Churg strauss syndrome full details for md exams 15marks answer from fishman and murray only
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive 15-mark MD exam answer. Here is the full structured answer from Fishman's and Murray & Nadel's:
Eosinophilic Granulomatosis with Polyangiitis (Churg-Strauss Syndrome) - 15 Marks
1. Introduction and Nomenclature
Churg-Strauss Syndrome (CSS) was originally described in 1951 by Jacob Churg and Lotte Strauss as "allergic granulomatosis, allergic angiitis and periarteritis nodosa," based largely on autopsy findings. The authors recognized the allergic background, blood and tissue eosinophilia with granulomatous inflammation leading to necrosis, and vasculitis - the final outcome of the disease before any mitigating therapy was available.
At the 2012 Chapel Hill Consensus Conference on Nomenclature of the Vasculitides, it was renamed Eosinophilic Granulomatosis with Polyangiitis (EGPA) - a name intended to reflect the most prevalent pathology, the pathogenic role of eosinophils, and its similarities to the vasculitis shared with Granulomatosis with Polyangiitis (GPA) and Microscopic Polyangiitis (MPA).
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (block 15)
- Murray & Nadel's Textbook of Respiratory Medicine (Ch. 96)
2. Definition
EGPA is a rare, systemic small-vessel vasculitis associated with:
- A prominent allergic component
- Asthma
- Blood and tissue eosinophilia
- Eosinophil-rich and granulomatous inflammation involving the respiratory tract
- Necrotizing small- to medium-vessel vasculitis
It involves capillaries, venules, and arterioles. Granulomas, eosinophils, and palisading histiocytes in extravascular tissues are hallmarks that distinguish EGPA from other vasculitides.
Incidence: Annual incidence estimated at 0.6 to 6.8 cases per million.
Fishman's Pulmonary Diseases and Disorders (block 13)
3. Classification
EGPA is classified among the ANCA-Associated Vasculitides (AAV) because of similarities of the small-vessel vasculitis, even though only 30-70% of patients with active EGPA are ANCA positive. In most cases circulating ANCAs are absent, and robust criteria of documented systemic vasculitis are not always present.
Murray & Nadel's (Ch. 96)
4. Epidemiology
- Predominates in the fourth or fifth decade of life
- No gender predominance (contrasts with allergic asthma, which predominates in women and presents earlier)
- Presents earlier in life than other ANCA-associated vasculitides
- Occasionally reported in children and adolescents
Murray & Nadel's (Ch. 96)
5. Pathology
Because diagnosis is now made earlier, lung biopsy is seldom necessary and patients may receive corticosteroids before overt vasculitis has developed.
Classic pathologic features (on biopsy):
| Feature | Description |
|---|---|
| Vasculitis | Necrotizing or non-necrotizing, involving mainly medium-sized pulmonary arteries; also capillaries (capillaritis) |
| Extravascular granuloma | Palisading histiocytes and giant cells - the "allergic granuloma" |
| Eosinophilic infiltration | Perivascular eosinophils in the early (prevasculitic) phase; diffuse tissue eosinophilia |
| Eosinophilic pneumonia | Similar to idiopathic chronic eosinophilic pneumonia when present |
| Diffuse alveolar hemorrhage | With capillaritis (rare) |
Note: The pathologic lesions only rarely comprise all characteristic features on a single biopsy from one organ.
Murray & Nadel's (Ch. 96, Fig. 96.5)
6. Three Classic Phases
Three distinct phases have been described, though they are not seen in all patients, do not necessarily occur in this order, and may coincide:
Phase 1 - Prodromal Allergic Phase
- Atopy, allergic rhinitis, sinusitis (with or without nasal polyposis), asthma
- May last several years (mean: asthma precedes vasculitis by 3-9 years; range 0-61 years)
- Asthma is generally severe and corticosteroid-dependent, presenting at a mean age of ~35 years
Phase 2 - Eosinophilic Phase
- Prominent peripheral blood and tissue eosinophilia
- Manifestations may remit and recur over this time period
- Differential: parasitic infection, chronic eosinophilic pneumonia, hypereosinophilic syndrome
Phase 3 - Vasculitic Phase
- Systemic vasculitis; may be life-threatening
- Constitutional symptoms (asthenia, weight loss, fever, arthralgias, myalgias) herald extrapulmonary vasculitis
Fishman's Pulmonary Diseases and Disorders (block 15); Murray & Nadel's (Ch. 96)
7. Clinical Features
A. Pulmonary
- Asthma present in 96-100% of cases - this is the single most constant feature
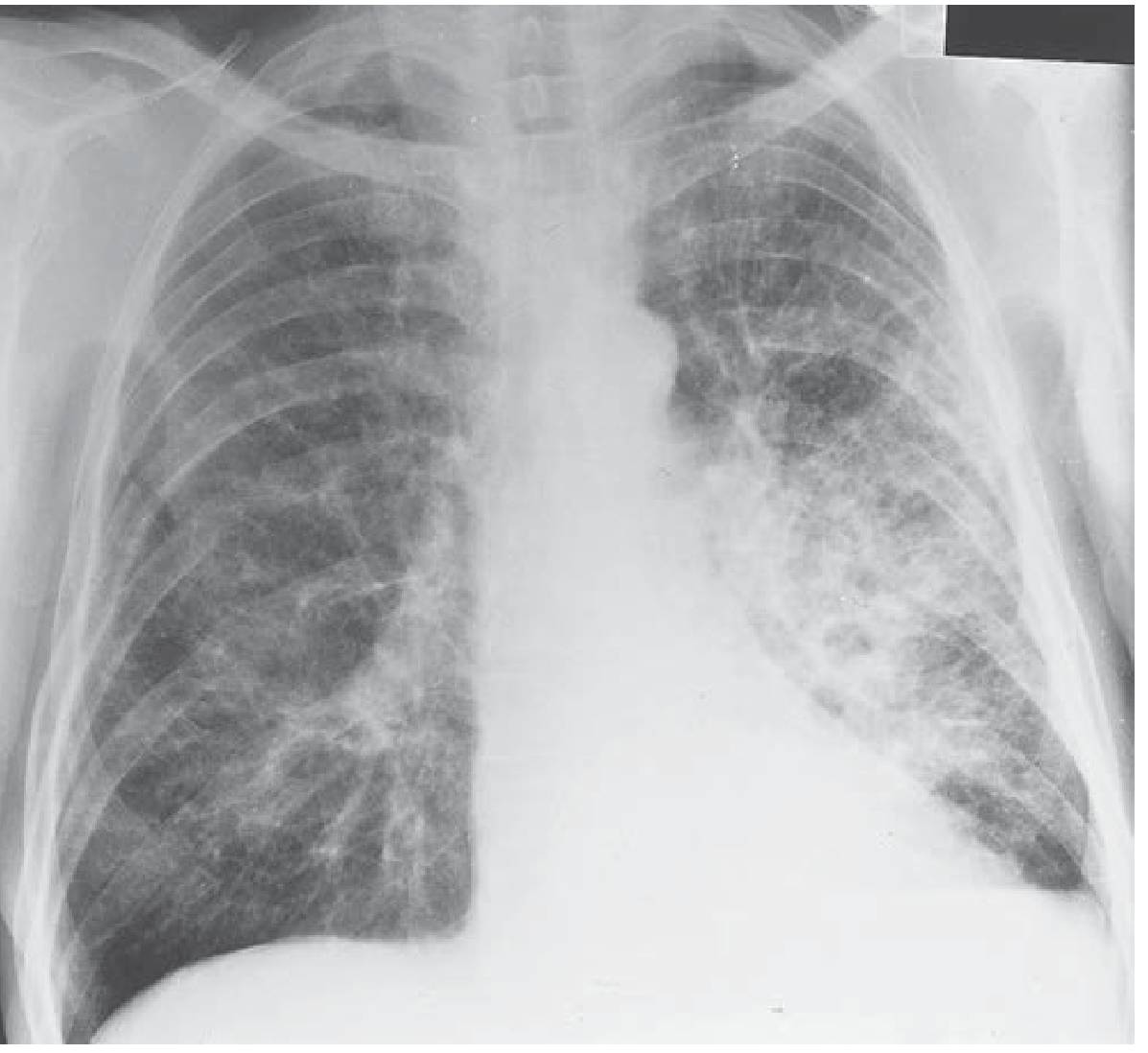
- Focal infiltrates on chest radiograph in 30-70% of cases
- Parenchymal involvement (alveolar infiltrates or nodules) in 38%
- Transient, migratory alveolar-type infiltrates with predominantly peripheral distribution - indistinguishable from chronic eosinophilic pneumonia (most common finding)
- Occasionally nodular lesions
- Pleural effusions in ~10%
- Diffuse Alveolar Hemorrhage (DAH): exceedingly rare in EGPA (in contrast to GPA and MPA)
- In contrast to GPA, no destructive upper airway lesions or nasal septal perforation
B. Upper Airway
- Chronic rhinitis in ~75% of cases
- Relapsing paranasal sinusitis, nasal polyposis with eosinophilic infiltration on histopathology
- Crusty rhinitis may be present, but much less severe than GPA
- Mild-to-moderate hearing impairment is frequent
C. Cardiac (16-56%)
- Most feared complication; may be severe and lead to cardiac failure, sudden death
- Primarily due to eosinophilic myocarditis (most common); less commonly from coronary arteritis or endomyocarditis
- Often insidious and asymptomatic - may be recognized only when left ventricular failure/dilated cardiomyopathy has developed
- Can require heart transplantation
- Conduction abnormalities, systolic or diastolic dysfunction, intracavitary thrombus, pericarditis
- Every suspected EGPA patient must have ECG, echocardiography, and serum troponin I + NT-proBNP
- Cardiac MRI (late gadolinium enhancement) is the preferred method to confirm involvement
D. Neurological (63-93%)
- Mononeuritis multiplex is the most frequent form of peripheral nerve involvement - more frequent than in GPA/MPA
- Can result from vasculitis of the vasa nervorum
E. Skin (50-78%)
- Palpable purpura, subcutaneous nodules, urticarial lesions
F. Renal (16-49%)
- Less prominent than in GPA and MPA
- Does not generally lead to renal failure (in contrast to GPA/MPA)
- Glomerulonephritis less common
G. Gastrointestinal (17-58%)
- Eosinophilic gastroenteritis, perforation, ischemia, bleeding
Fishman's Pulmonary Diseases and Disorders (blocks 13 and 15); Murray & Nadel's (Ch. 96)
8. Laboratory Findings
| Parameter | Finding |
|---|---|
| ESR, CRP | Elevated in >80% during acute phase/exacerbations |
| Blood eosinophil count | Elevated in >80% during active disease; absolute count typically >1500/μL |
| ANCA | p-ANCA (MPO-ANCA) in 30-70% |
| BAL | Eosinophilia |
ANCA Clinical Phenotyping:
- ANCA-positive subset: Higher incidence of renal involvement, DAH, glomerulonephritis, cutaneous vasculitis - shares features with GPA and MPA
- ANCA-negative subset: Features overlap with hypereosinophilic syndrome - cardiac manifestations, migratory lung opacities (eosinophilic pneumonia) predominate; these two subgroups may have differing genetic predispositions
Fishman's Pulmonary Diseases and Disorders (block 13); Murray & Nadel's (Chs. 87 and 96)
9. Diagnosis
ACR/EMA Classification Criteria (1990 ACR - widely used):
- Asthma
- Eosinophilia >10% on peripheral blood differential
- Mononeuropathy or polyneuropathy
- Non-fixed pulmonary infiltrates
- Paranasal sinus abnormality
- Biopsy containing a blood vessel with extravascular eosinophils
Presence of 4 or more criteria yields sensitivity of 85% and specificity of 99.7%.
Tissue biopsy showing characteristic features (extravascular granuloma, vasculitis, eosinophilic infiltration) is definitive but not always required in typical cases.
Fishman's Pulmonary Diseases and Disorders (block 15)
10. Differential Diagnosis
- Hypereosinophilic syndrome
- Idiopathic chronic eosinophilic pneumonia
- GPA (Granulomatosis with Polyangiitis)
- Microscopic Polyangiitis
- Allergic bronchopulmonary aspergillosis (ABPA)
- Parasitic infections
- Drug-induced eosinophilic syndromes
- Polyarteritis nodosa
Distinguishing EGPA from these: presence of ANCA, serology for Aspergillus, finding of vasculitis + granulomas on biopsy, and molecular biologic analysis (in cases of idiopathic hypereosinophilic syndrome).
Murray & Nadel's (Ch. 96)
11. Prognosis - Five Factor Score (FFS)
The French Vasculitis Study Group validated the Five-Factor Score (FFS) for EGPA:
| Factor | Score |
|---|---|
| Renal insufficiency (creatinine >150 µmol/L or proteinuria >1g/day) | +1 |
| Clinically significant gastrointestinal disease | +1 |
| Cardiac symptoms/cardiomyopathy | +1 |
| Absence of upper airway (ENT) involvement | +1 |
| Age ≥65 years | +1 |
5-year mortality rates:
- FFS = 0: 9%
- FFS = 1: 21%
- FFS ≥ 2: 40%
Additional predictors of poor prognosis: severe alveolar hemorrhage, eye involvement (scleritis), fulminant mononeuritis multiplex.
Murray & Nadel's (Ch. 87); Fishman's Pulmonary Diseases and Disorders (block 15)
12. Treatment
A. Glucocorticoids (First Line - All Patients)
- Mainstay of therapy; control disease in the majority of cases (>80-90%)
- Oral prednisone 1 mg/kg/day for 3-4 weeks, then tapered to 5-10 mg/day by 12 months
- IV methylprednisolone bolus (15 mg/kg/day for 1-3 days) for severe cases especially myocardial involvement
- Prolonged low-dose steroids are often required for long-term control
B. Cyclophosphamide (for Severe/Organ-Threatening Disease)
- Preferred agent for: FFS ≥ 2, cardiac involvement, GI involvement, CNS involvement, mononeuritis multiplex, DAH, ANCA-positive patients
- IV cyclophosphamide: 0.6 g/m² at days 1, 15, 30; then 0.7 g/m² every 3 weeks (3 more infusions)
- Reduces to 500 mg fixed-dose pulses every 2-3 weeks in patients >65 years
- Associated with improved survival in severe EGPA with higher FFS
- Should be replaced by azathioprine for maintenance after remission is achieved at 4-6 months
C. Remission Maintenance (18-24 months)
- Azathioprine (preferred)
- Methotrexate (0.25 mg/kg/week) - alternative to azathioprine
- Mycophenolate mofetil - may be less effective than azathioprine for preventing relapses
- In patients with no poor prognostic criteria: glucocorticoids alone may suffice for maintenance
Glucocorticoid-sparing agents (non-severe disease or inability to taper steroids below 10 mg/day):
- Azathioprine, methotrexate, or mycophenolate mofetil
D. Biologic Therapy - Mepolizumab (Anti-IL-5)
- Mepolizumab is a humanized monoclonal antibody against IL-5 (key cytokine for eosinophil differentiation and survival)
- MIRRA Trial (Phase III RCT): Mepolizumab vs. placebo as add-on therapy in relapsing/refractory EGPA
- 28% vs 3% had ≥24 weeks of accrued remission (P<0.001)
- Higher percentage in remission at weeks 36 and 48 (32% vs 3%; P<0.001)
- Best suited for: EGPA not controlled with glucocorticoids alone, low FFS, ANCA-negative EGPA patients
- Note: mepolizumab alone or with <5 mg/day prednisolone does not maintain remission in the majority
- Reslizumab (anti-IL-5) and benralizumab (anti-IL-5 receptor) are under investigation
E. Rituximab (Anti-CD20)
- Used in: refractory EGPA or when cyclophosphamide is contraindicated
- Retrospective data: improvement in 76.8% at 6 months, 82.8% at 12 months, 93.2% by 24 months
- Relapses (particularly asthma and ENT) in 54% by 24 months
- ANCA-positive subset: more sustained response
- Active trials: REOVAS (vs. cyclophosphamide for induction) and MAINRITSEG (vs. azathioprine for maintenance)
- Data remain insufficient to definitively recommend rituximab broadly for EGPA
F. Plasma Exchange (TPE)
- Rarely used; theoretically useful in ANCA-positive EGPA patients with severe pulmonary-renal syndrome failing CS and cyclophosphamide
Fishman's Pulmonary Diseases and Disorders (blocks 13 and 15); Murray & Nadel's (Chs. 87 and 96)
13. Disease Severity Classification (Treatment Stratification)
| Class | Features | Treatment |
|---|---|---|
| Non-organ-threatening | Rhinosinusitis, exanthem, pulmonary nodules without systemic organ involvement | Glucocorticoids ± MTX/AZA/MMF |
| Organ- or life-threatening | Rapidly progressive renal disease, pulmonary hemorrhage, motor neuropathy, cardiac involvement, GI bleeding | Cyclophosphamide + glucocorticoids OR Rituximab + glucocorticoids |
| Refractory | Disease flares during steroid taper or requires ≥7.5 mg prednisone to control | Escalate to cyclophosphamide or biologics (mepolizumab) |
Murray & Nadel's (Ch. 87, Table 87.4)
14. Monitoring
- Birmingham Vasculitis Activity Score (BVAS v3.0): Quantifies disease activity
- Vasculitis Damage Index (VDI): Tracks cumulative organ damage
- Routine cardiac surveillance for all EGPA patients (ECG, echo, troponin, NT-proBNP)
- Cardiac MRI for suspected myocardial involvement
15. Summary of Key Distinguishing Features of EGPA vs. GPA/MPA
| Feature | EGPA | GPA | MPA |
|---|---|---|---|
| Asthma | Always present | Absent | Absent |
| Eosinophilia | Universal | Absent | Absent |
| ANCA | 30-70% (p-ANCA/MPO) | 70-90% (c-ANCA/PR3) | 50-80% (p-ANCA) |
| Upper airway destruction | Rare | Common (saddle nose, septal perforation) | Rare |
| DAH | Rare | Common | Common |
| Renal failure | Less common | Common | Common |
| Mononeuritis multiplex | Very common (63-93%) | Less common | Less common |
| Cardiac involvement | Common (16-56%) | Rare | Rare |
| Granulomas | Yes (eosinophilic, extravascular) | Yes (necrotizing) | No |
Sources:
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set - Chapters on DAH/Vasculitis and EGPA Clinical Presentation/Treatment
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set - Chapters 87 (Pulmonary Vasculitis) and 96 (Eosinophilic Lung Diseases)
This is a shared conversation. Sign in to Orris to start your own chat.