Retinal detachment
Reading File
search_medical_text
retinal detachment types pathophysiology diagnosis management
search_medical_image
retinal detachment fundoscopy ultrasound imaging
GradeResponse
GradeResponse
Retinal Detachment
Definition
Retinal detachment (RD) is the separation of the neurosensory retina from the underlying retinal pigment epithelium (RPE). This separation deprives the photoreceptors of their metabolic support, making it a surgical emergency — time to treatment directly determines visual outcome.
Types
| Type | Mechanism | Common Causes |
|---|---|---|
| Rhegmatogenous | Retinal break (hole/tear/flap) allows liquefied vitreous into the subretinal space | Myopia, trauma, cataract surgery, lattice degeneration |
| Tractional | Fibrovascular membranes pull the retina away without a break | Proliferative diabetic retinopathy, sickle cell, ROP |
| Exudative (serous) | Fluid accumulates beneath the retina without a break or traction | Malignant hypertension, choroidal tumors, uveitis, Vogt-Koyanagi-Harada |
Rhegmatogenous RD is the most common type.
Pathophysiology (Rhegmatogenous)
As described in Harrison's Principles of Internal Medicine (p. 966):
- A hole, flap, or tear develops — often in areas of lattice degeneration (peripheral retinal thinning)
- Liquefied vitreous enters the subretinal space through the break
- Vitreous traction on the retinal surface + hydrostatic pressure behind the retina drive progressive detachment
- If the fovea becomes involved, central vision is acutely threatened
Risk Factors
- High myopia (elongated axial length, predisposes to lattice degeneration)
- Prior cataract extraction (posterior capsule rupture, vitreous loss)
- Ocular trauma
- Family history of RD
- Posterior vitreous detachment (PVD) — especially if symptomatic with floaters/flashes
- Age > 50
Clinical Presentation
| Symptom | Significance |
|---|---|
| Floaters (new or sudden increase) | Vitreous syneresis or hemorrhage from a retinal tear |
| Photopsia (flashing lights) | Vitreoretinal traction stimulating photoreceptors |
| Curtain/shadow in peripheral vision | Detached retina casting a scotoma |
| Sudden painless vision loss | Foveal detachment — urgent |
| Afferent pupillary defect (APD) | Extensive detachment involving the macula |
Pain is notably absent — this distinguishes RD from acute angle-closure glaucoma.
Imaging
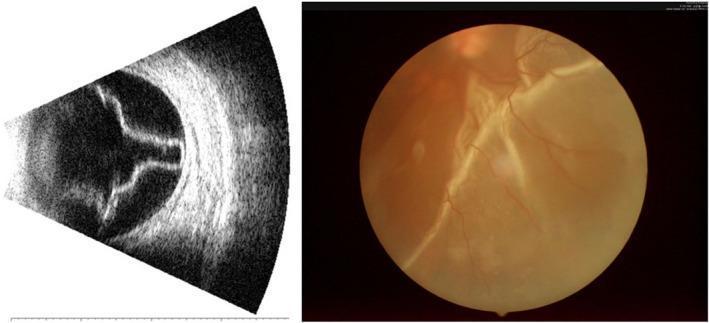
B-scan ocular ultrasound (left) demonstrating the classic V-shaped membrane anchored at the optic disc — characteristic of total/subtotal RD. Fundus photography (right) showing pale, elevated, corrugated retina with distorted vessels, contrasting with the normal flat orange-red appearance.
Diagnostic modalities
- Dilated fundoscopy — gold standard for confirming the diagnosis (Harrison's, p. 966); reveals the elevated, corrugated retina and visible break(s)
- B-scan ultrasonography — essential when media opacity (e.g., vitreous hemorrhage, dense cataract) prevents fundoscopic visualization; shows the classic V-shaped echogenic membrane tethered to the optic nerve
- OCT (optical coherence tomography) — useful for macular-off vs. macular-on determination and post-op monitoring
- Indirect ophthalmoscopy with scleral depression — identifies peripheral breaks
Management
RD is a surgical emergency. Management depends on type and extent.
Rhegmatogenous RD
| Procedure | Indication |
|---|---|
| Pneumatic retinopexy | Single superior break, phakic/pseudophakic, no significant PVR |
| Scleral buckle | Young phakic patients, inferior breaks, multiple breaks |
| Pars plana vitrectomy (PPV) | Complex cases, posterior breaks, vitreous hemorrhage, PVR, pseudophakic |
| Laser photocoagulation / cryotherapy | Treat retinal breaks before RD develops; adjunct to surgery |
- Macular-on RD = urgent surgery within hours to days (preserve central vision)
- Macular-off RD = emergent surgery; even 1-week delay worsens prognosis
Tractional RD
- Treat underlying disease (e.g., anti-VEGF + vitrectomy for proliferative diabetic retinopathy)
Exudative RD
- Treat the underlying cause (BP control, steroids for uveitis, radiation/resection for tumors)
Complications
- Proliferative vitreoretinopathy (PVR) — most common cause of surgical failure; fibrous membranes cause re-detachment
- Macular pucker / epiretinal membrane
- Persistent subretinal fluid
- Permanent vision loss if untreated
Prognosis
- Macular-on RD: >90% achieve good visual acuity with timely surgery
- Macular-off RD: ~40–75% recover reading vision; recovery can continue for up to 2 years
- Re-detachment rate: ~5–10% after primary repair
Key Differentials
| Condition | Distinguishing Feature |
|---|---|
| Posterior vitreous detachment (PVD) | Floaters/flashes without curtain; Weiss ring visible; retina attached |
| Vitreous hemorrhage | Dense floaters, red haze; no scotoma; retina may be attached |
| Retinoschisis | Smooth, convex elevation; no breaks (usually); stable |
| Choroidal detachment | Post-op or hypotony context; extends further anteriorly |
Harrison's Principles of Internal Medicine, 21st Ed., p. 966
This is a shared conversation. Sign in to Orris to start your own chat.