Explain the laboratory approach to diagnose a male child with repeated joint bleeding. Pathology 3 marks question. Max try to consize the matter. And try to give in flow charts diagrams classification tables
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have all the necessary content to write a comprehensive, concise, exam-oriented answer. Let me compose it.
Laboratory Approach to Diagnose a Male Child with Repeated Joint Bleeding (Hemarthrosis)
Clinical Context
A male child with recurrent hemarthrosis almost certainly has a coagulation factor deficiency of the intrinsic pathway - classically Hemophilia A (Factor VIII deficiency) or Hemophilia B (Factor IX deficiency), both X-linked recessive disorders. The lab workup follows a stepwise, tiered approach.
STEP 1 - Initial Clue: Bleeding Pattern Analysis
| Feature | Coagulation Factor Deficiency | Platelet/Vascular Disorder |
|---|---|---|
| Bleeding site | Deep - joints, muscles | Superficial - skin, mucosa |
| Lesions | Hematomas, hemarthrosis | Petechiae, ecchymoses |
| Onset | Delayed after trauma | Immediate / spontaneous |
| Sex | Males (X-linked) | Either sex |
A male child with joint bleeding = suspect coagulation factor deficiency (especially Hemophilia A/B)
STEP 2 - Screening Tests (Tier 1)
| Test | Hemophilia A/B | Normal Value |
|---|---|---|
| CBC + Platelet count | Normal | 1.5-4 x 10⁵/µL |
| PT (Prothrombin Time) | NORMAL | 11-14 sec |
| aPTT (activated Partial Thromboplastin Time) | PROLONGED | 25-35 sec |
| TT (Thrombin Time) | Normal | ~15 sec |
| Bleeding Time | Normal | 2-9 min |
Key Pattern: Isolated prolonged aPTT + Normal PT = intrinsic pathway defect
STEP 3 - Diagnostic Algorithm (Flowchart)
From the Tietz Textbook of Laboratory Medicine (7th ed.):
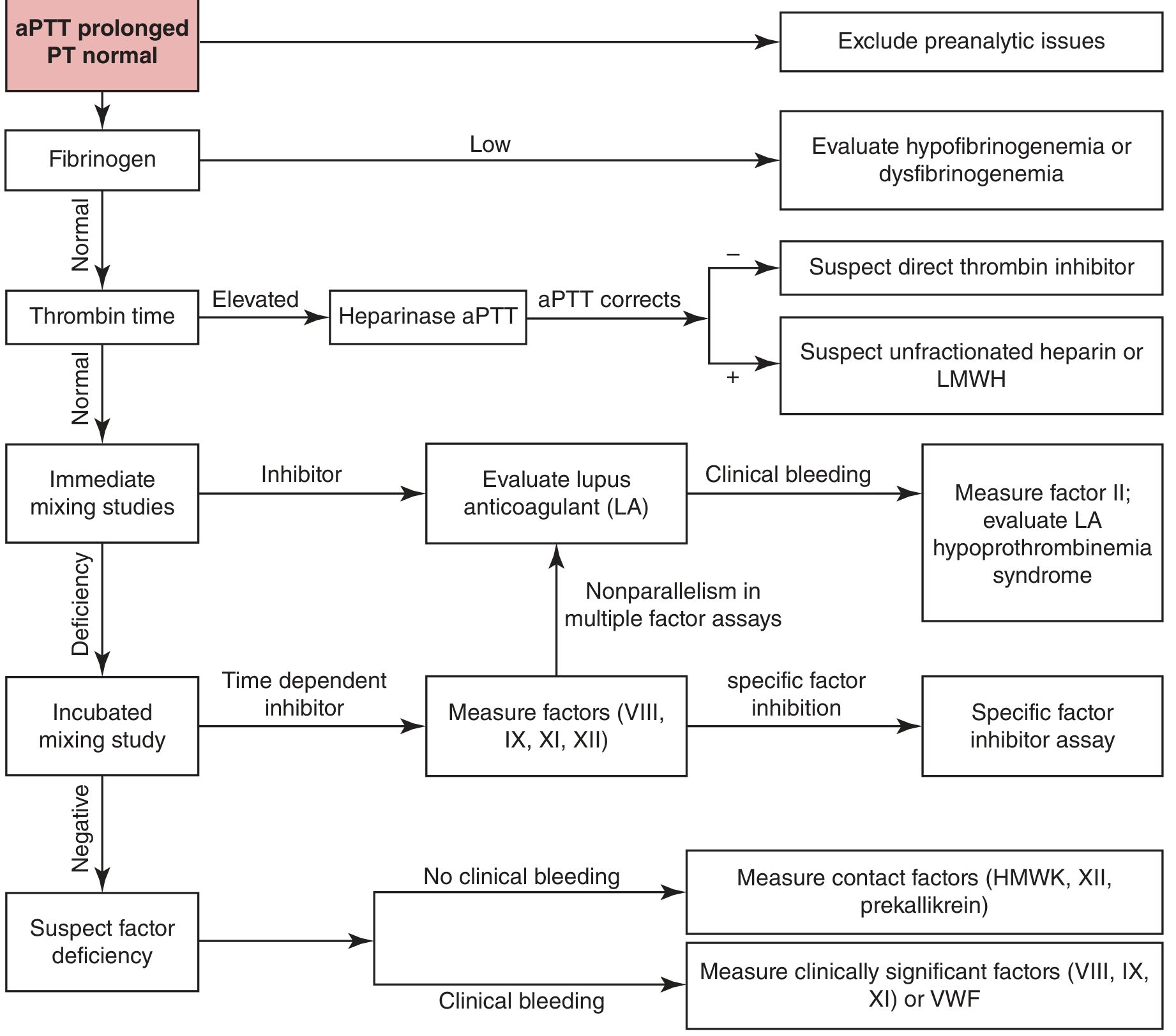
Simplified version:
ISOLATED PROLONGED aPTT + NORMAL PT
|
v
Check Fibrinogen (TT normal?)
|
NORMAL
|
v
MIXING STUDY (1:1 with Normal Plasma)
/ \
CORRECTS DOES NOT CORRECT
(Factor (Inhibitor present)
Deficiency) |
| --> LA / FVIII inhibitor assay
v
Incubated Mixing Study
|
CORRECTS
|
v
Measure Factors VIII, IX, XI, XII
|
_______________
| |
VIII low IX low
(Hemophilia A) (Hemophilia B)
STEP 4 - Mixing Study (1:1 Inhibitor Screen)
Principle: Mix patient plasma 1:1 with normal pooled plasma.
- If factor is 0% in patient + 100% in normal plasma → mixture = 50% → sufficient to correct aPTT
- Correction = Factor Deficiency
- No correction = Inhibitor (e.g., FVIII antibody, lupus anticoagulant)
| Result | Interpretation |
|---|---|
| Immediate correction | Factor deficiency |
| Immediate + incubated correction | Factor deficiency (non-time-dependent) |
| Corrects immediately but not after incubation | Time-dependent inhibitor (e.g., FVIII inhibitor) |
| No correction at any time | Immediate inhibitor (e.g., lupus anticoagulant) |
STEP 5 - Specific Factor Assays (Tier 3 - Confirmatory)
| Factor | Hemophilia A | Hemophilia B | Hemophilia C |
|---|---|---|---|
| Factor VIII activity | LOW | Normal | Normal |
| Factor IX activity | Normal | LOW | Normal |
| Factor XI activity | Normal | Normal | LOW |
| Factor XII, HMWK, PK | Normal | Normal | Normal (no bleeding!) |
Contact factors (XII, HMWK, prekallikrein) prolong aPTT but do NOT cause clinical bleeding - exclude them.
STEP 6 - Severity Classification (Hemophilia A/B)
| Severity | Factor Activity | Clinical Features |
|---|---|---|
| Severe | < 1 IU/dL (<1%) | Spontaneous hemarthrosis, muscle bleeds |
| Moderate | 1-5 IU/dL (1-5%) | Bleeding after minor trauma |
| Mild | 5-40 IU/dL (5-40%) | Bleeding only after significant trauma/surgery |
Severity correlates directly with factor activity level (Tietz Laboratory Medicine, 7th ed., p. 3123)
STEP 7 - Additional/Confirmatory Tests
| Test | Purpose |
|---|---|
| One-stage aPTT-based factor assay | Standard measurement |
| Two-stage / Chromogenic assay | Detects "mild discrepant Hemophilia A" (up to 40% of mild cases may be missed by one-stage alone) |
| Bethesda assay | Quantifies inhibitor titer (BU/mL) if inhibitor suspected |
| vWF antigen + ristocetin cofactor (VWF:RCo) | Rule out Type 2N VWD (mimics Hemophilia A) |
| Genetic testing (F8/F9 gene mutation) | Confirms diagnosis, carrier detection, prenatal testing |
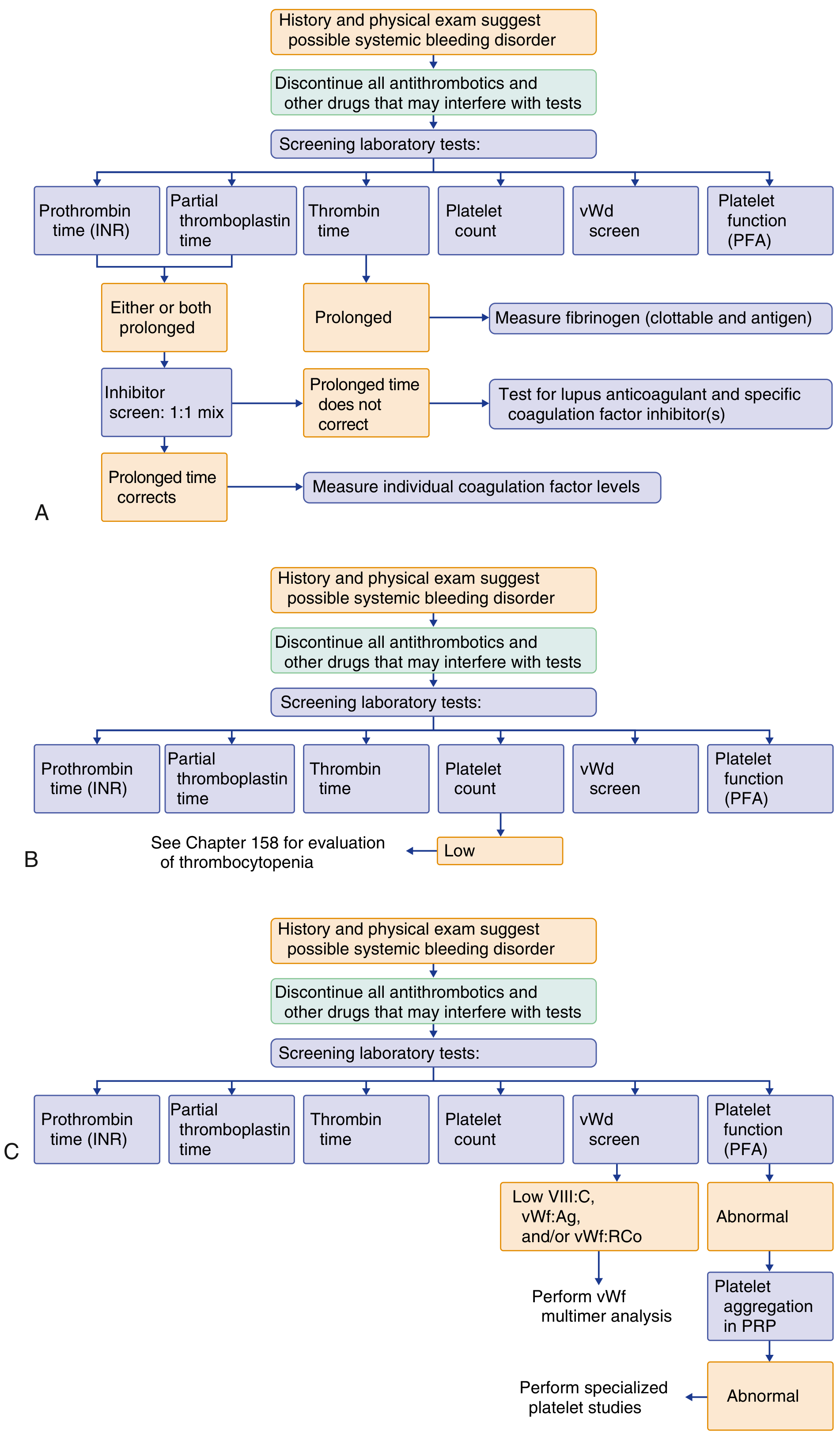
COMPLETE SUMMARY FLOWCHART
From Goldman-Cecil Medicine:
Quick Memory Aid
Male Child + Joint Bleeding
|
Platelet/Vascular disorders UNLIKELY (no petechiae, deep bleeding)
|
COAGULATION DISORDER
|
aPTT ↑ + PT Normal = INTRINSIC PATHWAY
|
Mixing Study Corrects = FACTOR DEFICIENCY
|
Factor VIII ↓ = Hemophilia A (1 in 5,000 males)
Factor IX ↓ = Hemophilia B (1 in 30,000 males)
Factor XI ↓ = Hemophilia C (rare, autosomal)
Sources:
- Tietz Textbook of Laboratory Medicine, 7th Edition - Inherited Coagulation Disorders, pp. 3121-3124
- Goldman-Cecil Medicine - Screening Tests of Hemostasis, p. 1800-1801
- Tietz: Factor VIII Deficiency (Hemophilia A), Factor IX Deficiency (Hemophilia B)
This is a shared conversation. Sign in to Orris to start your own chat.