arrhythmias
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching Images
cardiac arrhythmia ECG patterns classification
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have extensive, rich content from Braunwald's Heart Disease and Harrison's. I have enough to write a comprehensive, well-structured overview. Let me compile it now.
Arrhythmias — Overview
1. Classification
Arrhythmias are broadly classified by origin and rate:
| Category | Rate | Origin |
|---|---|---|
| Bradyarrhythmias | < 60 bpm | SA node dysfunction, AV block |
| Supraventricular | Variable–rapid | Atria, AV node, accessory pathways |
| Ventricular | Usually rapid | His-Purkinje system, ventricular myocardium |
Bradyarrhythmias
- Sinus bradycardia
- Sinus arrest / SA exit block
- Sick sinus syndrome (SSS)
- AV block: 1st degree, 2nd degree (Mobitz I/II), 3rd degree (complete)
Supraventricular Arrhythmias (SVAs)
- Sinus tachycardia / sinus arrhythmia
- Premature atrial contractions (PACs)
- Focal atrial tachycardia (AT)
- Multifocal atrial tachycardia (MAT)
- Atrial flutter
- Atrial fibrillation (AF)
- AV nodal reentrant tachycardia (AVNRT)
- AV reentrant tachycardia (AVRT) — via accessory pathway (WPW)
- Junctional tachycardia
Ventricular Arrhythmias
- Premature ventricular contractions (PVCs)
- Non-sustained VT (NSVT) — < 30 sec
- Sustained monomorphic VT
- Polymorphic VT
- Torsades de Pointes (TdP)
- Ventricular flutter / fibrillation (VF)
2. Mechanisms
Three fundamental electrophysiologic mechanisms underlie virtually all arrhythmias (Braunwald's Heart Disease):
A. Abnormal Automaticity
Normal automaticity is confined to the sinus node. Enhanced automaticity occurs when subsidiary pacemakers (AV node, His-Purkinje cells) fire spontaneously at abnormally rapid rates, or when working myocardium acquires pacemaker activity. This underlies focal atrial tachycardia, accelerated idioventricular rhythms, and some VTs. Features include:
- Gradual onset ("warm-up") and offset ("cool-down")
- Not initiated or terminated by overdrive pacing
B. Triggered Activity
Caused by membrane potential oscillations called afterdepolarizations:
| Type | Timing | Mechanism | Clinical Example |
|---|---|---|---|
| Early afterdepolarizations (EADs) | During phases 2/3 of AP | ↑ inward Ca²⁺/Na⁺ current; prolonged QT | Torsades de Pointes |
| Delayed afterdepolarizations (DADs) | After full repolarization (phase 4) | ↑ intracellular Ca²⁺ overload → transient inward current | Digoxin toxicity, catecholaminergic VT (CPVT) |
C. Reentry
The most common mechanism. Requires:
- Two functionally or anatomically distinct pathways
- Unidirectional block in one pathway
- Slow conduction in the other (sufficient time for the blocked limb to recover)
- Retrograde excitation of the recovered pathway
Reentry underlies: AVNRT, AVRT (WPW), atrial flutter, post-infarction VT, most sustained monomorphic VTs.
3. Key Arrhythmias and ECG Patterns
Sinus Arrhythmia
- Phasic variation in sinus cycle length; physiologically normal
- Maximum–minimum cycle length > 120 msec or > 10% difference
- P wave morphology unchanged; PR interval constant
Sinus Bradycardia
- HR < 60 bpm; causes include high vagal tone (athletes, sleep, inferior MI), drugs (beta-blockers, digoxin, amiodarone, calcium antagonists, ivabradine)
- Sick sinus syndrome: combination of sinus bradycardia, arrest, exit block, often with bradycardia-tachycardia syndrome
- Usually benign; inferior MI sinus bradycardia carries better prognosis than sinus tachycardia
AV Block
| Degree | PR Interval | QRS | Mechanism |
|---|---|---|---|
| 1st degree | > 200 ms, constant | Normal | Slowed AV conduction |
| 2nd degree Mobitz I (Wenckebach) | Progressive lengthening → dropped QRS | Normal | AV nodal (usually proximal) |
| 2nd degree Mobitz II | Fixed PR → sudden dropped QRS | Often wide (BBB) | Infranodal (His/Purkinje) |
| 3rd degree (complete) | None — AV dissociation | Wide (ventricular escape) or narrow (junctional) | Complete AV dissociation |
- Block proximal to His bundle → QRS narrow, rate 40–60 bpm (more stable)
- Block distal to His → wide QRS, rate < 40 bpm (less stable, more dangerous)
Focal Atrial Tachycardia
- Rate 100–250 bpm; discrete P waves with isoelectric intervals between them
- Mechanisms: enhanced automaticity, triggered activity, or microreentry
- "Warm-up" at onset, "cool-down" at termination if automatic
- Adenosine blocks AV conduction but does NOT terminate the AT (unlike AVNRT/AVRT) — distinguishing feature
Atrial Fibrillation (AF)
- Irregularly irregular rhythm; absent discrete P waves → chaotic f waves (350–600/min)
- AV node filters impulses → ventricular rate typically 110–160 bpm (uncontrolled)
- Mechanism: multiple reentrant wavelets ± focal triggers (commonly pulmonary veins)
Atrial Flutter
- Macro-reentry circuit in right atrium around tricuspid annulus
- Atrial rate ~300/min; classic "sawtooth" flutter waves in II, III, aVF
- Typical 2:1 conduction → ventricular rate ~150 bpm
AVNRT
- Most common paroxysmal SVT; sudden-onset, regular, narrow-complex tachycardia ~150–250 bpm
- Reentry using slow and fast pathways within/near AV node
- P waves hidden within or just after QRS (retrograde); pseudo-R' in V1, pseudo-S in II/III/aVF
AVRT (WPW)
- Accessory pathway (bundle of Kent) bypasses AV node
- Orthodromic AVRT: narrow complex (anterograde via AV node, retrograde via AP)
- Antidromic AVRT: wide complex (anterograde via AP, retrograde via AV node)
- Sinus rhythm shows delta wave (slurred QRS upstroke), short PR
Ventricular Tachycardia (VT)
- ≥ 3 consecutive beats ≥ 100 bpm, wide QRS (> 120 ms)
- Monomorphic: uniform QRS morphology → usually scar-related reentry (post-MI, ARVC, cardiomyopathy)
- Polymorphic: changing QRS morphology → ischemia, channelopathies (LQTS, Brugada, CPVT)
- Torsades de Pointes: polymorphic VT with twisting QRS around isoelectric line, triggered by EADs on background of prolonged QT
VT vs. SVT with Aberrancy (Wide Complex Tachycardia)
The algorithm from Harrison's (shown below) is used for differentiation:
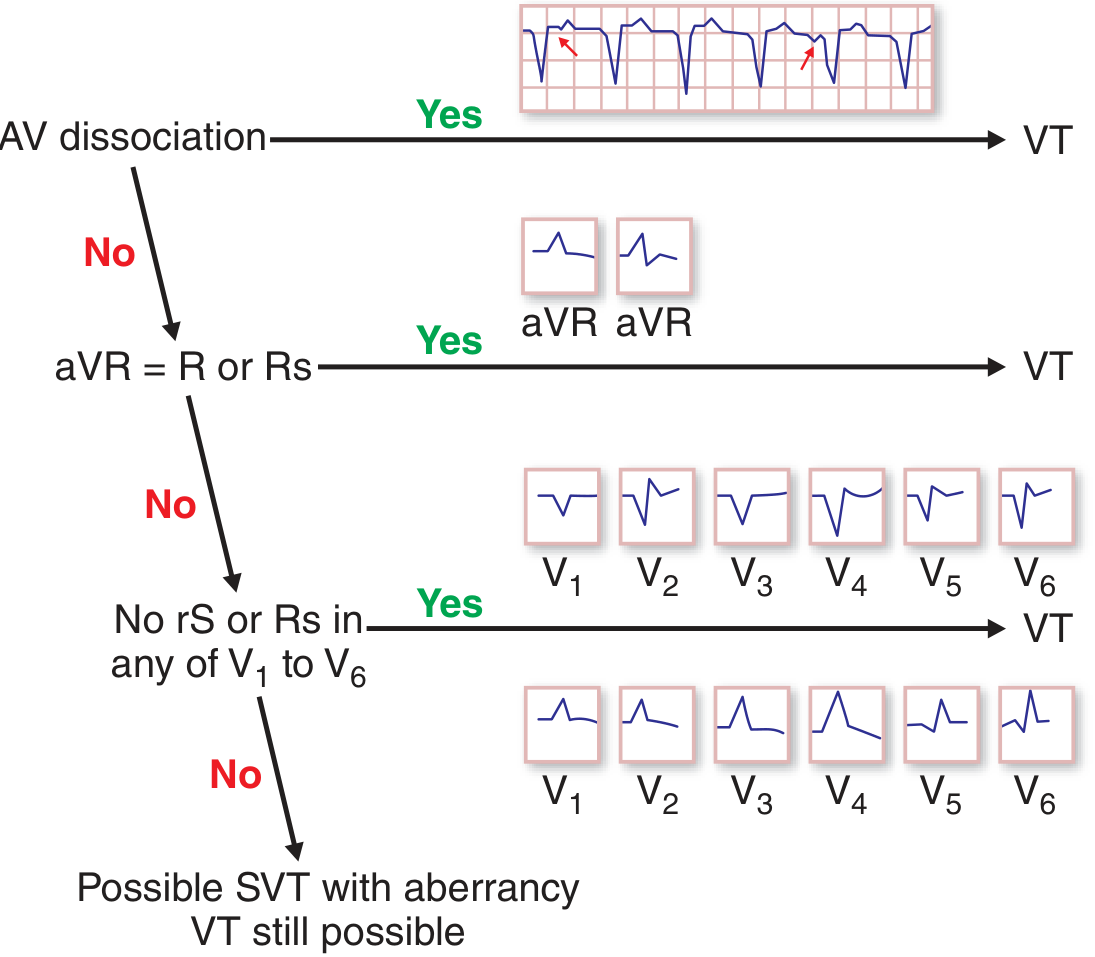
Key ECG features favoring VT:
- AV dissociation (P waves independent of QRS) — most specific criterion
- Positive R or Rs in aVR
- No rS or Rs complex in any of V1–V6 (concordance)
- QRS duration > 140 ms (RBBB morphology) or > 160 ms (LBBB morphology)
- Northwest axis (−90° to ±180°)
- Fusion beats or capture beats
Hemodynamic stability does not distinguish VT from SVT with aberrancy.
Ventricular Fibrillation (VF)
- Completely disorganized ventricular depolarization; no effective cardiac output
- Leads to cardiac arrest within seconds; requires immediate defibrillation
4. Arrhythmias by Underlying Disease (Causes)
| Setting | Typical Arrhythmia |
|---|---|
| Post-MI (scar) | Sustained monomorphic VT (reentry) |
| Acute ischemia | Polymorphic VT, VF |
| Dilated cardiomyopathy | NSVT, sustained VT, VF |
| ARVC | Monomorphic VT (LBBB morphology, RV origin) |
| Hypertrophic cardiomyopathy | Polymorphic VT, VF |
| LQTS | Torsades de Pointes (EAD-triggered) |
| Brugada syndrome | VF (nocturnal) |
| CPVT | Bidirectional or polymorphic VT with exercise/stress |
| Digoxin toxicity | DAD-triggered VT, AF with slow ventricular response |
| Sarcoidosis / Lamin A/C mutation | Monomorphic VT (fibrotic scar) |
5. Genetic Arrhythmia Syndromes (Channelopathies)
| Syndrome | Gene | ECG finding | Arrhythmia |
|---|---|---|---|
| LQTS type 1 | KCNQ1 (IKs↓) | Broad T wave | TdP with exercise |
| LQTS type 2 | KCNH2 (IKr↓) | Notched/bifid T | TdP with emotion/noise |
| LQTS type 3 | SCN5A (INa↑) | Late-peaked T | TdP at rest/sleep |
| Brugada | SCN5A (INa↓) | Coved ST↑ in V1–V3 | VF (nocturnal) |
| CPVT | RYR2 | Normal | Polymorphic/bidirectional VT |
| Short QT | KCNH2/KCNJ2 | Short QT < 300 ms | VF |
Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 12th ed.
Harrison's Principles of Internal Medicine, 22nd ed.
This is a shared conversation. Sign in to Orris to start your own chat.