You are a prosthodontics professor and i am your final year BDS student.Now teach me full occlusion topic with easiest explanation also build my concepts and explain difficult terminologies. Also explain by using labelled diagram wherever needed
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Alright, settle in - this is going to be your complete, concept-building lecture on Occlusion. I'll teach it the way I'd explain it on a whiteboard, building every idea from scratch.
🦷 OCCLUSION - Complete Lecture for Final Year BDS
PART 1: What is Occlusion? (The Foundation)
Simple definition: Occlusion is simply the contact between upper (maxillary) and lower (mandibular) teeth when the jaws come together.
Think of it like this: your upper and lower teeth are two gears. When those gears mesh together - that's occlusion.
Remember: Occlusion is NOT just about biting. It includes any tooth contact - chewing, swallowing, speaking, even resting contact.
PART 2: The Key Players - The TMJ
Before teeth can meet, the jaw must move. The joint that controls all jaw movement is the Temporomandibular Joint (TMJ).
TMJ Anatomy - Here's the actual diagram:
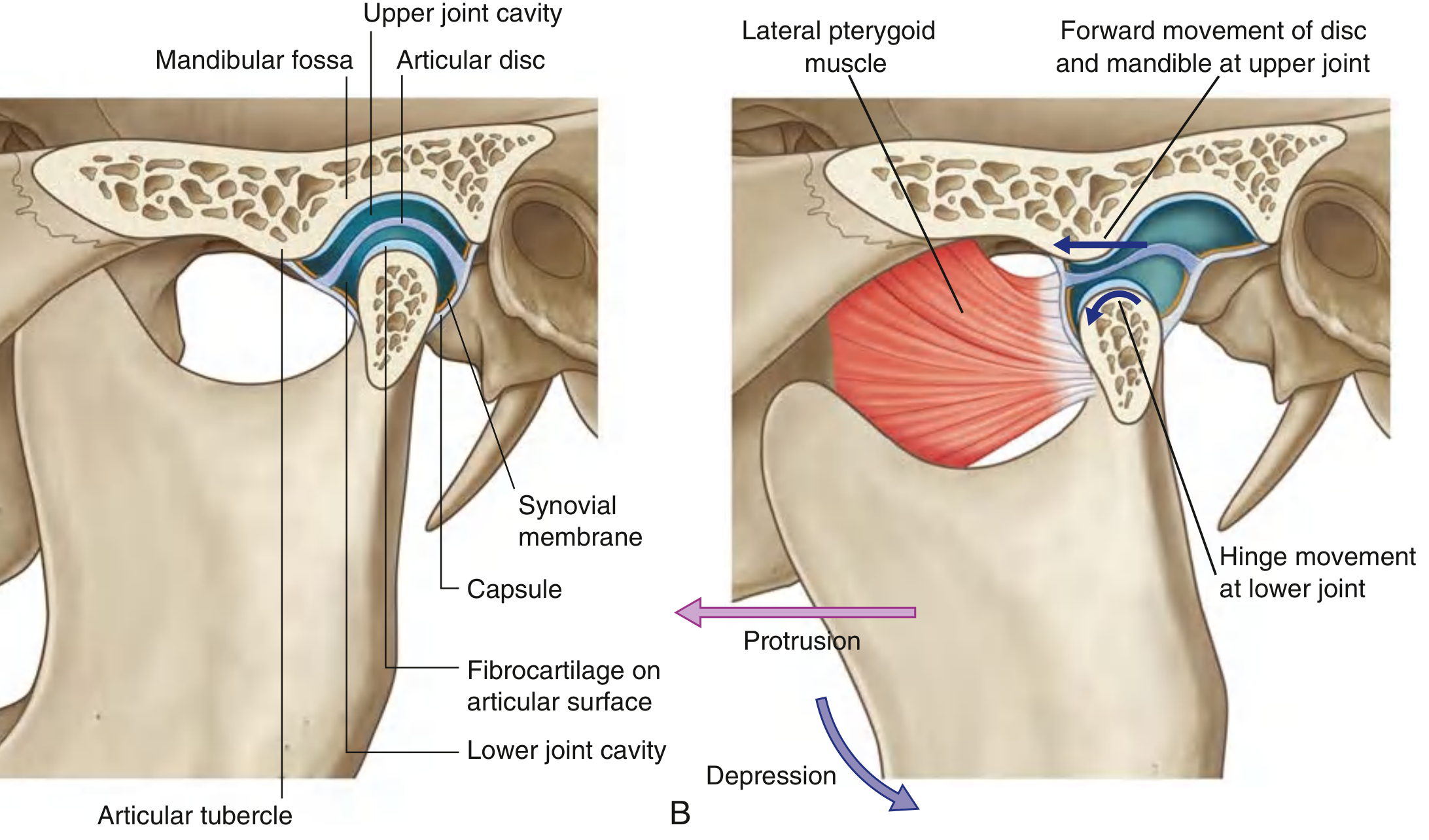
Key structures (memorize these):
| Structure | Simple Explanation |
|---|---|
| Mandibular fossa | The socket in the temporal bone - the "cup" |
| Mandibular condyle | The rounded head of the jaw - the "ball" |
| Articular disc | A fibrocartilage cushion sitting between ball and cup |
| Upper joint cavity | Above the disc - allows gliding/translation |
| Lower joint cavity | Below the disc - allows hinge/rotation |
| Lateral pterygoid | The muscle that pulls the disc and condyle forward |
Two Movements in One Joint
The TMJ is unique - it does two things at once:
- Lower compartment = HINGE (rotation) - mouth opens slightly
- Upper compartment = GLIDE (translation) - condyle slides forward onto the articular eminence for wider opening
Easy memory: "Lower = rotation, Upper = translation" - L comes before U, rotation comes before translation when opening your mouth.
PART 3: Critical Terminology - Jaw Positions
This is where most students get confused. Let's fix that.
3A. Centric Relation (CR)
┌─────────────────────────────────────────────────────┐
│ CENTRIC RELATION = Position of the CONDYLE │
│ │
│ The condyle is in its most superior, anterior, │
│ and medial position in the glenoid fossa │
│ WITHOUT any tooth contact │
│ │
│ This is a JOINT position, not a tooth position │
└─────────────────────────────────────────────────────┘
Simple analogy: Imagine your car's steering wheel in the perfectly centered "neutral" position. That's Centric Relation for the condyle.
- It is reproducible - you can find it again and again
- It is a border position - at the very limit of the hinge arc
- NOT dependent on teeth - even an edentulous patient has a CR
- This is why CR is used as the reference position when making dentures and occlusal records
3B. Centric Occlusion (CO) = Intercuspal Position (ICP)
┌─────────────────────────────────────────────────────┐
│ CENTRIC OCCLUSION = Position of MAXIMUM TOOTH │
│ CONTACT │
│ │
│ Upper and lower teeth are in maximum intercuspation │
│ (maximum number of teeth touching each other) │
│ │
│ This is a TOOTH position │
└─────────────────────────────────────────────────────┘
Simple analogy: CO is when you bite down fully - maximum teeth contact. Like interlocking your fingers together as tightly as possible.
3C. The CR-CO Slide (Most Important Concept!)
In a PERFECT world, CR = CO. But in most people, they do NOT coincide.
CR CO
| |
| ← usually 0.5–2mm → |
| anterior slide |
[condyle in fossa] [teeth in max contact]
When you close from CR, the teeth start to contact and the mandible slides forward and slightly sideways to reach CO (maximum intercuspation). This slide is called the CR-CO discrepancy or the long centric slide.
Why this matters clinically: A large CR-CO slide creates uneven forces, which can lead to TMD (Temporomandibular Disorder), tooth wear, and muscle pain.
3D. Rest Position (Postural Rest Position)
┌──────────────────────────────────────────────┐
│ REST POSITION = Mandible at rest │
│ │
│ Muscles of mastication are at minimum │
│ activity (physiologic equilibrium) │
│ │
│ Teeth are APART - a small gap exists │
│ called the FREEWAY SPACE │
└──────────────────────────────────────────────┘
Freeway Space (Interocclusal Distance):
- The gap between upper and lower teeth when the jaw is at rest
- Normal = 2-4 mm (average 3 mm)
- Too small = denture feels "cramped," muscles fatigue
- Too large = patient looks "sunken in," speaking difficulty, clicking sounds when talking
PART 4: Angle's Classification of Malocclusion
Dr. Edward Angle (1855-1930) classified bite relationships based on where the upper first molar's mesiobuccal cusp lands relative to the lower first molar.
The Reference Point: Upper First Molar
Upper 1st Molar: The "KEY OF OCCLUSION" (Angle's term)
|
↓
Mesiobuccal cusp of upper 1st molar sits in...
|
├── ...mesiobuccal groove of lower 1st molar → CLASS I ✓
|
├── ...distal to that groove → CLASS II (lower jaw behind)
|
└── ...mesial to that groove → CLASS III (lower jaw forward)
Class I - Normal Occlusion
Upper: [ | | | | | | ]
↓ mesiobuccal cusp lands in ↓
Lower: [ | | | | | | ]
mesiobuccal groove
- The upper and lower molars are in ideal relationship
- All other teeth may still have individual rotations/crowding - that's Class I malocclusion
- The molar key is correct but individual teeth can be problematic
Class II - "Buck Teeth" / Retrognathic Mandible
The lower jaw is behind where it should be (or upper jaw is too far forward).
Class II Division 1:
- Upper incisors are proclined (flared forward)
- Deep overjet (horizontal overlap is increased)
- Usually associated with incompetent lips (can't close without strain)
Class II Division 2:
- Upper central incisors are retroclined (tipped back)
- Upper lateral incisors are proclined and overlap centrals
- Usually deep overbite (vertical overlap is increased)
- Lips are competent
CLASS II Div 1 CLASS II Div 2
┌─┐ ┌─┐
│/│ ← proclined │\│ ← retroclined
└─┘ └─┘
deep overjet deep overbite
Class III - "Underbite" / Prognathic Mandible
The lower jaw is in front of where it should be.
Lower jaw sticks out → lower teeth bite in front of upper teeth
- Can be true Class III (skeletal - large mandible)
- Or pseudo/false Class III (postural - mandible shifts forward to achieve contact)
- Common in certain ethnic populations
PART 5: Overjet and Overbite - Two Most Confused Terms
↕ OVERBITE ←→ OVERJET
(vertical) (horizontal)
Upper tooth
────────
| ↕ Overbite = vertical overlap
────────
Lower tooth
←→ Overjet = horizontal gap
| Term | Definition | Normal Value | Measured |
|---|---|---|---|
| Overjet | Horizontal distance between upper and lower incisor edges | 2-4 mm | Horizontally |
| Overbite | Vertical overlap of upper over lower incisors | 2-4 mm (1/3 of lower incisor crown) | Vertically |
Abnormal variations:
- Increased overjet = Class II div 1 appearance, proclined upper incisors
- Increased overbite = deep bite, can impinge on lower gingiva
- Reverse overjet = lower teeth in front (Class III or edge-to-edge)
- Open bite = teeth do NOT overlap at all - a space exists when back teeth contact
- Edge-to-edge = incisors meet tip to tip (0 mm overjet AND 0 mm overbite)
PART 6: Occlusal Contacts - Types and Their Functions
When upper and lower teeth contact, the type of contact matters enormously.
6A. Ideal Contacts in ICP
Cusp tip → Central fossa or marginal ridge
Upper buccal cusp → contacts lower central fossa
Lower buccal cusp → contacts upper central fossa
RULE: "Cusp to Fossa" or "Cusp to Marginal Ridge"
The ideal occlusal contact scheme is often called "cusp-fossa" relationship where each cusp tip contacts the center of a fossa or the marginal ridge area directly across from it.
6B. Cusp Types - Stamp vs. Shear
| Cusp Type | Upper Teeth | Lower Teeth | Function |
|---|---|---|---|
| Centric cusps (holding cusps) | Palatal cusps of upper | Buccal cusps of lower | Maintain vertical dimension |
| Non-centric cusps (shearing cusps) | Buccal cusps of upper | Lingual cusps of lower | Food shearing, cosmetics |
Memory trick: "BULL" - Buccal Upper Lingual Lower are the NON-centric (shearing) cusps. The centric (holding) cusps are the opposite - Upper Palatal and Lower Buccal.
PART 7: Occlusal Schemes - The Big Three
An occlusal scheme is the pattern of tooth contacts during different jaw movements.
7A. Balanced Occlusion (Bilaterally Balanced)
┌─────────────────────────────────────────────────────┐
│ Contacts on BOTH sides during ALL lateral movements │
│ │
│ Used in: COMPLETE DENTURES │
│ │
│ Why: Denture stability - bilateral contacts prevent │
│ the denture from tipping/rotating │
└─────────────────────────────────────────────────────┘
Working side = the side the jaw moves toward
Balancing side (non-working side) = the opposite side
In bilateral balance, contacts exist on BOTH working and balancing sides simultaneously during lateral excursion.
7B. Mutually Protected Occlusion (Canine Protected / Organic Occlusion)
┌─────────────────────────────────────────────────────────┐
│ Posterior teeth protect anteriors in ICP │
│ Anterior teeth protect posteriors during EXCURSIONS │
│ │
│ Used in: NATURAL DENTITION, Fixed Prosthodontics │
│ │
│ In lateral movement → ONLY CANINE contacts on │
│ working side (canine guidance) │
│ │
│ In protrusive movement → ONLY incisors contact │
└─────────────────────────────────────────────────────────┘
Why canines?
- Strong roots (longest, with dense bone)
- Good proprioception
- Located at corners - ideal for guiding lateral movements
7C. Group Function Occlusion
┌──────────────────────────────────────────────────────────────┐
│ During lateral movements → Multiple teeth on working side │
│ contact simultaneously (canine + premolars + possibly │
│ first molar) │
│ │
│ NO balancing side contacts │
└──────────────────────────────────────────────────────────────┘
This distributes force across multiple teeth rather than concentrating it all on the canine.
PART 8: Mandibular Movements and Their Guidance
The 4 Border Movements of the Mandible
Mandibular movements can be plotted in three dimensions. When you trace the extreme/border limits:
In Frontal plane:
┌───────────────┐
│ CR/ICP │ ← Maximum intercuspation
/ \
/ \ ← Lateral borders (guided by teeth/TMJ)
/ \
/ \
└─────────────────────┘
Maximum open
The POSSELT'S ENVELOPE OF MOTION - The total border path of the mandible in the sagittal plane:
ICP (Centric Occlusion)
●
/|
/ |
CR / | ← hinge arc (pure rotation)
● |
\ |
\ |
\|
● Maximum open
|
● Maximum protrusion
Envelope = the outer boundary of ALL possible jaw movements
Clinical use: When making dentures, you must record jaw movements within this envelope. Any restoration placed OUTSIDE this envelope will cause immediate trauma to teeth or joints.
PART 9: Occlusal Discrepancies and Their Effects
Premature Contact / Deflective Contact
┌──────────────────────────────────────────────────────┐
│ One tooth hits before all others during closure │
│ │
│ CR closure → one tooth contacts → mandible SLIDES │
│ to reach full CO │
│ │
│ This is a DEFLECTIVE contact │
│ (it deflects/redirects the jaw path) │
└──────────────────────────────────────────────────────┘
What it causes:
- Tooth mobility
- Bone loss around that tooth
- Muscle hyperactivity
- TMD symptoms (clicking, pain, limited opening)
Interference
Any tooth contact that occurs during lateral or protrusive excursion that is NOT part of the planned occlusal scheme.
| Type | Definition | Where |
|---|---|---|
| Working side interference | Posterior contact on the side jaw moves toward | Working side |
| Non-working/balancing interference | Posterior contact on the opposite side from jaw movement | Balancing side (most harmful) |
| Protrusive interference | Posterior contact during forward jaw movement | Posterior teeth |
Key point: Non-working (balancing) side interferences are the MOST harmful because they create a lever-like effect, concentrating enormous force on those teeth.
PART 10: Occlusal Plane and Curves
The Curve of Spee
Side view of lower arch:
Incisors Molars
* *
* *
* *
* *
* * * * * * *
The curve following the buccal cusp tips
from canine back to the last molar = CURVE OF SPEE
(also called the "anteroposterior curve")
This curve corresponds to the arc of the mandibular movement. Restorations must not violate this curve.
The Curve of Wilson
Frontal view (cross-arch):
Upper teeth
\ | /
\ | /
\ | / ← Each posterior quadrant tilts
Left \ | / lingual = Curve of Wilson
Lower * | * Right Lower
\|/
The mediolateral curve passing through the buccal and lingual cusps of each side. Lower molars tilt slightly lingually.
PART 11: Occlusion in Prosthodontics - Clinical Application
In Complete Dentures
- Always use CR as the reference - because there are no teeth, you can't use ICP
- Record the freeway space to correctly set vertical dimension of occlusion (VDO)
- Bilateral balanced occlusion is the goal - prevents denture tipping
- Set teeth on the residual ridge - occlusal plane should be at the level of the tongue in rest
In Fixed Partial Dentures (Bridges)
- The restoration must not create new interferences
- Should follow the existing curve of Spee
- Contact in ICP should be light and equal to adjacent teeth
- Canine guidance or group function must be preserved or restored
In Implants
- Implants lack the periodontal ligament - no proprioception
- Must not receive heavy occlusal forces
- "Implant-protected occlusion" - slightly lighter contact than natural teeth
- Avoid lateral forces (cantilever effect is dangerous)
PART 12: Occlusal Examination - How to Check in Clinic
Step-by-step at the chair:
-
Articulating paper - have patient bite on blue paper → marks where teeth hit
- Red/blue marks show contact points
- Large marks = heavy contact, small dots = light contact
-
Check ICP - ask patient to clench, look at marks, should be bilateral and even
-
Check for premature contact in CR - use a leaf gauge or bimanual manipulation to guide mandible to CR, then have patient close
-
Lateral excursions - move jaw side to side, check:
- Is there canine guidance (canine alone rises the posterior teeth)?
- Or group function (multiple contacts)?
- Any balancing side contact?
-
Protrusive movement - move jaw forward, check:
- Only anterior teeth should contact
- All posterior teeth should be free (posterior disclusion)
PART 13: Quick Summary Table
| Term | Simple Meaning | Type |
|---|---|---|
| Centric Relation (CR) | Condyle in its most stable joint position | Joint position |
| Centric Occlusion (CO/ICP) | Maximum tooth contact | Tooth position |
| Freeway Space | Gap between teeth at rest | Measurement |
| Overjet | Horizontal tooth overlap | Measurement |
| Overbite | Vertical tooth overlap | Measurement |
| Angle Class I | Normal molar relationship | Classification |
| Angle Class II | Lower jaw behind | Classification |
| Angle Class III | Lower jaw forward | Classification |
| Balanced occlusion | Contacts on both sides during excursion | Occlusal scheme |
| Mutually protected | Canine guidance in lateral | Occlusal scheme |
| Group function | Multiple posterior contacts in lateral | Occlusal scheme |
| Curve of Spee | AP curve of lower arch | Anatomical concept |
| Curve of Wilson | ML curve of lower arch | Anatomical concept |
| Posselt's envelope | Total border path of mandible | Movement concept |
PART 14: TMJ Anatomy (Labelled Diagram from Textbook)
Here is the actual labelled diagram of the TMJ showing the articular disc with its upper and lower compartments:
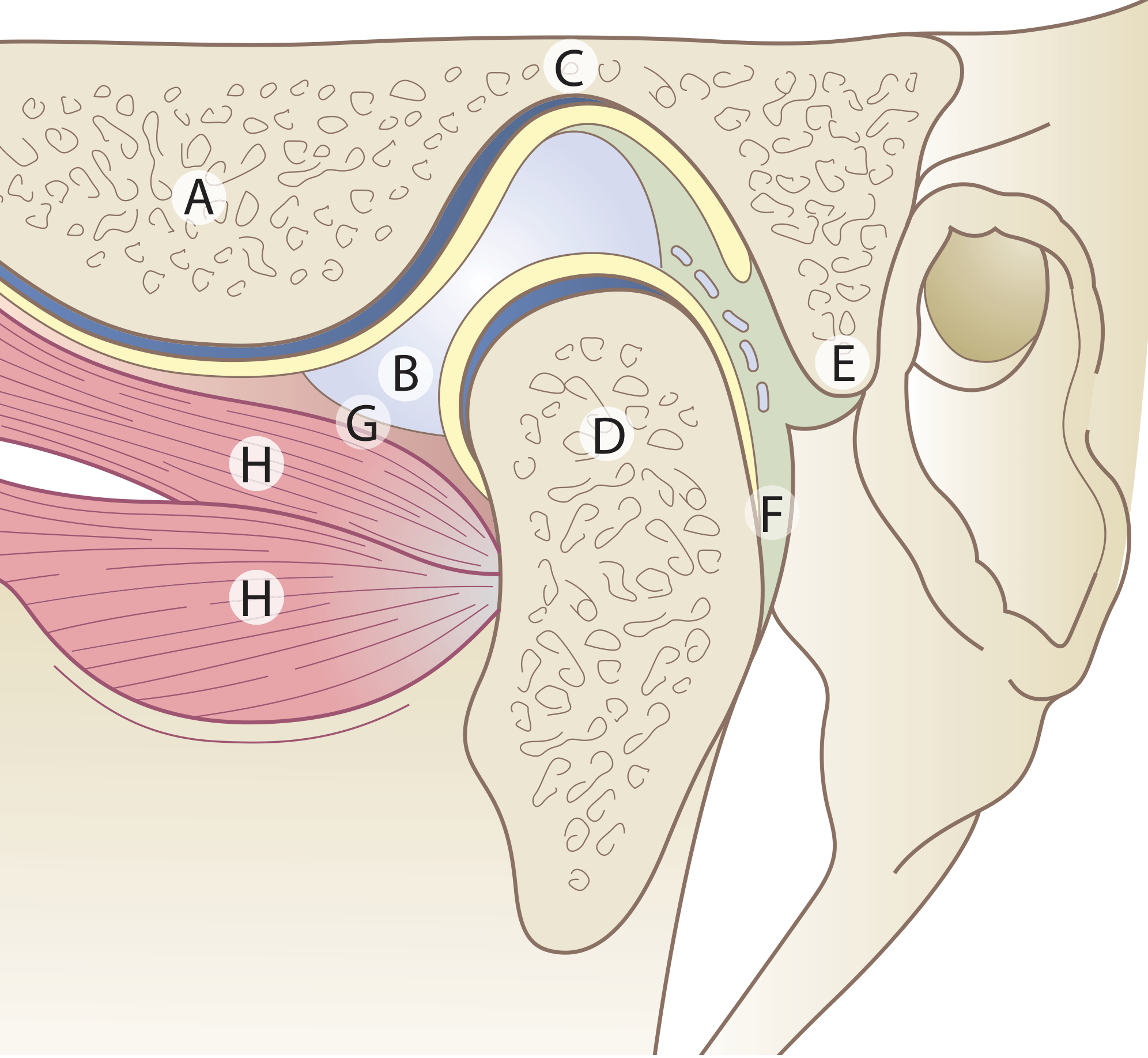
Key labels:
- A = Articular eminence (the ridge the condyle slides over during mouth opening)
- B = Articular disc (fibrocartilage "pillow" - divides the joint)
- C = Mandibular fossa (temporal bone socket)
- D = Condyle (mandibular head)
- E = Upper lamina (fibro-elastic - allows disc to spring back)
- F = Lower lamina (non-elastic collagen)
- H = Lateral pterygoid muscle (pulls disc and condyle forward)
High-Yield Exam Points (Don't Miss These!)
- CR is reproducible; CO/ICP is not always the same as CR - average slide is 0.5-2 mm
- Freeway space = 2-4 mm (if lost = patient has excess VDO; if more = insufficient VDO)
- For complete dentures - always record in CR, never in CO
- Non-working side interference is the most destructive type of occlusal interference
- Canine has the best bone support = best tooth to carry lateral guidance
- Bilateral balanced occlusion is ONLY indicated for complete dentures - harmful for natural dentition
- Angle's classification is molar-based - always check the first molar relationship first
- Posselt's envelope - any restoration violating this will cause occlusal trauma
- Articular disc surface = fibrocartilage, NOT hyaline cartilage (unlike other joints)
- Lower joint compartment = rotation; Upper = translation - separate movements in one joint
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Gray's Anatomy for Students - TMJ anatomy and movements; Clinical knowledge integrated from prosthodontic principles.
This is a shared conversation. Sign in to Orris to start your own chat.