Describe clinical presentation and Physiotherapy Management in Radial Nerve injury
Reading File
Finding Sources
Finding Sources
Searching PubMed
"radial nerve" injury rehabilitation physiotherapy
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full detailed answer.
Radial Nerve Injury: Clinical Presentation and Physiotherapy Management
Anatomy Recap (Basis for Clinical Features)
The radial nerve (C5-C8, T1) is the largest terminal branch of the posterior cord of the brachial plexus. Its key anatomical relationships determine the clinical picture at each level of injury:
- Axilla: gives branches to triceps, posterior cutaneous nerve of arm
- Spiral groove (radial groove) of humerus: most vulnerable point - innervates brachioradialis and ECRL before passing anteriorly
- Lateral to humerus / anterior to lateral epicondyle: ECRB, supinator
- Within radial tunnel, divides into two terminal branches:
- Posterior interosseous nerve (PIN) - pure motor, innervates all remaining wrist and finger extensors
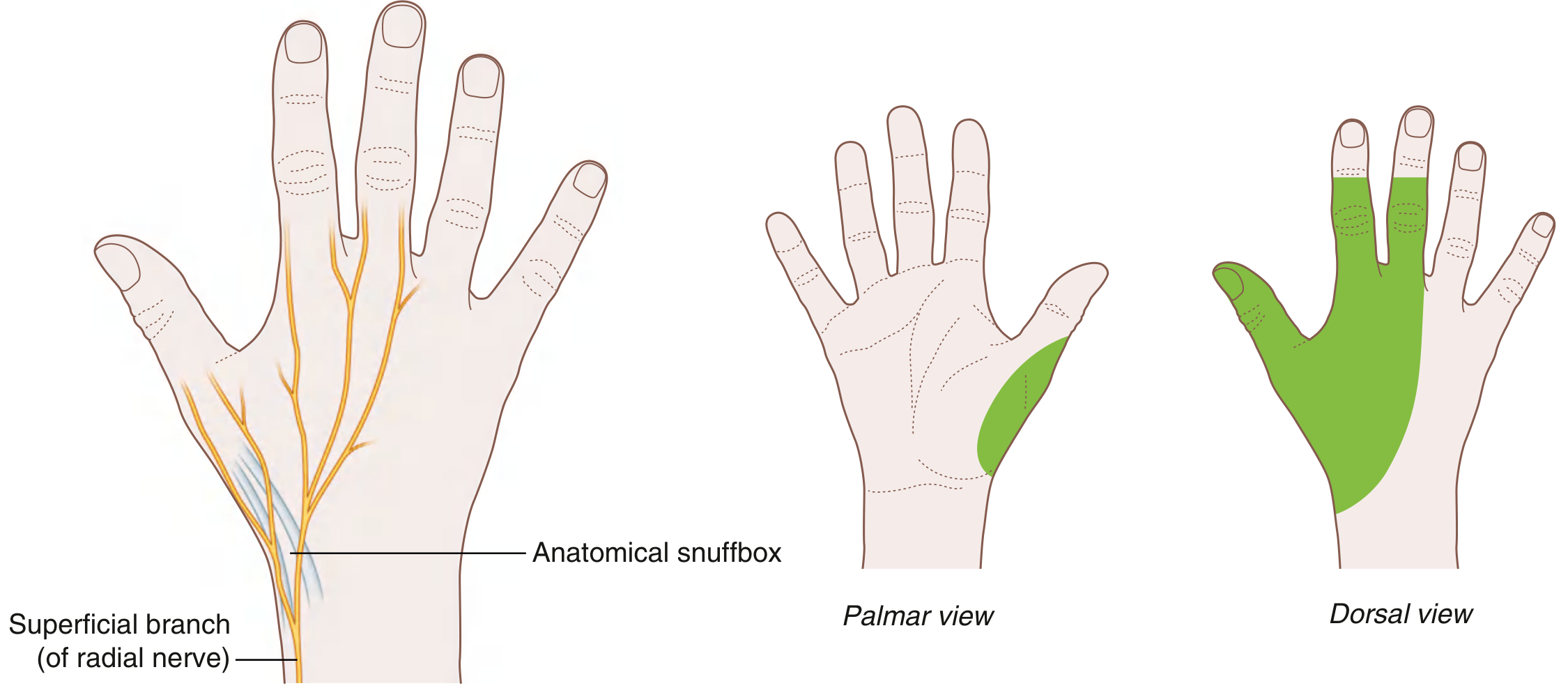
- Superficial radial nerve - pure sensory, supplies dorsoradial hand (thumb, index, middle, half ring finger)
Causes / Common Injury Sites
| Level | Typical Cause |
|---|---|
| Axilla | Crutch palsy, "honeymoon palsy," shoulder joint replacement |
| Spiral groove (most common) | "Saturday-night palsy" (drunken sleep), humeral shaft fractures (22% are associated with radial nerve injury) |
| Elbow / radial tunnel | Lateral epicondyle fractures, lipoma, ganglioma, rheumatoid synovitis |
| Wrist (superficial branch) | Tight wristbands, handcuffs, de Quervain's tenosynovitis - "cheiralgia paresthetica / Wartenberg's syndrome" |
- Bradley & Daroff's Neurology, p. 2464
- Sabiston Textbook of Surgery, p. 810
Clinical Presentation
1. Motor Loss - Level Dependent
High Lesion (Axilla level)
- Triceps weakness (elbow extension lost)
- Wrist drop (loss of wrist extension)
- Loss of finger and thumb extension at MCP joints
- Loss of supination (with elbow extended)
- Brachioradialis weakness (elbow flexion in mid-prone position impaired)
Mid-Arm Lesion (Spiral groove - most common)
- Triceps spared (branches leave before the spiral groove)
- Wrist drop - the hallmark sign - inability to extend wrist
- Loss of extension at MCP joints of all fingers
- Brachioradialis weakness
- Loss of thumb abduction and extension
PIN Lesion (forearm level)
- No wrist drop per se - wrist extension partially preserved because ECRL is spared
- Radial deviation of wrist on attempted extension (pathognomonic) - ECU is weak, ECRL intact
- Dropped fingers - inability to extend at MCPs
- No sensory deficit (PIN is purely motor)
Important clinical note:
The interossei (ulnar nerve) extend the interphalangeal joints via the extensor expansion - this is preserved in radial nerve palsy. Students must not misinterpret IP extension as a sign of nerve recovery (S Das, p. 143).
2. Sensory Loss
- Spiral groove / arm lesions: Reduced/absent sensation over the dorsum of hand, first web space, dorsal surfaces of thumb, index, middle, and radial half of ring finger
- Axilla lesion: Additional loss over extensor surface of forearm and lateral arm (posterior cutaneous nerve of arm and posterior cutaneous nerve of forearm also affected)
- PIN lesion: No sensory loss (pure motor)
- Superficial radial nerve (wrist): Paresthesia and pain over dorsoradial hand only; small area of hypoesthesia in dorsoradial hand
3. Reflexes
- Brachioradialis reflex: Diminished or absent
- Triceps reflex: Absent in axillary lesions; preserved in spiral groove lesions
4. Deformity
- Wrist drop: characteristic drooping of the wrist, inability to maintain wrist in extension against gravity
- Risk of flexion contractures of wrist and fingers if left unsupported
- No intrinsic hand muscle wasting (those are ulnar/median nerve)
Summary Table: Lesion Level vs. Findings
| Feature | Axilla | Spiral Groove | PIN (Forearm) |
|---|---|---|---|
| Triceps | Weak | Spared | Spared |
| Wrist extension | Lost | Lost | Partial (radial deviation) |
| Finger MCP extension | Lost | Lost | Lost |
| Brachioradialis | Weak | Weak | Spared |
| Sensory loss | Arm + forearm + hand dorsum | Hand dorsum | None |
| Wrist drop | Yes | Yes | No (radial deviation) |
- Bradley & Daroff's Neurology, p. 2466
- S Das Clinical Surgery, p. 142-143
Investigations
- Electrodiagnostic studies (EMG/NCS): Essential for confirming site, extent, severity, and prognosis. Low amplitude or absent radial SNAP is common (unless purely demyelinating at spiral groove). Conduction block = segmental demyelination (good prognosis). Denervation on needle EMG = axon loss.
- Ultrasonography: Useful adjunct - enlarged radial nerve CSA >5.75 mm² at the spiral groove is highly specific for radial neuropathy.
- X-ray / CT: To identify associated humeral fractures.
Prognosis
-
Neuropraxia (Saturday-night palsy, demyelinating conduction block): Usually recovers in 6-8 weeks
-
Axonotmesis (humeral fracture associated): Protracted course, often incomplete recovery
-
Closed injuries with humeral fracture: Spontaneous recovery in 60-92% of patients
-
High-velocity gunshot wounds or penetrating trauma: Surgical exploration recommended
-
Bradley & Daroff's Neurology, p. 2470-2474
-
Sabiston Textbook of Surgery, p. 810
Physiotherapy Management
Goals
- Prevent contractures and joint stiffness
- Maintain muscle extensibility
- Facilitate nerve regeneration
- Restore functional movement
- Sensory re-education
- Maximize ADL function during recovery
Phase 1: Acute / Early Phase (Week 0-6)
A. Splinting / Orthotic Support
The most immediately important physiotherapy intervention is appropriate splinting:
- Cock-up / wrist extension splint (static): Maintains wrist in dorsiflexion (~30-40°), preserving grip strength and preventing wrist flexion contracture. This passive dorsiflexion of the wrist is indicated to preserve grip strength in wrist drop due to radial nerve palsy. (Tintinalli's EM, p. 1819)
- Dynamic (functional) splint for high radial palsy: Dynamically splints the digits in extension, allowing active use of the hand for ADL tasks while the nerve recovers. This is particularly valuable when recovery is expected to take months.
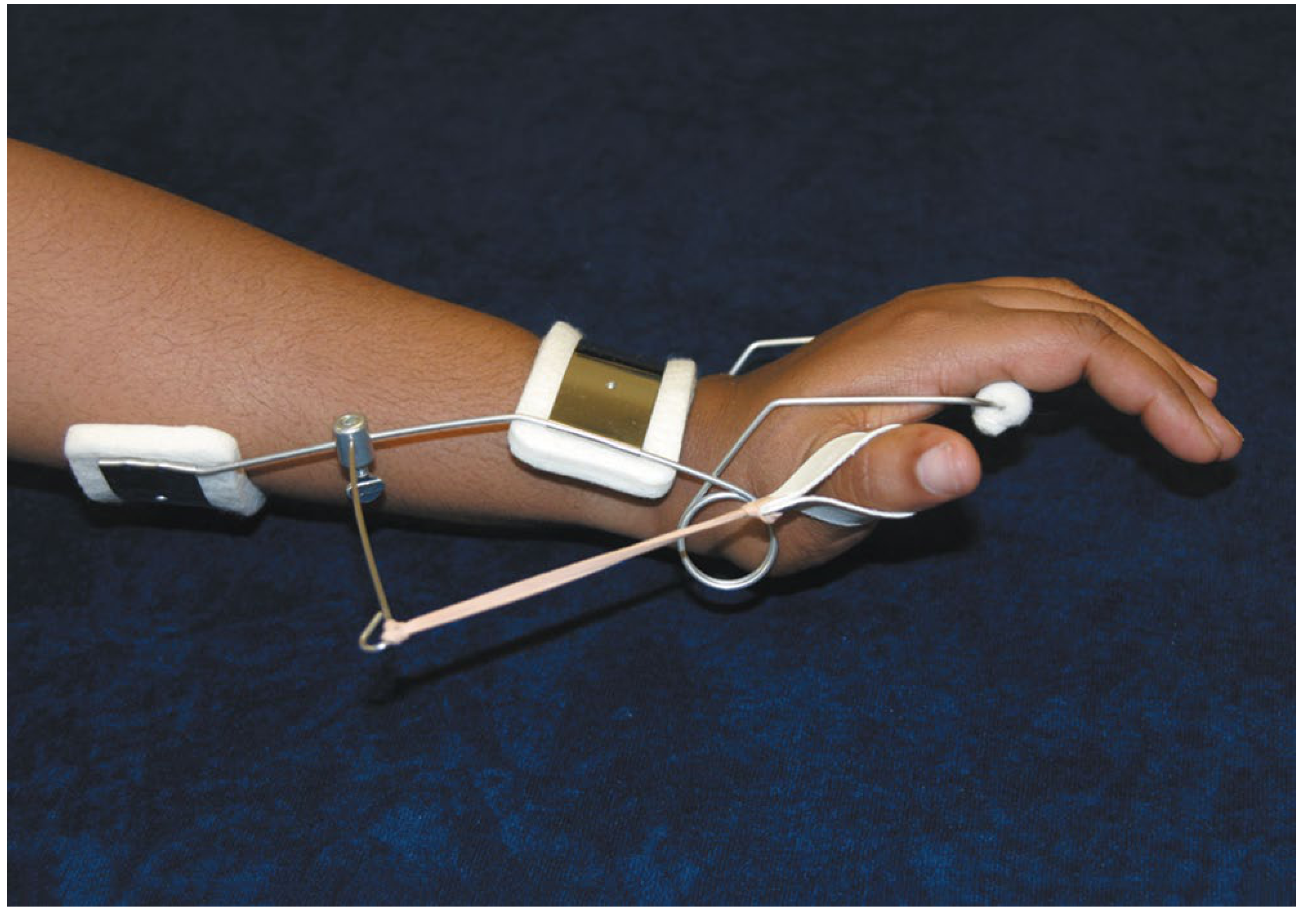
The splint should be removed periodically for exercise and skin hygiene. In a clinical case from Neuroanatomy Through Clinical Cases, a splint was prescribed immediately after posterior interosseous nerve injury to prevent contracture deformities while the nerve recovered over 4 months.
B. Passive Range of Motion (PROM) Exercises
- Daily passive extension of wrist, fingers, and thumb through full range
- Prevent shortening of finger and wrist flexors
- Maintain joint mobility of wrist, MCPs, and IPs
- Thumb abduction/extension PROM
C. Oedema Management
- Elevation of limb
- Gentle retrograde massage if soft tissue swelling present (e.g., post-fracture)
Phase 2: Intermediate Phase (With Signs of Recovery)
A. Active-Assisted and Active Exercises
- As nerve regeneration progresses (typically proximal to distal), begin active-assisted exercises:
- Wrist extension (assisted)
- Finger MCP extension
- Thumb extension and abduction
- Supination exercises
- Progress to active resisted exercises as muscle strength improves
- Brachioradialis strengthening (elbow flexion in mid-prone position)
B. Strengthening Exercises
- Graduated resistance training for wrist extensors, finger extensors (EDC), EPL, EPB, APL
- Grip strengthening (intrinsics and flexors are intact - capitalize on preserved function)
- Forearm supination strengthening
C. Sensory Re-Education
- For spiral groove / axillary lesions with sensory loss
- Tactile discrimination exercises (texture identification, object recognition)
- Protective sensation training to prevent inadvertent injury
- Vibration-stimulus training
D. Neuromuscular Electrical Stimulation (NMES / FES)
- Applied to denervated wrist and finger extensor muscles
- Aims to maintain muscle bulk, prevent atrophy, and improve re-innervation
- Typically used when complete denervation is confirmed on EMG
E. Nerve Gliding (Neural Mobilization) Exercises
- Radial nerve neurodynamic mobilization to improve nerve mobility and reduce intraneural fibrosis
- Performed in graduated range with respect to pain and irritability
Phase 3: Late / Functional Rehabilitation
A. Functional Task Training
- ADL retraining with improving hand function
- Writing, dressing, eating - incorporating wrist extension
- Occupational therapy collaboration is key (as demonstrated in the clinical case - patient was followed by occupational therapist as strength gradually recovered)
B. Progressive Strengthening
- Eccentric and concentric wrist extensor exercises with progressively heavier resistance
- Fine motor coordination training
C. Tendon Transfer Considerations (Surgical adjunct)
- When recovery is incomplete after 3-6 months (no return of function in expected timeline), tendon transfer surgery may be planned
- Physiotherapy is essential pre- and post-tendon transfer:
- Pre-op: maintain full PROM of all joints
- Post-op: motor re-education of transferred tendons, graded exercises
Special Considerations by Injury Type
| Injury Type | PT Priority |
|---|---|
| Saturday-night palsy (neuropraxia) | Static splint + PROM; expect recovery 6-8 weeks |
| Humeral fracture + radial palsy | Co-manage fracture immobilization + splint; monitor for spontaneous recovery |
| PIN syndrome | No wrist splint needed (wrist extension partially preserved); focus on finger extension exercises |
| Superficial radial nerve (Wartenberg's) | Activity modification, desensitization, padding of wrist |
| Post-nerve repair / graft | Protect repair 3 weeks, then graduated nerve gliding and PROM |
Summary of Physiotherapy Interventions
| Intervention | Purpose |
|---|---|
| Static wrist extension splint | Prevent flexion contracture, preserve grip |
| Dynamic radial palsy splint | Allow functional use during recovery |
| PROM exercises | Maintain joint mobility, prevent soft tissue shortening |
| AROM / ARAM / strengthening | Restore muscle strength as re-innervation occurs |
| NMES / electrical stimulation | Maintain muscle bulk, reduce atrophy |
| Nerve gliding exercises | Restore nerve mobility, reduce adhesions |
| Sensory re-education | Restore sensory discrimination |
| Functional/ADL training | Maximize independence and participation |
| Patient education | Skin care (sensory loss), joint protection, splint use |
Sources
- Bradley and Daroff's Neurology in Clinical Practice, pp. 2460-2483
- S Das A Manual on Clinical Surgery, 13th Ed., pp. 142-143
- Gray's Anatomy for Students, p. 940
- Sabiston Textbook of Surgery, p. 810
- Campbell's Operative Orthopaedics, 15th Ed., 2026
- Miller's Review of Orthopaedics, 9th Ed., p. 3202-3216
- Tintinalli's Emergency Medicine, p. 1819
- Neuroanatomy Through Clinical Cases, 3rd Ed., p. 398
Discuss in detail about Physiotherapy Management of a patient with complete Spinal Cord Injury at T4 level
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"spinal cord injury" AND rehabilitation AND paraplegia
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. I have enough to write a very detailed, well-structured answer. Let me now compose the full response.
Physiotherapy Management of Complete Spinal Cord Injury at T4 Level
Understanding the Lesion: What T4 Complete (ASIA A) Means
A complete SCI at T4 (ASIA Impairment Scale Grade A) means:
- No motor or sensory function is preserved in the sacral segments S4-S5
- The lesion is classified as paraplegia (both lower limbs affected; upper limbs fully intact)
- The neurological level is T4 - the nipple line is a key dermatome landmark for T4
- All spinal cord tracts are destroyed at this level
Functional expectations (Harrison's, Table 43-4):
Paraplegia (below T1): Self-care: Independent | Transfers: Independent | Maximum Mobility: Ambulates short distances with aids
This forms the rehabilitation target.
What is preserved vs. lost at T4 Complete SCI
| System | Status |
|---|---|
| Upper limb motor/sensation (C1-T3 intact) | Fully intact |
| Trunk muscles below T4 (abdominals, intercostals) | Paralyzed |
| Lower limb motor function | Absent |
| Lower limb sensation | Absent |
| Bladder/bowel control | Lost (upper motor neuron pattern - detrusor hyperreflexia) |
| Autonomic function | At risk for autonomic dysreflexia (T4 is above T6 splanchnic outflow) |
| Respiratory | Upper intercostals partially affected; diaphragm intact (C3-C5) |
Phase 1: Acute / Spinal Shock Phase (Days 1-14)
A. Respiratory Management
At T4, the intercostal muscles from T4 downward are paralyzed. Diaphragm (C3-C5) is intact, but vital capacity is significantly reduced.
PT Interventions:
- Chest physiotherapy: Assisted coughing techniques, postural drainage, percussion and vibration to prevent atelectasis and pneumonia
- Incentive spirometry: Encourage deep breathing exercises
- Assisted / augmented cough: The therapist applies manual pressure to the lower thorax/abdomen during expiration to augment cough force
- Positioning: Semi-recumbent positioning where tolerated; suction if needed
- Breathing exercises: Diaphragmatic breathing training
- Monitoring: Pulse oximetry, regular respiratory rate and SpO2 checks
B. Positioning and Pressure Care
- Complete SCI eliminates all protective sensation below T4 - pressure injuries develop rapidly on insensate skin
- 2-hourly repositioning in bed: supine, side-lying (30° tilt), prone when medically stable
- Special pressure-relieving mattresses (dynamic air alternating or foam)
- Careful heel protection: padded heel boots, foam wedges under calves
- Sacral and ischial protection: key pressure points in the SCI patient
- Education of nursing staff and family in log-roll technique for turning
Harrison's: "Prophylaxis against decubitus ulcers should involve frequent changes in position in a chair or bed, the use of special mattresses, and cushioning of areas where pressure sores often develop, such as the sacral prominence and heels."
C. DVT Prevention
- Patients with complete SCI are at high risk for DVT and pulmonary embolism
- PT role: Passive lower limb exercises (ankle pumps, hip/knee cycling movements)
- Calf compression devices (pneumatic sequential compression)
- Prophylactic anticoagulation is typically initiated medically (LMWH for 3 months)
- Harrison's: "Use of calf-compression devices and anticoagulation with low-molecular-weight heparin are recommended."
D. Passive Range of Motion (PROM) Exercises
- Daily full PROM to all paralyzed lower limb joints: hips, knees, ankles, toes
- Prevents contractures which would impair future transfer ability and seating
- Hip flexion, abduction, extension; knee flexion/extension; ankle dorsiflexion/plantarflexion
- Particular attention to maintaining hip extension (prevents hip flexion contracture) and ankle dorsiflexion (prevents equinus contracture)
- Correct positioning in neutral alignment during rest
Bailey & Love: "Soft-tissue contractures around joints may occur as a result of spasticity but can be avoided by appropriate physical therapy, positioning and splinting."
E. Upper Limb Strengthening
- Fully intact - begin early progressive strengthening
- Shoulder girdle, elbow, wrist strengthening (will be essential for transfers, wheelchair mobility)
- Resistance exercises for shoulder depressors, triceps, and latissimus dorsi - critical for push-up relief from wheelchair seat (pressure relief)
Phase 2: Early Rehabilitation (Weeks 2-8)
A. Bed Mobility Training
The first functional skills to train:
- Rolling: Log-roll with assistance, progressing to active rolling using arm momentum
- Supine to sitting: Using upper limbs to push up, using head-hips relationship
- Long-sitting balance: Maintaining upright posture in long-sit position (legs extended) - challenges posterior ligaments and hip flexors
- Short-sitting balance (legs over edge of bed): Maintaining trunk stability using upper limbs on the mat
Key challenge: With T4 SCI, all trunk muscles below T4 are lost. The patient relies on intact upper trapezius, serratus anterior, pectorals, and shoulder girdle muscles to stabilize. Balance in sitting is a major training focus.
B. Transfer Training
A critical independence goal. For T4 paraplegia, independent transfers are expected:
- Lateral sliding transfers: Between bed and wheelchair, wheelchair and toilet, wheelchair and car
- Requires strong shoulder depression (trapezius, serratus, triceps)
- Use of transfer board initially, progress to unassisted
- Supine to sitting transfer
- Floor to wheelchair transfer (advanced - important for falls safety)
Physiotherapist role: Teach technique, provide guarding, progress from assisted to independent over weeks.
C. Sitting Balance and Trunk Stability Training
- With complete T4 SCI, no abdominal or lower trunk muscles are active
- Sitting balance is maintained by locking the arms or using proximal upper limb muscles
- Progression:
- Static sitting with bilateral arm support
- Unilateral arm support
- Hands-free sitting with practice of protective reactions
- Reaching tasks in all directions
Trunk stability exercises: Use of arms-reaching tasks, reaching to floor, overhead - all challenging balance reactions. Proprioceptive neuromuscular facilitation (PNF) techniques applied to the upper trunk.
D. Wheelchair Prescription and Training
A well-fitted manual wheelchair is the primary mobility aid for T4 paraplegia:
- Wheelchair prescription: Lightweight rigid or folding frame; seat dimensions precisely fitted; appropriate seat cushion (pressure-relieving foam/gel/air for sacral protection)
- Propulsion training: Manual wheelchair propulsion technique on flat surfaces, inclines, rough terrain, ramps, and curbs
- Pressure relief: Teaching push-up relief every 15-30 minutes (lifts body weight off ischium by pressing down on armrests/wheels) - vital for pressure sore prevention
- Wheelchair sports and community mobility: Integration into real-world environments
E. Standing Program
Even for complete T4 SCI, standing has important physiological benefits:
- Prevents disuse osteoporosis (weight-bearing stimulus through long bones)
- Reduces spasticity
- Prevents hip flexion contractures
- Psychological benefit
Standing equipment used:
- Tilt table: Gradual progressive tilting from horizontal to vertical (begin 30°, increase over days/weeks to 80°) - also monitors for orthostatic hypotension
- Standing frame / standing wheelchair: For sustained daily standing (target 30-60 minutes/day)
- Knee-ankle-foot orthoses (KAFOs) with parallel bars or walking frame for therapeutic standing/stepping
Phase 3: Advanced Rehabilitation (Weeks 8 onwards)
A. Gait / Ambulation Training
For complete T4 paraplegia, functional community ambulation is generally not achieved due to energy expenditure limitations. However, therapeutic ambulation has value:
Options:
- KAFOs (Knee-Ankle-Foot Orthoses) with parallel bars or forearm crutches: Swing-through or swing-to gait pattern
- Reciprocating Gait Orthosis (RGO): Cables link hip joints to allow reciprocal stepping; requires high upper limb strength
- Body Weight Supported Treadmill Training (BWSTT): Harness supports partial body weight while patient walks on treadmill - facilitates stepping even in complete injuries by activating spinal pattern generators
- Robotic-assisted gait training (Lokomat, Ekso, ReWalk): Exoskeleton devices providing supported stepping practice - the 2020 clinical practice guidelines (cited in Current Surgical Therapy) recommend virtual reality walking and circuit training for CNS injury rehabilitation
B. Spasticity Management
Above T6, T4 SCI produces an upper motor neuron syndrome - spasticity develops over weeks to months:
PT Interventions for spasticity:
- Prolonged passive stretching: Daily slow, sustained stretching of spastic muscles (hamstrings, hip flexors, calf)
- Splinting and positioning: Anti-spasticity positioning (prevents reinforcement of spastic patterns)
- Standing: Weight-bearing reduces spasticity
- Hydrotherapy / warm water immersion: Reduces spastic tone
- Ice/cold application: Temporarily reduces spasticity for exercise
- TENS / electrical stimulation: Can inhibit spasticity circuits
Pharmacological adjuncts (prescribed by physician, PT monitors effect):
- Baclofen up to 240 mg/day - most effective
- Tizanidine 2-8 mg TID
- Diazepam 2-4 mg at bedtime (for nocturnal spasms)
- Intrathecal baclofen pump (refractory cases)
- Botulinum toxin injections to focal spastic muscles
- Harrison's: "Spasticity is aided by stretching exercises to maintain mobility of joints... Baclofen (up to 240 mg/d in divided doses) is effective."
Autonomic Considerations for PT
Autonomic Dysreflexia (AD) - A Medical Emergency
T4 is above T6, placing this patient at risk for autonomic dysreflexia:
- Definition: Massive uncontrolled sympathetic discharge triggered by a noxious stimulus below the injury level
- Clinical features: Sudden severe hypertension, pounding headache, flushing and diaphoresis above the injury level, pallor/cool skin below, bradycardia
- Common triggers: Bladder distension (most common), fecal impaction, pressure sore, pain, tight clothing, catheter blockage
PT responsibilities:
- Recognize early signs of AD during therapy sessions
- Stop exercise immediately
- Sit patient upright (reduces blood pressure orthostically)
- Check and relieve the cause (check catheter, check clothing, loosen tight equipment)
- Call medical staff if symptoms persist
- Never ignore patient complaints of headache during PT session
Bradley & Daroff's: "Autonomic dysreflexia represents an acute syndrome characterized by excessive and uncontrolled sympathetic output from the spinal cord... Common triggers include bladder distention, constipation, rectal fissures, joint injury, and urinary tract infection."
Goldman-Cecil: "These episodes can be triggered by bladder distension, fecal impaction, or nociceptive stimuli below the lesion and may result in hypertensive encephalopathy, cerebral or retinal hemorrhage, and cardiac arrhythmias."
Orthostatic Hypotension
- Common in early rehabilitation (loss of sympathetic vasoconstriction below T4)
- PT management: Gradual tilting on tilt table; abdominal binder, lower limb compression stockings to reduce venous pooling; slow progression from lying to sitting to standing; monitoring blood pressure with all position changes
Thermoregulation
- Loss of thermoregulatory sweating below T4; risk of hyperthermia in hot environments and hypothermia in cold
- PT ensures appropriate environmental conditions and monitors patient temperature during exercise
Bladder and Bowel Program
Bladder (T4 = Upper Motor Neuron lesion)
- Detrusor hyperreflexia + sphincter dyssynergia
- PT role: Educate on clean intermittent catheterization (CIC) schedule (every 4-6 hours)
- Monitor fluid intake patterns
- Oxybutynin / anticholinergic drugs prescribed to treat detrusor overactivity
Harrison's: "Detrusor spasticity is treated with anticholinergic drugs (oxybutynin, 2.5-5 mg qid)..."
Bowel
- Upper motor neuron bowel (reflexic): bowel emptying can be triggered by digital rectal stimulation
- PT/OT educate on scheduled bowel program, diet, fluid management, positioning during bowel care
Prevention of Secondary Complications
1. Pressure Injuries
- Regular skin inspection by patient using mirror (especially sacrum, ischial tuberosities, heels, trochanters)
- Pressure relief technique: 15-30 second push-up every 15-30 minutes in wheelchair
- Appropriate wheelchair cushion prescribed
- Education on seating posture and duration limits
2. Heterotopic Ossification (HO)
- Ectopic bone formation in soft tissues around hips, knees (occurs in 25% of SCI patients - Bailey & Love)
- PT role: Maintain ROM (gentle), avoid vigorous manipulation of inflamed joints
- Bisphosphonates and indomethacin may be prescribed medically
3. Osteoporosis
- Disuse osteoporosis begins immediately below the injury level
- PT role: Weight-bearing programs (tilt table, standing), FES cycling, vibration therapy to partially mitigate bone loss
4. Pain Management
- Nociceptive pain: From musculoskeletal injuries, overuse of shoulders
- Neuropathic pain: At-level burning/dysesthetic pain - treated with gabapentin or pregabalin
- PT: Heat/cold, TENS, massage, activity modification; avoid shoulder overuse
Functional Electrical Stimulation (FES)
An important advanced PT modality for SCI:
- FES cycling: Electrical stimulation of lower limb muscles to produce cycling movement - maintains muscle bulk, reduces spasticity, improves cardiovascular fitness, reduces bone loss
- FES-assisted standing: Stimulates quadriceps and gluteals for therapeutic standing
- Combined with upper limb cycling for cardiovascular training (arm-FES ergometry)
- Recent systematic review (Hodgkiss et al., PLoS Med, 2023 - PMID 38011304) confirms exercise and FES improve aerobic capacity in SCI individuals
Psychological and Psychosocial Rehabilitation
- SCI is a catastrophic life event; depression, anxiety, and adjustment disorder are common
- PT works as part of the MDT (psychiatry, psychology, social work, OT, PT, SLT, nursing)
- Peer support programs (connecting with other SCI survivors)
- Goal-setting that is patient-centered and functionally meaningful
- Return to work, sport, community participation planning
- 2017 AOSpine/AANS guidelines (cited in Current Surgical Therapy) place strong emphasis on psychosocial rehabilitation
Expected Functional Outcomes for T4 Complete SCI
| Function | Expected Outcome |
|---|---|
| Bed mobility | Independent |
| Pressure relief | Independent (push-up technique) |
| Transfers | Independent (sliding board → unassisted) |
| Dressing (upper body) | Independent |
| Dressing (lower body) | Independent with equipment |
| Wheelchair propulsion | Independent (manual wheelchair) |
| Bladder management | Independent CIC |
| Bowel management | Independent with digital stimulation |
| Community mobility | Manual wheelchair, accessible vehicle |
| Ambulation | Therapeutic only (KAFOs / standing frame) |
| Sport / recreation | Wheelchair sport |
Summary of Physiotherapy Management Phases
| Phase | Timing | Key PT Focus |
|---|---|---|
| Acute / spinal shock | Days 1-14 | Respiratory care, PROM, positioning, pressure care, DVT prevention |
| Early rehabilitation | Weeks 2-8 | Bed mobility, transfers, sitting balance, wheelchair basics |
| Active rehabilitation | Weeks 8-16 | Advanced transfers, wheelchair skills, standing program, spasticity management |
| Community integration | Months 4+ | Community wheelchair skills, vocational rehab, sport, independence |
Outcome Measures Used in SCI Rehabilitation
- ASIA Impairment Scale (AIS): A-E classification of completeness
- Spinal Cord Independence Measure (SCIM III): Self-care, respiratory/sphincter management, mobility (0-100)
- Functional Independence Measure (FIM): 18 items, motor and cognitive
- Berg Balance Scale / Wheelchair Skills Test
- 10-metre walk test (if any ambulation achieved)
Sources
- Harrison's Principles of Internal Medicine, 22nd Ed., Table 43-4 and rehabilitation section
- Bradley & Daroff's Neurology in Clinical Practice, pp. 735, 791-801 (Thoracic levels; Autonomic dysreflexia; Bladder dysfunction)
- Goldman-Cecil Medicine, Autonomic dysfunction section, p. 1472-1473
- Bailey & Love's Short Practice of Surgery, 28th Ed., pp. 413, 3212-3213
- Current Surgical Therapy, 14th Ed., pp. 3058-3065 (Rehabilitation After Acute SCI)
- Hodgkiss DD et al. Exercise and aerobic capacity in SCI: systematic review with meta-analysis. PLoS Med 2023 [PMID: 38011304]
Discuss in detail about Physiotherapy Management of a patient of traumatic Brain Injury with Level 4 on RLA Scale of Cognitive functioning ?
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"traumatic brain injury" AND rehabilitation AND agitation
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive textbook content. I have all the information I need to write a thorough, well-structured answer. Let me now compile the complete detailed response.
Physiotherapy Management of Traumatic Brain Injury: RLA Scale Level 4
Understanding the Rancho Los Amigos (RLA) Scale
The Rancho Los Amigos (RLA) Levels of Cognitive Functioning Scale was developed at Rancho Los Amigos Hospital and is the standard clinical tool for tracking cognitive recovery after TBI. It has 10 levels (revised), with Level I being no response and Level X being purposeful, appropriate behavior.
All 10 RLA Levels - Overview
| Level | Description |
|---|---|
| I | No Response |
| II | Generalized Response |
| III | Localized Response |
| IV | Confused - Agitated |
| V | Confused - Inappropriate, Non-Agitated |
| VI | Confused - Appropriate |
| VII | Automatic - Appropriate |
| VIII | Purposeful - Appropriate |
| IX | Purposeful, Appropriate (Stand-By Assist) |
| X | Purposeful, Appropriate (Modified Independence) |
RLA Level IV: Confused - Agitated
Defining Characteristics
A patient at RLA Level IV is the most challenging to manage in acute neurorehabilitation. The defining features are:
1. Heightened state of activity:
- Patient is in a state of heightened agitation - may shout, scream, pull at lines/tubes
- Extreme restlessness and motor hyperactivity
- Purposeless, repetitive movements
2. Severely confused:
- Grossly disorientated to person, place, and time
- Unable to process new information
- Short attention span (seconds to minutes)
- No meaningful short-term memory - cannot carry over learning from session to session
3. Dangerous and impulsive behavior:
- May attempt to get out of bed without recognition of danger
- Attempts to remove IVs, NG tubes, urinary catheters, tracheostomy tubes
- May strike out at staff, bite, kick
- Verbally and/or physically aggressive
4. No awareness of deficits:
- Complete lack of insight into injury or limitations
- Appears to be "fighting" all attempts at care
- Cannot cooperate with voluntary rehabilitation activities
5. Internally driven responses:
- Behavior driven by internal discomfort, pain, or fear rather than external stimuli
- May call out names, respond to hallucinated stimuli
Clinical context (Goldman-Cecil Medicine):
"Patients with moderate to severe traumatic brain injury have readily recognizable reductions in the level of consciousness, ranging from confusion to agitation to somnolence persisting for at least 24 hours."
This corresponds to moderate-to-severe TBI on the GCS (typically GCS <12), with patients emerging from coma/stupor into this agitated confused phase before further recovery.
TBI Severity Classification (for Context)
| Severity | GCS | LOC | PTA |
|---|---|---|---|
| Mild | 13-15 | <30 min | <24 hours |
| Moderate | 9-12 | >30 min, <24 h | >24 hours, <7 days |
| Severe | <9 | >24 hours | >7 days |
A patient reaching RLA Level IV typically had a severe TBI (GCS ≤8) initially and is now emerging from the prolonged altered consciousness phase.
Neurocognitive sequelae of moderate-severe TBI (Bradley & Daroff, Table 44-8) include:
- Attention: difficulty with sustained attention, poor concentration
- Memory: problems acquiring and retaining new information
- Speed of information processing: slowed sensorimotor skills
- Executive functioning: poor judgment, difficulty planning
- Awareness of symptoms: difficulty recognizing deficits
- Language and communication: word comprehension problems
- Behavioral/emotional: frontal lobe syndrome - lowered frustration tolerance, impulsivity
Core Principles of Physiotherapy at RLA Level IV
Before listing specific interventions, there are cardinal principles that govern ALL PT interactions at this level:
1. Environment Modification (HIGHEST PRIORITY)
The PT environment must be carefully controlled:
- Low-stimulation environment: Single patient room preferred; dim lighting, reduced noise, limited visitors
- Reduce sensory overload: TV/radio off during therapy; one stimulus at a time
- Consistent caregivers: Same therapist each session reduces fear and agitation
- Predictable routine: Same time, same sequence daily
- Remove provocative stimuli: Tight clothing, full bladder, pain sources all trigger agitation
2. Session Duration and Timing
- Sessions must be very short - 5-15 minutes maximum, multiple times per day
- Stop immediately when agitation escalates (do not push through heightened agitation)
- Schedule therapy around the patient's natural calmer periods (often early morning or post-medication)
- Rest between sessions is as important as the activity itself
3. Communication Approach
- Use simple, short sentences (3-5 words maximum): "Bend your knee." "Move your arm."
- Use one command at a time - do not chain instructions
- Calm, soft, slow voice - tone matters more than content
- Provide orientation cues gently and repeatedly: "You are in hospital, you had an accident, you are safe"
- Never argue with a confused, agitated patient - redirect rather than confront
4. Safety First
- Bed rails up at all times when patient is unattended
- Padded mittens may be needed if patient pulls at tubes
- Low-low beds / floor-level mattresses to prevent fall injury
- One or two staff to guard during all sessions
- Document agitation patterns using validated tool (e.g., Agitated Behavior Scale - ABS)
Physiotherapy Assessment at RLA Level IV
Despite the agitation, a PT assessment can be carried out over multiple brief sessions:
A. Consciousness and Responsiveness
- Monitor RLA level progression over time
- Glasgow Coma Scale (even though emerging from coma)
- Coma Recovery Scale - Revised (CRS-R) if near-vegetative
B. Motor Assessment
- Observe resting posture: Decorticate (flexor) or decerebrate (extensor) posturing?
- Tone assessment: Spasticity, rigidity, hypotonia
- Passive ROM: Assess all joints during PROM (often only possible way to assess)
- Presence of contractures forming (common if positioning was neglected during coma)
- Reflexes: Abnormal reflexes (Babinski, hyperreflexia) suggest UMN involvement
C. Respiratory Assessment
- Respiratory pattern, SpO2, tracheostomy status
- Chest expansion symmetry
- Secretion load
D. Skin Integrity
- Pressure areas over sacrum, heels, occiput, elbows
- Splint/casting complications
E. Pain
- Non-verbal pain indicators (facial grimacing, increased agitation with movement)
- Use behavioral pain scales (CPOT, FLACC) if verbal assessment impossible
Specific Physiotherapy Interventions at RLA Level IV
1. Positioning and Postural Management
Why critical: The patient cannot voluntarily correct their position; abnormal tone drives harmful postures. Prolonged malpositioned lying causes pressure injuries, aspiration, contractures, and reinforces abnormal movement patterns.
Key positions and principles:
- Supine: Head of bed elevated 30° (reduces ICP, reduces aspiration risk); arms positioned in shoulder protraction, elbow extension, forearm neutral; legs in slight hip abduction and neutral rotation; ankles in 90° neutral (anti-equinus)
- Side-lying: Opposite side lying every 2 hours; top limb supported on pillow in functional position; avoid lying on hemiplegic arm
- Semi-reclined/sitting: Progress to 45-60° in bed; use positional supports
- Avoid: Prolonged hip flexion, knee hyperextension, ankle plantarflexion
Specific postural concerns in TBI:
- Decorticate posturing (common in TBI): Arms in flexion, internal rotation; legs in extension - requires counter-positioning into shoulder extension/external rotation, elbow extension
- Decerebrate posturing: All four limbs in extension/internal rotation - requires hip abduction, shoulder protraction supports
2. Passive Range of Motion (PROM) Exercises
The most important PT physical intervention at this level:
- Perform daily PROM to all joints of both upper and lower limbs
- Slow, gentle, rhythmic movements - avoid rapid forceful stretching (can increase agitation and trigger spasticity/clonus)
- Order of priority: Ankle dorsiflexion (prevent equinus), shoulder abduction/external rotation, hip extension, elbow extension, wrist/finger extension
- Duration: 10-15 repetitions per movement, multiple times daily
- Work within range of comfort - watch patient's facial expression and agitation cues
Bailey & Love: "Soft-tissue contractures around joints may occur as a result of spasticity but can be avoided by appropriate physical therapy, positioning and splinting."
3. Splinting and Serial Casting
Indications: When PROM + positioning alone cannot prevent or reverse contracture.
Common splints used:
- Ankle-foot orthosis (AFO) / resting foot splint: Maintains ankle at 90° to prevent equinus contracture (most common TBI contracture)
- Elbow extension splint: For arms held in persistent flexion posture
- Wrist extension splint: Prevents wrist and finger flexion contracture
- Hand resting splint: Thumb abducted, fingers gently extended
Principles of splinting at Level IV:
- Wear schedule: 2 hours on, 2 hours off (skin checks each removal)
- Patient may pull at splints in agitation - ensure secure but non-restrictive application
- Monitor skin integrity carefully under all splints
- Serial casting used for fixed contractures - cast changed every 5-7 days as range improves
4. Respiratory Physiotherapy
Many TBI patients at Level IV have concurrent respiratory complications (aspiration pneumonia, atelectasis, mechanical ventilation):
Interventions:
- Positioning for postural drainage: Dependent lung segments up; use modified positions where ICP is a concern
- Assisted coughing / manual techniques: Percussion, vibration over affected lung segments
- Suction (in coordination with nursing/respiratory therapy) for tracheostomy or oral secretions
- Breathing exercises: May be impossible voluntarily at Level IV - rely on positioning and passive techniques
- Weaning from ventilation: PT works with respiratory therapists on upright positioning and diaphragmatic work to facilitate extubation
5. Mobilization and Early Upright Activity
Evidence for early mobilization after TBI is strong - but must be modified for agitation at Level IV:
Progression:
- Tilt table: Begin once medically stable; gradual tilting from horizontal to 60-80° vertical
- Monitor blood pressure and heart rate (autonomic instability common post-TBI)
- Watch for signs of increased agitation with positional change
- Begin at 15 minutes, progress as tolerated
- Benefits: Prevents orthostatic hypotension, improves alertness/arousal, reduces lower limb spasticity, maintains bone density
- Sitting over edge of bed (with maximal assist): Even brief sitting has significant arousal and orientation benefits
- Supported sitting in chair/tilt-back wheelchair: Progress once sitting is tolerated
- Standing with full support: Standing frame or tilt table standing with full weight-bearing
Important: Upright positioning itself often improves orientation and reduces agitation in Level IV patients by providing vestibular and proprioceptive input.
6. Sensory Stimulation Program
At Level IV, the patient is emerging from low consciousness and sensory input can facilitate arousal and orientation:
Structured sensory stimulation:
- Tactile: Firm pressure touch (deep touch preferred over light touch which can increase agitation); textured materials, familiar objects placed in hand
- Auditory: Familiar voices (family members), familiar music (can significantly reduce agitation); avoid sudden loud noises
- Olfactory: Familiar pleasant scents (family member's perfume/cologne); can trigger recognition
- Visual: Familiar photos placed in line of sight; high contrast images; natural light exposure
- Proprioceptive/vestibular: Weight-bearing through limbs during standing; joint approximation; rhythmic movement
Important: Stimulation at Level IV should be structured and limited - overstimulation worsens agitation. One modality at a time.
7. Tone Management / Spasticity Reduction
The mechanism (Miller's Review of Orthopaedics):
"Disruption of the upper motor neuron pathways can lead to paralysis, muscular imbalance, and acquired spasticity, which ultimately" results in contracture if unmanaged.
PT interventions:
- Prolonged slow passive stretching: Most effective non-pharmacological intervention
- Weight-bearing: Standing reduces lower limb extensor spasticity
- Cold/ice application: Temporarily reduces spasticity to enable easier ROM
- Positioning: Anti-spasticity postures (see above)
- Rhythmic movement: Slow rhythmic rocking can reduce tone (works via spinocerebellar pathways)
- Hydrotherapy: Warm water significantly reduces tone (when feasible)
Pharmacological (team decision, monitored by PT):
- Baclofen, tizanidine (oral)
- Intrathecal baclofen (for severe refractory spasticity)
- Botulinum toxin A injections (focal muscles, typically used after Level IV)
8. Pain Management
The agitation at Level IV is frequently driven or worsened by unrecognized pain:
- Fractures, soft tissue injuries co-existing with TBI
- Headache (common post-TBI)
- Catheter/tube discomfort
PT role:
- Identify and remove noxious stimuli before and during therapy
- Gentle handling to minimize procedural pain
- Positioning to offload painful areas
- TENS, heat/cold as adjuncts
- Communicate pain observations to the medical team (cannot rely on self-report)
Managing Agitation During PT Sessions
This is the most challenging clinical skill at Level IV:
Agitation De-escalation Strategies in PT
| Strategy | How to Apply |
|---|---|
| Reduce stimulation | Stop what you are doing, move to quieter area, reduce noise/light |
| Calm voice | Lower your tone, speak slowly, use patient's name |
| Redirection | Gently redirect activity: "Let's try moving your arm instead" |
| Familiar comfort objects | Blanket from home, familiar smell, family photo |
| Rhythmic movement | Gentle rocking, swaying (activates inhibitory circuits) |
| Music | Pre-selected familiar calming music; can dramatically reduce agitation |
| Remove triggers | Check: Is the catheter blocked? Is clothing too tight? Is there pain? |
| Give space | If safe, allow patient to move within safe boundaries rather than restraining |
What to AVOID at Level IV:
- Arguing, debating, correcting
- Forced restraint (escalates agitation dramatically)
- Complex multi-step commands
- Long sessions or repeated failed attempts
- Stimulating activities late in the day (sundowning effect)
Recent Systematic Review (Block H et al., Disabil Rehabil 2024 - PMID: 36694351): Clinical practice guideline recommendations for managing challenging behaviors after TBI in acute and inpatient rehab settings emphasize environmental modification and behavioral approaches as first-line management.
Pharmacological Management of Agitation (Team Decision - PT Input)
The PT should understand medications used at Level IV as they affect therapy participation:
Kaplan & Sadock's Comprehensive Textbook of Psychiatry identifies options:
- Amantadine: Dopaminergic agent - evidence for improving cognitive function post-TBI; often improves responsiveness and may reduce agitation
- Beta-blockers (propranolol): Reduce autonomic arousal components of agitation; useful for persistent agitation
- Valproate: For agitation/aggression with mood instability
- SSRIs (citalopram, escitalopram): For irritability, anxiety, emotional lability
- Avoid benzodiazepines: Increase confusion and paradoxically worsen agitation in TBI; sedation impairs rehabilitation
- Avoid haloperidol: May impair dopaminergic recovery mechanisms
Updated systematic review (Klimenko et al., J Neurotrauma, 2026 - PMID: 41051905) confirms pharmacological options for agitated behaviors in TBI patients in inpatient settings.
Family and Caregiver Education at Level IV
A critically underrecognized component of PT at this level:
Educate family on:
- What RLA Level IV means - this is a normal phase of recovery, not the endpoint
- How to interact: calm voice, simple reassurance, presence without demand
- What behaviors to expect and not to take personally (verbal/physical aggression is the injury, not the person)
- How to participate in therapy: provide familiar voice, familiar music
- How to perform simple passive movements and positioning under PT guidance
- Safety: do not attempt to restrain, do not argue
- Prognosis: most patients continue to progress through RLA levels with intensive rehabilitation
Goal Setting at RLA Level IV
Short-term physiotherapy goals:
- Prevent secondary complications: pressure injuries, contractures, DVT, pneumonia
- Maintain full PROM in all joints
- Reduce agitation through environmental and sensory strategies
- Tolerate 5-10 minutes of upright positioning/tilt table
- Establish basic safety protocols and family education
Anticipate progression to RLA Level V (Confused - Inappropriate, Non-Agitated):
- As agitation diminishes, more purposeful therapeutic activities become possible
- Memory and orientation continue to be impaired but patient becomes more manageable
- More structured ADL training can begin
MDT Roles at RLA Level IV
| Professional | Role |
|---|---|
| Physiotherapist | PROM, positioning, splinting, respiratory care, tilt table, tone management, mobility |
| Occupational Therapist | Splinting, ADL positioning, sensory programs, upper limb function |
| Speech-Language Therapist | Dysphagia assessment, communication strategies, cognitive communication |
| Neuropsychologist | Cognitive assessment, behavior management planning |
| Psychiatry | Medication for agitation, mood disorders |
| Nursing | 24-hour positioning, skin care, bowel/bladder, catheter management |
| Social Work | Family support, care planning |
| Physician/Intensivist | Medical optimization, ICP management, seizure prophylaxis |
Outcome Measures for TBI Rehabilitation
- Rancho Los Amigos Scale (RLA): Primary functional tracking tool
- Glasgow Coma Scale (GCS): Consciousness level
- Agitated Behavior Scale (ABS): Quantifies agitation severity (14 items, score 14-42; ≥22 = clinically significant agitation)
- Disability Rating Scale (DRS): Tracks global disability 0-29
- Functional Independence Measure (FIM): Motor and cognitive subscales
- Coma Recovery Scale - Revised (CRS-R): For near-vegetative patients
- Post-Traumatic Amnesia duration: Predictor of long-term outcome
Prognosis and Recovery Trajectory
Recovery from RLA Level IV follows a predictable trajectory in most patients:
- Duration at Level IV varies: days to weeks depending on severity
- Younger patients, less severe injury, earlier rehabilitation = faster progression
- Predictors of poor outcome (Bradley & Daroff; Goldman-Cecil): older age, GCS <6, bilateral unreactive pupils, diffuse axonal injury on MRI
- Most patients who reach Level IV will progress to Level V-VI with appropriate rehabilitation
- The 2020 clinical practice guidelines (cited in Current Surgical Therapy) recommend early rehabilitation once medically stable and place strong emphasis on psychosocial rehabilitation
Summary: Physiotherapy Priorities at RLA Level IV
| Priority | Intervention |
|---|---|
| FIRST | Environmental modification - reduce stimulation |
| FIRST | Safety - bed rails, padded bed, supervision |
| DAILY | PROM to all limbs |
| DAILY | Positioning and repositioning every 2 hours |
| DAILY | Splint application and monitoring |
| DAILY | Respiratory care if needed |
| PROGRESSIVE | Upright positioning / tilt table |
| ALWAYS | Family education and involvement |
| ALWAYS | Short sessions, multiple times per day |
| ALWAYS | Document RLA level and agitation scores |
Sources
- Bradley & Daroff's Neurology in Clinical Practice, pp. 3198-3219 (TBI neurocognitive sequelae, Table 44-8)
- Goldman-Cecil Medicine, 22nd Ed., pp. 1404-1415 (TBI Clinical Manifestations and Treatment)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, pp. 1669-1706 (TBI severity grading, behavioral management)
- Bailey & Love's Short Practice of Surgery, 28th Ed., p. 3213 (contracture prevention)
- Miller's Review of Orthopaedics, 9th Ed., pp. 2420-2435 (acquired spasticity)
- Current Surgical Therapy, 14th Ed., pp. 3058-3060 (rehabilitation after acute TBI)
- Block H et al. Clinical practice guideline recommendations for challenging behaviors after TBI. Disabil Rehabil 2024 [PMID: 36694351]
- Klimenko T et al. Pharmacological interventions for agitated behaviors in TBI. J Neurotrauma 2026 [PMID: 41051905]
This is a shared conversation. Sign in to Orris to start your own chat.