Compartment syndrome
Reading File
Finding Sources
Searching PubMed
"compartment syndrome" diagnosis management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive, high-quality information from multiple authoritative textbooks. I have enough to write a thorough answer.
Compartment Syndrome
Compartment syndrome is a condition where pressure within a closed fascial compartment rises to a level that compromises tissue perfusion, leading to progressive ischemia and potentially irreversible muscle and nerve damage. It is a surgical emergency.
Anatomy
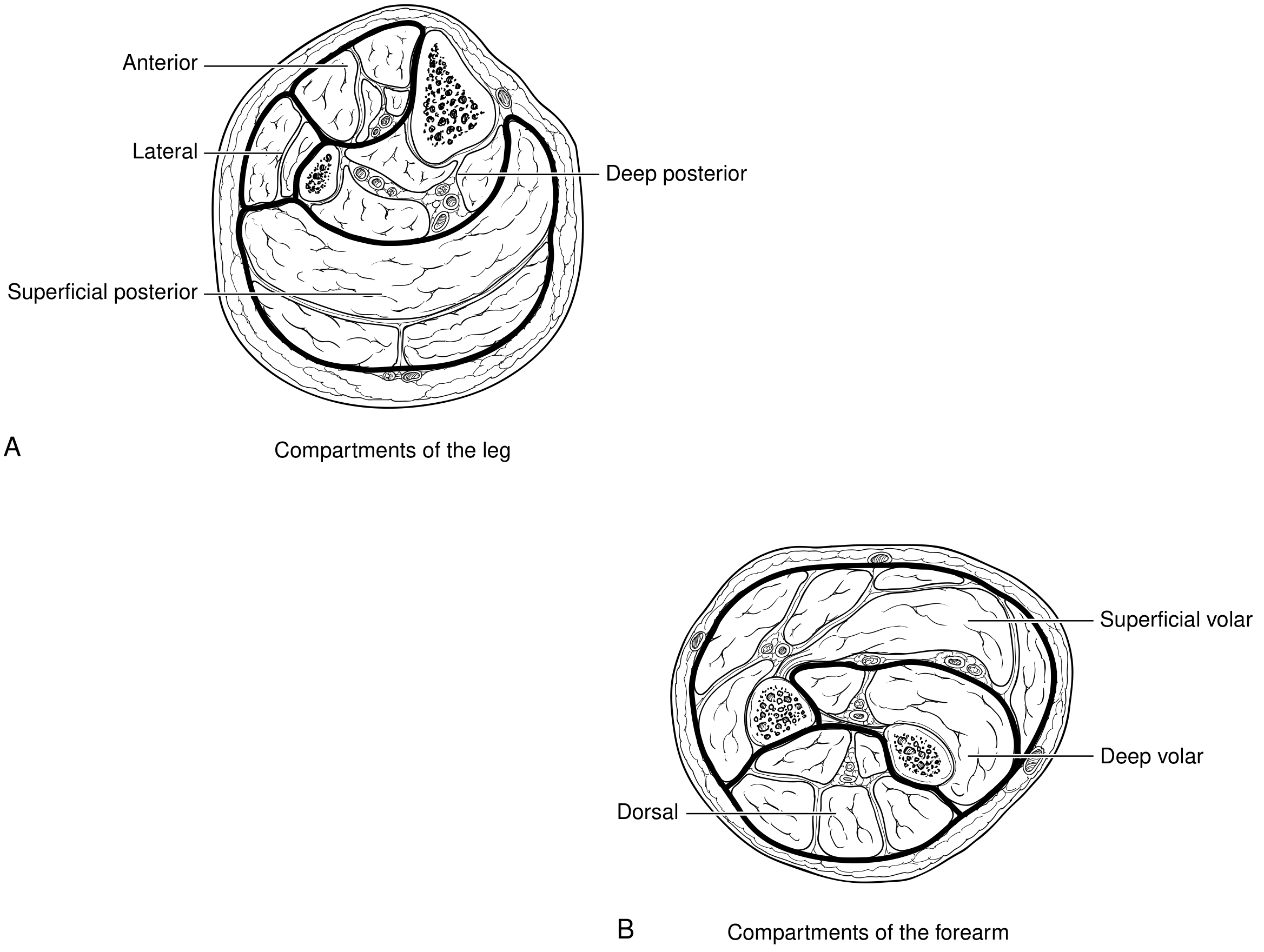
Muscles are enclosed within fascial compartments. The leg has four compartments (anterior, lateral, superficial posterior, and deep posterior); the forearm has three (superficial volar, deep volar, and dorsal). Because fascia is inelastic, any increase in compartment volume or decrease in compartment size raises pressure rapidly.
Types
| Type | Description |
|---|---|
| Acute | Surgical emergency; most common after fracture or crush injury |
| Chronic (exertional) | Seen in athletes; exercise-induced pain that resolves with rest; no emergency |
| Abdominal | Elevated intra-abdominal pressure >20 mmHg with new organ dysfunction |
Causes of Acute Compartment Syndrome
Most common: Fractures (70%), especially proximal/midshaft tibial fractures (~36% of lower leg cases).
Other causes include:
- Soft tissue contusions (23%)
- Crush injuries, gunshot wounds
- Vascular injury / reperfusion after ischemia (reperfusion injury releases oxygen free radicals, triggers lipid peroxidation and calcium influx, driving progressive edema)
- Circumferential third-degree burns
- Tight casts or dressings
- Extravasation of IV infusions
- Bleeding disorders / anticoagulation
- Prolonged exertion (rare)
High-risk demographics: Males under 55 years; patients on anticoagulation.
Bailey and Love's Short Practice of Surgery 28th Ed, p. 466; Campbell's Operative Orthopaedics 15th Ed, Box 53.2
Pathophysiology
- Tissue volume increases (hemorrhage, edema) or container shrinks (tight cast)
- Pressure in the closed compartment rises
- Venous outflow is impaired first, creating a positive-feedback loop of increasing edema
- Capillary perfusion pressure is exceeded - tissue ischemia begins
- Irreversible muscle necrosis occurs from cellular anoxia
- Nerve damage follows (non-myelinated type C sensory fibers are most sensitive to hypoxia)
- Systemically: rhabdomyolysis, myoglobinuria, acute tubular necrosis, renal failure
Rosen's Emergency Medicine 9e, Chapter 40
Clinical Features
Compartment syndrome is a clinical diagnosis.
The "6 Ps" (in order of appearance)
| Sign | Timing | Notes |
|---|---|---|
| Pain out of proportion | Early | Most sensitive sign |
| Pain on passive stretch | Early | Most important clinical sign |
| Pressure (tense compartment) | Early | Firm, woody feel on palpation |
| Paraesthesia / Paresthesia | Intermediate | Nerve ischemia |
| Paralysis | Late | Muscle ischemia advanced |
| Pallor + Pulselessness | Very late | Near-terminal finding; does NOT rule out CS if absent |
Critical point: Pulselessness is an extremely late sign. The presence of palpable pulses does NOT rule out compartment syndrome. Do not wait for it. - Bailey and Love, p. 466
Key warning: Do not dismiss escalating analgesic requirements as drug-seeking behavior - this should prompt urgent evaluation for compartment syndrome.
Rockwood and Green's Fractures in Adults 10th Ed 2025, Chapter 63; Bailey and Love, p. 466
Compartment Pressure Measurement
Used when clinical diagnosis is uncertain (e.g., sedated patient, altered consciousness, head injury).
Techniques: Slit catheter, wick catheter, handheld Stryker device
Thresholds for fasciotomy:
- Absolute pressure ≥ 30 mmHg (Mubarak/Hargens criterion)
- Delta pressure (ΔP) = Diastolic BP - Compartment pressure ≤ 30 mmHg (Bailey & Love)
- Some sources use ΔP < 10-20 mmHg as a more aggressive threshold
- High clinical suspicion warrants fasciotomy even with normal pressures
Important: Measure multiple sites and all compartments in the affected limb. Elevated CPK and myoglobinuria are late markers of tissue destruction - do not use them to establish or exclude the diagnosis.
Roberts and Hedges' Clinical Procedures in Emergency Medicine; Current Surgical Therapy 14e, p. 1155
Management
Immediate (Emergency)
- Remove or split all circumferential casts, dressings, and bandages down to skin
- Elevate the limb
- Seek senior/surgical input immediately
- Do NOT delay for imaging if clinical diagnosis is clear
Definitive: Fasciotomy
Fasciotomy should be performed without delay once diagnosis is made. There are no contraindications - though correction of coagulopathy is preferred when time allows. - Fischer's Mastery of Surgery 8e
Indications for fasciotomy:
- Compartment pressure ≥ 30 mmHg
- ΔP ≤ 30 mmHg (diastolic - compartment pressure)
- High clinical suspicion regardless of pressure
Lower leg: Four-compartment fasciotomy via double-incision technique (lateral and medial incisions). A single perifibular incision may be used if soft tissue is not extensively distorted, but double-incision is generally safer.
Forearm: Volar (superficial + deep) and dorsal compartment releases. If swelling extends to the hand, carpal tunnel release and hand fasciotomies may also be required.
Post-fasciotomy: Wounds are left open. Vacuum-assisted closure (VAC) is applied. Return to OR at 48-72 hours for debridement. Delayed primary closure or skin grafting once swelling resolves.
Campbell's Operative Orthopaedics 15th Ed 2026; Current Surgical Therapy 14e, p. 1155
Timing matters critically:
- Fasciotomy < 12 hours from onset: ~68% good results
- Fasciotomy > 12 hours from onset: ~8% good results
Campbell's Operative Orthopaedics 15th Ed 2026
Prophylactic Fasciotomy
Indicated when prolonged ischemia (>6 hours) preceded revascularization or when limb edema is observed after arterial repair. The more severe the prior ischemia, the more likely reperfusion compartment syndrome will develop. Liberal use of four-compartment calf (with or without thigh) fasciotomies following revascularization of a prolonged ischemic limb is advisable.
Current Surgical Therapy 14e, p. 1155; Bailey and Love, p. 461
Chronic Exertional Compartment Syndrome
- Typical in athletes; most common in the anterolateral leg compartment
- Aching/cramping starting within 10-30 min of exercise, resolving with rest
- No signs at rest - diagnosis requires history + intracompartmental pressure measurement before and after exercise in a specialized center
- Fascial defects may be found on MRI in up to 40% of patients
- Treatment: activity modification, or elective fasciotomy in refractory cases
Rheumatology 2-Volume Set (2022, Elsevier)
Complications of Untreated Compartment Syndrome
- Volkmann's ischemic contracture (forearm)
- Rhabdomyolysis - acute kidney injury / ATN
- Permanent sensorimotor deficits
- Limb loss / amputation
- Death (in severe cases with systemic involvement)
Key Pitfalls
- Compartment syndrome can occur in open fractures - do not assume an open wound decompresses all compartments
- High-energy and low-energy injuries have nearly equal incidence of compartment syndrome
- Pulselessness is not required for diagnosis - it is a very late sign
- Sedated or obtunded patients cannot report pain - maintain high suspicion and use pressure monitoring
- Elevated CPK/myoglobinuria confirm damage but are not diagnostic tools
This is a shared conversation. Sign in to Orris to start your own chat.