Heart failure as per harrison
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have enough comprehensive content. Let me compile the full Harrison's-based answer on Heart Failure.
Heart Failure - Harrison's Principles of Internal Medicine, 22nd Edition (2025)
(Chapter 264: Heart Failure: Pathophysiology and Diagnosis | Chapter 265: Management)
1. DEFINITION
The AHA/ACC/HFSA defines HF as a complex clinical syndrome with symptoms and signs that result from any structural or functional impairment of ventricular filling or ejection of blood.
The ESC definition emphasizes cardinal symptoms (breathlessness, ankle swelling, fatigue) that may be accompanied by signs (elevated JVP, pulmonary crackles, peripheral edema) due to a structural and/or functional cardiac abnormality resulting in elevated intracardiac pressures and/or inadequate cardiac output at rest and/or during exercise.
A universal definition was proposed that is comprehensive with near-universal applicability, prognostic/therapeutic validity, and acceptable sensitivity/specificity.
- The older term "congestive heart failure" is less preferred because some patients present without volume overload signs.
- "Cardiomyopathy" and "LV dysfunction" are broader terms for myocardial structural/functional disorders that may lead to HF.
2. EPIDEMIOLOGY
- ~6.7 million American adults are treated for HF; >600,000 new cases/year
- Globally, an estimated 56.2 million people have HF
- 5-year survival ~50% in primary care; 1-year mortality up to 40% in severe HF
- 1 in 8 deaths in the US lists HF on the death certificate
- Racial disparities: Black individuals have the highest risk, followed by Hispanic, White, and Chinese Americans - attributed to cardiometabolic risk factors and social determinants of health
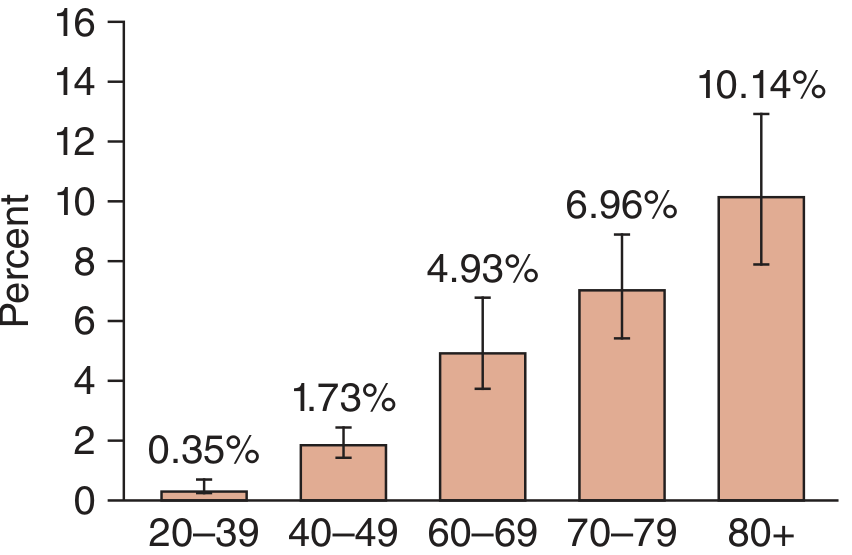
Figure 264-2: HF prevalence rises steeply with age (NHANES 2017-2020)
3. PHENOTYPES / CLASSIFICATION
| Phenotype | LVEF | Key Features |
|---|---|---|
| HFrEF (reduced EF) | ≤40% | Rich evidence base; neurohormonal antagonism is cornerstone |
| HFmrEF (mildly reduced EF) | 41-49% | Treat as HFrEF; emerging evidence |
| HFpEF (preserved EF) | ≥50% | Historically symptom-focused; SGLT-2i now emerging |
ACC/AHA Stages:
- Stage A: At risk (no symptoms, no structural disease)
- Stage B: Asymptomatic ventricular dysfunction
- Stage C: Symptomatic HF (most patients)
- Stage D: Advanced/refractory HF - salvage therapies needed
Temporal classification:
- Chronic HF: Longstanding (months to years) symptoms on therapy; episodes that resolve termed "remission" (not "stable"), since risk for decompensation/sudden death persists
- Acute HF (ADHF): Rapid onset or worsening of HF symptoms; ~80% represent worsening chronic HF, ~20% are new-onset (ACS, acute valvular dysfunction, hypertensive urgency, postcardiotomy)
4. PATHOPHYSIOLOGY
4a. Progressive Disease Model (HFrEF)
HFrEF typically involves an index event followed by months-to-years of cardiovascular remodeling:
- Index event: acute (MI), gradual (pressure/volume overload), inherited (genetic cardiomyopathy), or congenital
- Patients may be asymptomatic for prolonged periods due to compensatory mechanisms that ultimately contribute to disease progression
4b. Ventricular Remodeling
| Load Type | Pattern | Example |
|---|---|---|
| Pressure overload | Concentric hypertrophy (mass > chamber volume) | Hypertension, aortic stenosis |
| Volume overload | Eccentric hypertrophy (increased cavity size) | Aortic/mitral regurgitation |
At the cellular/molecular level:
- Myocyte hypertrophy and interstitial fibrosis
- Alterations in calcium-handling and cytoskeletal protein function
- Reexpression of fetal genes
- Cell loss via necrosis and apoptosis
- Afterload mismatch from systemic vasoconstriction + neurohormonal failure
4c. HFpEF Pathophysiology
Less well understood than HFrEF. Original focus was diastolic dysfunction; current understanding involves a broader multisystem, inflammatory, and microvascular model with major contributions from comorbidities (obesity, diabetes, hypertension, CKD).
5. SYMPTOMS
- Dyspnea on exertion - most common early symptom; caused by elevated pulmonary venous pressure
- Orthopnea - dyspnea in recumbent position; quantified by number of pillows used
- PND (paroxysmal nocturnal dyspnea) - awakens patient 1-3 hours after sleep; relieved by sitting up
- Bendopnea - dyspnea on bending forward (elevated filling pressures)
- Fatigue and weakness - from decreased cardiac output and peripheral hypoperfusion
- Nocturia - improved CO in supine position increases renal perfusion + delayed diuretic effect
- Oliguria - sign of advanced HF (severe reduction in renal blood flow)
- Mood disturbances and poor sleep - exacerbated by nocturnal dyspnea and sleep apnea
- Cardiac cachexia - unintentional weight loss; sign of advanced/poor prognosis
6. PHYSICAL EXAMINATION
General
- Mild-moderate HF: Well nourished, comfortable at rest; dyspnea on exertion
- Severe HF: Must sit upright, anxious, diaphoretic, dyspneic at rest; pallor (anemia) or duskiness (low output); cool extremities, peripheral cyanosis
Key Signs
| Sign | Significance |
|---|---|
| Elevated JVP | Most reliable sign of volume overload |
| S3 gallop | Elevated filling pressure; marker of poor prognosis |
| Pulmonary crackles | Pulmonary edema |
| Peripheral edema | Right heart failure / fluid overload |
| Hepatomegaly, ascites | Right-sided or biventricular failure |
| Displaced/diffuse apical impulse | Dilated cardiomyopathy |
| Narrow pulse pressure | Reduced stroke volume |
7. PRECIPITATING FACTORS (Table 264-5)
Identifiable factors found in 50-90% of admissions:
Patient-related: Excess exertion/emotional stress, excess fluid/sodium intake, nonadherence with medications, heavy alcohol use
Provider-related: NSAIDs (salt/water retention), negative inotropes (e.g., CCBs), unrecognized congestion and inadequate diuretic use
HF-related disease states: Uncontrolled hypertension, myocardial ischemia or infarction, atrial or ventricular arrhythmias, pulmonary emboli
Other: Systemic infection, worsening renal/hepatic failure, hyperthyroidism, untreated sleep apnea, anemia or iron deficiency
8. DIAGNOSIS
Biomarkers
- BNP/NT-proBNP: Gold standard biomarkers; elevated in HF from volume/pressure overload; used for diagnosis, prognosis, and monitoring
- Cardiac troponins: Elevated in ADHF; associated with worse outcomes
Electrocardiogram
- No specific diagnostic pattern for HF
- LVH + left atrial enlargement → HFpEF from HTN, AS, HCM
- Q waves → ischemic cardiomyopathy
- Pseudo-infarct pattern (Q waves + reduced QRS voltage) → restrictive/infiltrative (amyloid)
- Conduction disease → cardiac sarcoid or Chagas cardiomyopathy
- AF present in up to 40% of chronic HF patients
- QRS width and LBBB guide CRT/pacing eligibility
Echocardiography (key noninvasive tool)
- LVEF ≥50% = systolic function normal
- Myocardial strain (speckle tracking) adds prognostic value
- Doppler estimates CO, PA pressures, valve areas, diastolic dysfunction
- TEE/CT: rule out LAA thrombus before cardioversion; assess valve pathology for TAVR/repair
Cardiac MRI
- Best for quantitative LV mass, volumes, function
- Defines specific etiology: ischemic CM, myocarditis, amyloidosis, hemochromatosis
- Late gadolinium enhancement (LGE) patterns guide diagnosis
Cardiopulmonary Exercise Testing (CPET)
- Used in evaluation for MCS or heart transplant
- Key parameters: peak VO2 and VE/VCO2 slope (independent predictors of survival)
Independent Predictors of Adverse Outcome (Table 264-1)
- Male sex, older age, diabetes mellitus, CKD, CAD, advanced NYHA class
- Presence of S3 or elevated JVP
- Decreased exercise capacity, cardiac cachexia
- Low LVEF, low sodium, elevated BNP/troponin, renal impairment
9. MANAGEMENT
9a. HFrEF (LVEF ≤40%) - The "Four Pillars"
Evidence-based, disease-modifying pharmacotherapy:
| Drug Class | Examples | Benefits |
|---|---|---|
| RAAS blockers | ACEi / ARB / ARNI (sacubitril-valsartan) | Reduce mortality and hospitalization |
| Beta-blockers | Carvedilol, metoprolol succinate, bisoprolol | Reduce mortality; anti-arrhythmic |
| MRA | Spironolactone, eplerenone | Reduce mortality and hospitalization |
| SGLT-2 inhibitors | Dapagliflozin, empagliflozin | Reduce CV mortality + HF hospitalizations |
9b. HFpEF/HFmrEF (LVEF ≥41%)
- Historically symptom-focused; management of comorbidities (obesity, DM, sleep apnea, HTN, AF, anemia, CKD)
- SGLT-2 inhibitors now have evidence to reduce CV mortality and HF hospitalizations in HFmrEF and HFpEF
- GLP-1 agonists and angiotensin-neprilysin inhibitors: emerging favorable results
- RAAS antagonists and MRA show variable benefits; principally in those with LVEF <60%
9c. Acute Decompensated HF (ADHF) Management
Three phenotypes guide therapy (Fig. 265-2):
- Hypertensive ADHF: High BP, pulmonary congestion → vasodilators (nitrates, nitroprusside)
- Normotensive ADHF: Congestion without hypotension → IV diuretics (furosemide)
- Low-output ADHF/Cardiogenic shock: Hypotension, hypoperfusion → inotropes, vasopressors, MCS
Vasopressive Drugs in ADHF (Table 265-1):
Inotropic therapy (for hypotension/shock):
- Dobutamine: 2-20 μg/kg/min; variable efficacy with beta-blockers
- Milrinone: 0.375-0.75 μg/kg/min; reduce dose in renal insufficiency
- Levosimendan: 0.1 μg/kg/min; retains efficacy in presence of beta-blockers
Vasodilators (for congestion with preserved BP):
- Nitroglycerin: 10-200 μg/min (often underdosed)
- Nitroprusside: 0.3-5 μg/kg/min; requires arterial line; caution thiocyanate toxicity in renal failure
- Nesiritide: 2 μg/kg bolus + 0.01 μg/kg/min infusion; hypotension risk
Poor prognostic markers in ADHF:
- BUN >43 mg/dL, SBP <115 mmHg, creatinine >2.75 mg/dL, elevated BNP/troponins
9d. Device Therapy
- ICD (Implantable Cardioverter-Defibrillator): Sudden cardiac death prevention in HFrEF
- CRT (Cardiac Resynchronization Therapy): For LBBB with wide QRS; improves symptoms and mortality
- His bundle / LBBP pacing: Emerging alternative to CRT
9e. Advanced/Stage D HF
- Cardiac transplantation: Gold standard for eligible patients
- LVAD (Mechanical Circulatory Support): Bridge to transplant or destination therapy
- Palliative care: Appropriate when salvage therapies are exhausted
9f. Surgical Therapy (selected indications)
- Coronary revascularization (for ischemic HF)
- Valvular repair/replacement (mitral, aortic)
- Transcatheter valve procedures (TAVR, MitraClip)
10. SUMMARY TABLE: HF EF-Based Management
| Feature | HFrEF (≤40%) | HFmrEF (41-49%) | HFpEF (≥50%) |
|---|---|---|---|
| Diuretics | Yes (symptom control) | Yes | Yes |
| ACEi/ARB/ARNI | Yes (mortality) | Consider | Limited benefit |
| Beta-blocker | Yes (mortality) | Consider | Not proven |
| MRA | Yes (mortality) | Consider | Limited |
| SGLT-2i | Yes (mortality + HF hosp) | Yes (emerging) | Yes (emerging) |
| ICD/CRT | Yes | Selected | No |
Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapters 264 & 265. Authors: Michael M. Givertz, Mandeep R. Mehra
This is a shared conversation. Sign in to Orris to start your own chat.