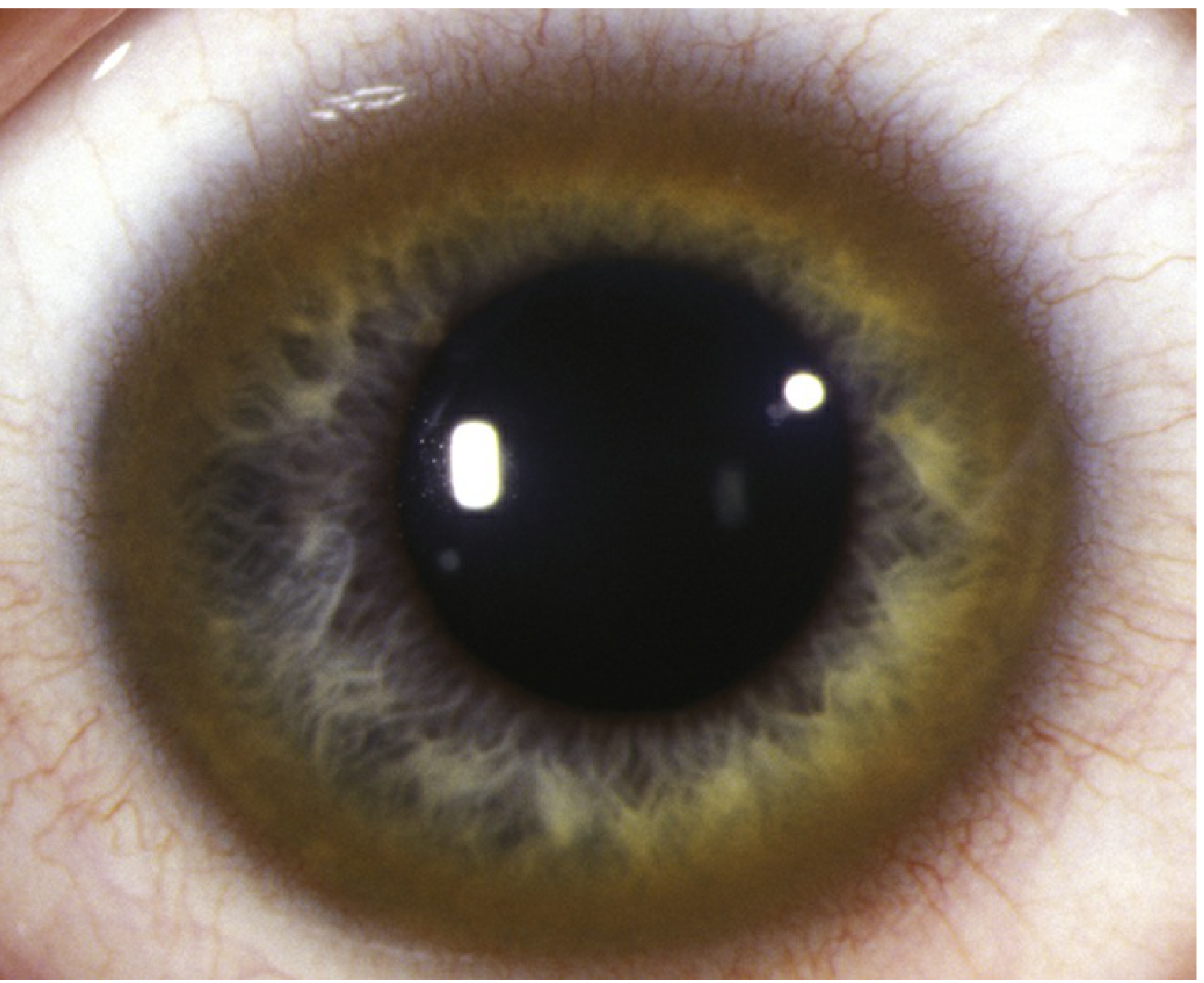
3. Kayser-Fleischer (KF) Ring
| Feature | Detail |
|---|---|
| What is it | Copper (cupruric) deposits in Descemet's membrane of cornea periphery |
| Colour | Golden-brown to greenish-yellow ring |
| Location | Starts at superior limbus → inferior → circumferential |
| Detection | Slit-lamp examination mandatory — rarely visible to naked eye |
| Present in | 95% of neurological WD; only 60% of hepatic WD; ~50% of asymptomatic |
| Absent in | 40–60% with pure hepatic disease; 5% of neurological WD |
| NOT specific | Also in PBC, PSC, other cholestatic liver diseases (rare) |
| Reverses with | Chelation therapy |
| Sunflower cataract | Copper in lens — does not affect vision; also reverses with treatment |
"Most patients with a neurologic or psychiatric presentation of Wilson disease have Kayser-Fleischer rings; only 5% do not." — Sleisenger & Fordtran
4. MRI of Wilson's Disease
Image 1 — Full spectrum of basal ganglia and brainstem changes:
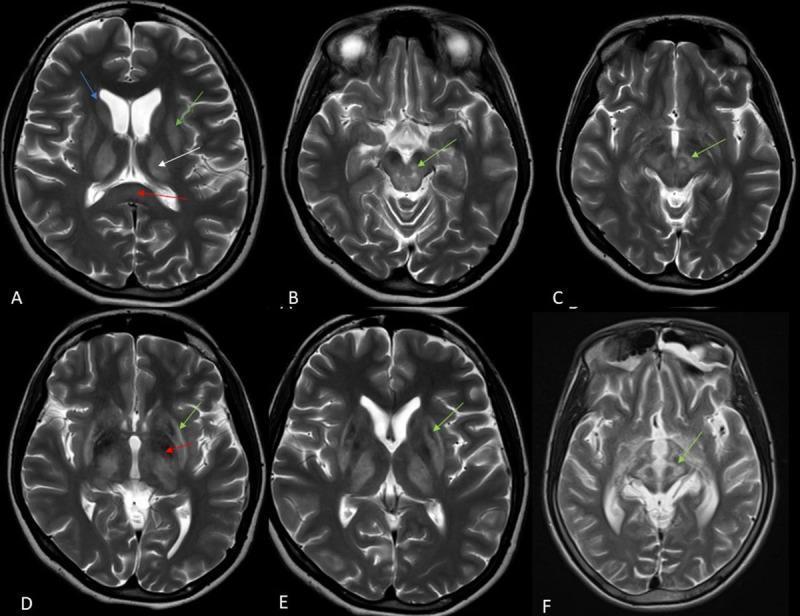
Image 2 — Midbrain signs and pontine involvement:
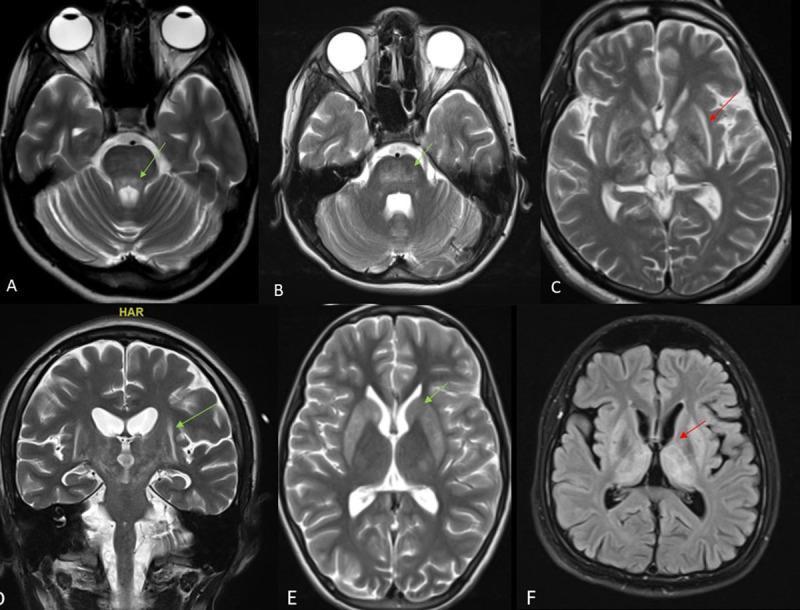
MRI Findings — Summary
| Structure | Signal | Sign |
|---|---|---|
| Putamen | T2 hyperintensity (bilateral) | Most common finding |
| Caudate | T2 hyperintensity | Bilateral |
| Thalamus | T2 hyperintensity | |
| Globus pallidus | T2 hypointensity (copper/iron deposition) | |
| Midbrain tegmentum | T2 hyperintensity with sparing of red nuclei + substantia nigra | "Face of Giant Panda" sign — pathognomonic |
| Pons | Hyperintensity in tegmentum, sparing CST | "Face of Panda Cub" sign |
| Claustrum | T2 hyperintensity | "Bright Claustrum" sign — highly specific |
| Corpus callosum (splenium) | T2 hyperintensity | |
| White matter | Diffuse leukoencephalopathy | Severe disease |
MRI Hallmarks — Viva Points
- T2 hyperintensity in putamen = most common MRI finding in Wilson's
- "Face of Giant Panda" sign = T2 hyperintense midbrain tegmentum + dark red nuclei (eyes) + dark substantia nigra pars reticulata (ears) = pathognomonic for Wilson's
- T1 hyperintensity in basal ganglia = seen in some cases (copper/manganese deposition)
- MRI abnormalities may partially/fully reverse with treatment
5. Differential Diagnosis
For Bilateral Basal Ganglia T2 Hyperintensity
| Condition | Clue |
|---|---|
| Wilson's Disease | Young, liver disease, KF ring, low ceruloplasmin |
| Leigh Syndrome | Infant/child, mitochondrial, periventricular lesions, lactic acidosis |
| NBIA (Neurodegeneration with Brain Iron Accumulation) | "Eye of tiger" sign in globus pallidus (T2 central hyperintensity in hypointense GP) |
| Manganism | Industrial exposure; T1 hyperintensity GP + putamen |
| Carbon monoxide poisoning | History of exposure; GP involvement bilaterally |
| Hypoxic-ischaemic | Context; diffuse cortical + basal ganglia changes |
| Huntington's Disease | Caudate atrophy, chorea, family history |
| Glutaric Aciduria Type 1 | Striatal degeneration, macrocephaly, child |
For Young-Onset Movement Disorder + Liver Disease
- Wilson's (AR, copper), Niemann-Pick type C (NPC1/NPC2, sphingomyelinase), Gaucher disease, Westphal variant Huntington's (rigid juvenile), NBIA
6. Diagnosis
Leipzig Scoring System (Viva must-know)
| Finding | Score |
|---|---|
| KF rings present | +2 |
| Neuropsychiatric symptoms | +2 |
| Serum ceruloplasmin <0.1 g/L | +4; 0.1–0.2 g/L = +1 |
| Coombs-negative haemolytic anaemia | +1 |
| 24-hr urine copper >2× ULN | +2; 1–2× ULN = +1 |
| Liver copper >5× ULN (biopsy) | +2; 0.8–4× = +1 |
| Pathogenic ATP7B mutations (both alleles) | +4; one allele = +1 |
Key Lab Values
| Test | Normal | Wilson's |
|---|---|---|
| Serum ceruloplasmin | 20–35 mg/dL | <20 mg/dL (often <10) |
| Serum copper | 70–140 µg/dL | Low (most copper unbound) |
| 24-hr urinary copper | <40 µg/day | >100 µg/day (symptomatic); >40 µg/day (asymptomatic) |
| Hepatic copper (biopsy) | 20–50 µg/g dry wt | >250 µg/g dry wt |
| Serum ALT/AST | Normal | Elevated (AST > ALT) |
Trick question: Serum ceruloplasmin can be normal in acute liver failure (acute phase reactant) and low in normal neonates — do not use alone
7. Treatment
Chelating Agents (First-Line for Symptomatic)
| Drug | Mechanism | Dose | Key Points |
|---|---|---|---|
| D-Penicillamine | Chelates copper → urinary excretion | 250 mg BD → 15–20 mg/kg/day | Add pyridoxine (B6). Paradoxical worsening of neurological symptoms in 10–50%. Hypersensitivity, nephrotoxicity, elastosis perforans serpiginosa, haematological toxicity |
| Trientine | Chelates copper → urinary excretion | 750–2000 mg/day | Less side effects than penicillamine; preferred if penicillamine intolerance |
| Tetrathiomolybdate | Tripartite complex: copper-albumin-drug | Experimental | Fastest acting; preferred for neurological presentations |
Zinc Acetate (Maintenance / Presymptomatic)
- Mechanism: Induces metallothionein in intestinal cells → blocks copper absorption → copper lost in faeces
- Uses: Presymptomatic patients, maintenance after initial chelation, pregnancy (safest in pregnancy)
- Dose: 50 mg elemental zinc TDS
- Side effect: Dyspepsia; risk of hepatic decompensation if used as sole initial therapy
- Takes 4–6 months to achieve copper balance
Liver Transplant
- Indicated: Acute liver failure unresponsive to medical therapy; end-stage cirrhosis
- Corrects both hepatic failure AND neurological disease (provides normal ATP7B enzyme)
Dietary Restriction
- Avoid: shellfish, liver, nuts, chocolate, mushrooms, drinking water with copper >1.3 mg/L
Treatment is lifelong — stopping causes relapse and liver failure
8. High-Yield Viva Questions
250 µg/g dry weight (normal 20–50 µg/g)
Explain mris of wilson
Wilson's Disease MRI — Full Explanation
Image 1 — Axial T2: Bilateral Basal Ganglia Hyperintensity (Most Common Finding)
- Bright (hyperintense) caudate nuclei bilaterally — the curved structures flanking the lateral ventricles
- Bright putamen bilaterally — the lateral part of the lentiform nucleus
- Bright thalami bilaterally
- Midbrain tegmentum bright — the region around the aqueduct
- No mass effect — this is not oedema from a tumour, it is diffuse copper-induced cytotoxic injury and gliosis
Image 2 — The Three Classic MRI Signs Together
- Symmetrical bright signal in bilateral thalami, basal ganglia and dorsal mesencephalon (midbrain)
- FLAIR suppresses CSF — so the bright areas here are genuine parenchymal signal, not CSF
- This confirms bilateral deep grey matter involvement — characteristic of Wilson's
- Bright background = T2 hyperintense midbrain tegmentum (the region of copper/gliosis)
- Dark dots in the centre = red nuclei — they appear DARK because they are relatively spared and contain iron normally → form the "eyes" of the panda
- Dark outline laterally = substantia nigra pars reticulata → forms the "ears"
- Dark region inferiorly = superior colliculi → forms the "mouth"
- Net result: the midbrain looks like a panda's face → pathognomonic for Wilson's disease
- Bilateral frontal > parietal white matter hyperintensity — diffuse leukoencephalopathy in severe/late Wilson's
- This reflects demyelination and gliosis from copper toxicity spreading into white matter tracts
Image 3 — Giant Panda Sign Close-up (Single Axial T2 at Midbrain Level)

- Level: midbrain at the level of the superior colliculi
- You can see the bright (white) tegmentum surrounding the central structures
- The dark red nuclei (round, symmetrical, flanking the midline) = the panda's eyes
- The dark substantia nigra laterally = the panda's ears
- The whole midbrain takes on a face-shaped appearance at this level
Image 4 — Full Series: All Six Wilson's MRI Patterns
- Blue arrow → caudate nucleus bright
- Green arrows → putamen bright bilaterally
- White arrow → splenium of corpus callosum bright (copper deposits in posterior commissural fibres)
- Red arrow → thalamus bright
- Green arrows → midbrain tegmentum hyperintensity bilaterally at different cuts through the midbrain
- The relative dark regions (red nuclei) can be identified against this bright background
- Green arrow → "Bright claustrum" sign — the claustrum (a thin grey matter layer lateral to the putamen and medial to the insula) appears bright; this is highly specific for Wilson's disease
- Red asterisk → T2-hypointense globus pallidus — in contrast to the hyperintense putamen/caudate; GP hypointensity = heavy iron/copper mineralisation (copper itself is diamagnetic but associated iron causes T2 shortening)
- Green arrow → Classic "central hypointensity surrounded by hyperintensity" in putamen
- This "eye within eye" or "target" pattern reflects: outer ring = gliosis/oedema (bright) + inner core = copper/iron deposition (dark)
- Green arrow → Face of Giant Panda sign — clearest demonstration, with bright tegmentum and dark central structures forming the face pattern
Image 5 — Pontine Signs: Face of Panda Cub + Trident Sign
- "Face of Panda Cub" sign — T2 hyperintensity in pontine tegmentum with relative sparing of the central tegmental tracts (which appear dark) → smaller panda face at pons level
- "Trident sign" — T2 hyperintensity in the basis pontis in a trident shape, sparing the corticospinal tracts
Summary: Wilson's MRI Signs in Order of Importance
| Sign | Location | Appearance | Significance |
|---|---|---|---|
| Face of Giant Panda | Midbrain | Bright tegmentum + dark red nuclei (eyes) + dark SN (ears) | Pathognomonic |
| Face of Panda Cub | Pons | Bright tegmentum + dark central tegmental tracts | Highly specific |
| Bright Claustrum | Claustrum (lateral to putamen) | T2 bright linear structure | Highly specific |
| Bilateral putamen T2 hyperintensity | Putamen | Bright bilateral | Most common finding |
| Target sign in putamen | Putamen | Dark centre + bright rim | Copper core + gliotic rim |
| Thalamus hyperintensity | Thalami | Bilateral bright | Common |
| Globus pallidus hypointensity | GP | Dark (T2) | Mineralisation (iron/copper) |
| Splenium involvement | Corpus callosum | Bright | White matter extension |
| Leukoencephalopathy | Frontal white matter | Diffuse bilateral bright | Severe/late disease |
| Trident sign | Pons | Bright basis pontis, sparing CST | Specific |
Why Do Different Structures Show Different Signals?
| Mechanism | Result on MRI |
|---|---|
| Copper deposition → cytotoxic oedema → gliosis | T2 bright (increased water) |
| Copper + secondary iron mineralisation in GP | T2 dark (paramagnetic effect) |
| Neuronal loss + cavitation | T2 bright (fluid-filled spaces) |
| Recovery with chelation | Partial/complete signal normalisation |
Define epilepsy seizure convulsion status epilepsy