Decompensation in cld
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Decompensation in Chronic Liver Disease (CLD)
Definition
Decompensated cirrhosis is defined by the presence of one or more of the following complications:
- Ascites
- Variceal hemorrhage
- Hepatic encephalopathy
- Jaundice
These arise from the two main consequences of cirrhosis: portal hypertension and liver insufficiency.
— Goldman-Cecil Medicine, p. 1613
Natural History
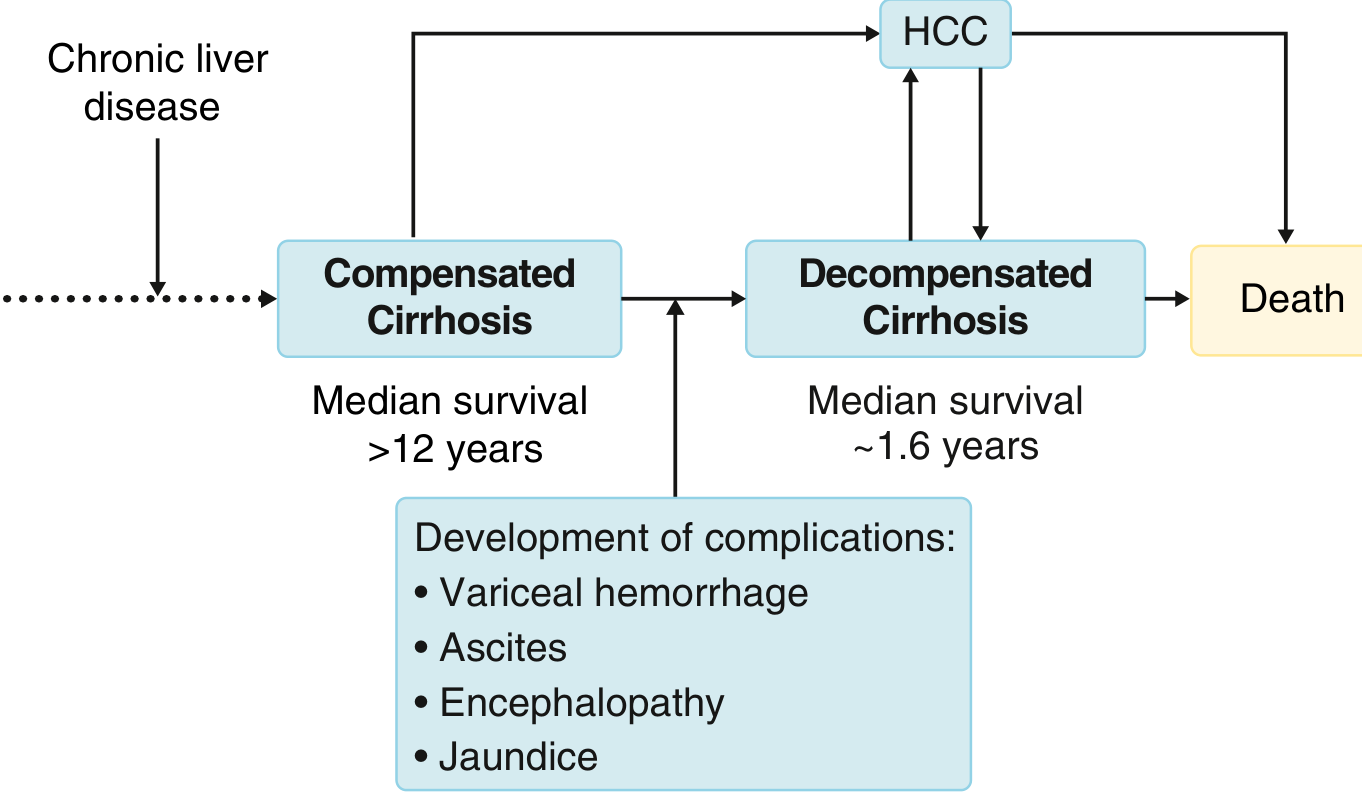
FIGURE: Natural history of cirrhosis. Any CLD leads to cirrhosis. Compensated cirrhosis has a median survival >12 years; once decompensation occurs, median survival falls to ~1.6 years. HCC can develop at any stage and precipitate decompensation.
Pathophysiology of Each Complication
1. Ascites
The sequence: cirrhosis → portal hypertension → splanchnic vasodilation → decreased effective arterial blood volume → activation of RAAS + SNS + ADH → renal sodium and water retention → ascites.
- Splanchnic vasodilation (mediated by nitric oxide) causes pooling of blood in the splanchnic bed.
- The kidney perceives this as "underfilling" and retains Na⁺ and water.
- The most severe form is refractory ascites, and further renal vasoconstriction leads to hepatorenal syndrome (HRS).
2. Variceal Hemorrhage
- Portal hypertension causes formation of portosystemic collaterals (varices) — most dangerous at the gastroesophageal junction.
- Varices develop when hepatic venous pressure gradient (HVPG) exceeds 10 mmHg; they bleed when HVPG exceeds 12 mmHg.
- 1-year mortality from a first bleed is ~20%; rebleeding occurs in ~60% within 1–2 years without prophylaxis.
3. Hepatic Encephalopathy (HE)
- Brain dysfunction caused by liver insufficiency and/or portosystemic shunting.
- Ammonia — normally detoxified by the liver — accumulates in the systemic circulation due to collateral shunting and reduced hepatocyte function.
- Ammonia damages astrocytes → Alzheimer type II astrocytosis.
- Upregulates peripheral-type benzodiazepine receptors → ↑ neurosteroids → ↑ GABA-ergic tone → cortical depression.
- Other toxins: manganese deposits in the globus pallidus → impaired motor function.
4. Jaundice
- Results from the liver's inability to excrete bilirubin (liver insufficiency).
- In cholestatic diseases (PBC, PSC), jaundice may reflect biliary damage more than hepatocyte failure.
- Prolonged PT/INR and encephalopathy help distinguish causes.
5. Cardiopulmonary Complications
- Cirrhotic cardiomyopathy: Hyperdynamic circulation → eventual high-output heart failure with decreased peripheral O₂ utilization.
- Hepatopulmonary syndrome (HPS): Pulmonary vasodilation (capillaries dilated up to 500 μm vs. normal 8 μm) → functional right-to-left shunt → arterial hypoxemia.
- Portopulmonary hypertension (PPH): Vasoconstrictive substances bypass hepatic metabolism → endothelial proliferation + vasoconstriction + in situ thrombosis → irreversible pulmonary hypertension.
Precipitants of Acute Decompensation / Acute-on-Chronic Liver Failure (ACLF)
In previously stable patients, sudden decompensation can be triggered by:
- Infection (especially SBP, pneumonia, UTI)
- GI bleeding
- Hepatitis D superinfection (in chronic HBV)
- Emergence of antiviral resistance (viral hepatitis)
- Sepsis
- Acute cardiac failure
- Superimposed hepatotoxin/drug injury
- Alcohol binge (in alcohol-related CLD)
— Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine
Staging (Baveno Criteria)
| Stage | Features | Median Survival |
|---|---|---|
| Compensated | No complications; often asymptomatic | >12 years |
| Decompensated | Ascites, variceal bleed, HE, or jaundice | ~1.6 years |
Prognostic Scores
- Child-Pugh score: Incorporates bilirubin, albumin, PT, ascites, encephalopathy.
- MELD score (Model for End-stage Liver Disease): Uses bilirubin, creatinine, INR — used for transplant prioritization and prognosis. Higher MELD = worse prognosis.
Key Management Principles
| Complication | Key Interventions |
|---|---|
| Ascites | Salt restriction, diuretics (spironolactone ± furosemide), large-volume paracentesis + albumin for refractory ascites |
| Variceal bleeding | IV terlipressin/octreotide, endoscopic band ligation/sclerotherapy, prophylactic antibiotics, TIPS for refractory cases |
| Hepatic encephalopathy | Identify/treat precipitant, lactulose (first-line), rifaximin (maintenance), dietary protein adjustment |
| HRS | Albumin + vasoconstrictors (terlipressin), TIPS, liver transplantation |
| Jaundice/liver failure | Treat underlying cause; consider transplant evaluation |
| HPS | O₂ supplementation; liver transplant is curative |
| SBP (spontaneous bacterial peritonitis) | IV cefotaxime/ceftriaxone + IV albumin; norfloxacin prophylaxis thereafter |
Liver transplantation remains the definitive treatment for decompensated cirrhosis not responsive to medical therapy.
— Goldman-Cecil Medicine, Chapter 139; Robbins & Kumar Basic Pathology, Chapter 14; Sleisenger & Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.