Inj streptokinase
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Here is a comprehensive overview of Injection Streptokinase:
Streptokinase (Inj.)
Class
Fibrinolytic (Thrombolytic) agent — First generation, non-fibrin-specific
Mechanism of Action
Streptokinase is a protein derived from β-hemolytic streptococci. Unlike other plasminogen activators, it is not itself an enzyme and does not directly cleave plasminogen. Instead, it:
- Forms a 1:1 stoichiometric complex with plasminogen
- This induces a conformational change in plasminogen, exposing its active site
- The streptokinase–plasminogen complex then converts additional plasminogen molecules to plasmin
- Plasmin degrades fibrin clots → thrombolysis
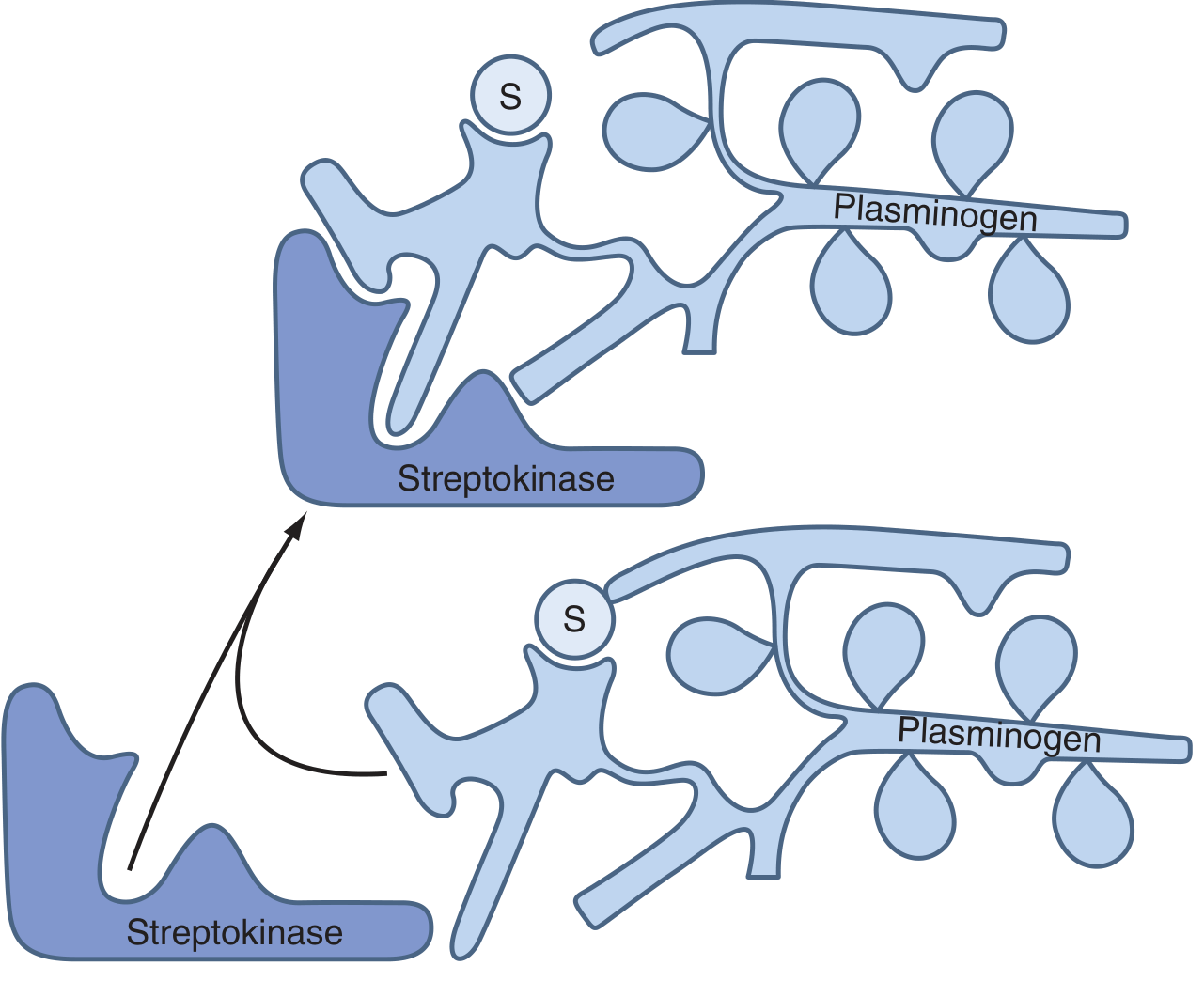
Key point: Streptokinase has no affinity for fibrin. The complex activates both free (circulating) and fibrin-bound plasminogen → produces a systemic lytic state. Plasmin overwhelms α₂-antiplasmin, degrading not only thrombus fibrin but also circulating fibrinogen and clotting factors.
Indications
| Indication | Notes |
|---|---|
| Acute MI (STEMI) | IV infusion; reduces mortality |
| Pulmonary embolism (severe/hemodynamically unstable) | IV infusion |
| Deep vein thrombosis (severe, e.g., iliofemoral, SVC syndrome) | |
| Peripheral arterial occlusion | Intra-arterial route used |
Dosage
| Indication | Regimen |
|---|---|
| Acute MI | 1.5 million units IV over 30–60 min |
| Pulmonary embolism | Loading dose: 250,000 IU over 30 min, then 100,000 IU/hr for 12–24 hrs |
| DVT / other thromboses | Loading: 250,000 units IV, then 100,000 units/hr for 24–72 hrs |
Adverse Effects
| Effect | Details |
|---|---|
| Allergic reactions | ~5% of patients — rash, fever, chills, rigors; rarely anaphylaxis |
| Hypotension | Common; due to plasmin-mediated bradykinin release from kininogen. Managed with leg elevation, IV fluids, low-dose vasopressors (dopamine/norepinephrine) |
| Bleeding | Systemic lytic state → risk of major hemorrhage |
| Antibody formation | Patients with prior streptococcal infection or previous streptokinase use may have antistreptococcal antibodies → reduced efficacy, therapeutic resistance |
Contraindications
Absolute:
- Any hemorrhagic stroke or stroke of unknown origin
- CNS neoplasm or damage
- Major trauma, surgery, or head injury within past 3 weeks
- GI bleeding within past month
- Significant ongoing bleeding
Relative:
- Ischemic stroke or TIA within past 6 months
- Anticoagulant therapy (DOAC or VKA)
- Pregnancy or within 1 week of delivery
- Noncompressible puncture site
- Traumatic resuscitation
- Advanced liver disease
- Infective endocarditis
- Active peptic ulcer disease
Note: Streptokinase is not recommended in acute ischemic stroke (increased bleeding risk at the 1.5 MU dose used for MI).
Comparison with Other Fibrinolytics
| Property | Streptokinase | tPA (Alteplase) |
|---|---|---|
| Fibrin specificity | ❌ Non-specific | ✅ Fibrin-specific |
| Systemic lytic state | Yes | Minimal |
| Antigenic | Yes (streptococcal) | No |
| Cost | Low | High |
| Mortality in MI | Reduces (less than tPA) | Greater reduction than SK |
Sources: Harrison's Principles of Internal Medicine 22E, p. 998 | Braunwald's Heart Disease, p. 1135 | Katzung's Basic & Clinical Pharmacology 16E, p. 969 | Goldman-Cecil Medicine, Table 68-4
This is a shared conversation. Sign in to Orris to start your own chat.