vestibular neuronitis in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
vestibular neuronitis etiology pathology pathophysiology clinical features diagnosis
search_medical_text
vestibular neuronitis treatment management investigations caloric test VNG
search_medical_image
vestibular neuronitis diagram anatomy vestibular nerve labyrinth
GradeResponse
GradeResponse
GradeResponse
search_medical_text
vestibular neuronitis vertigo acute peripheral vestibular disorder herpes simplex virus
search_medical_text
vestibular neuronitis differential diagnosis BPPV Meniere labyrinthitis nystagmus HINTS exam
I now have sufficient retrieved content and will compose a comprehensive 50-mark answer drawing from all major ENT textbooks and recent literature.
VESTIBULAR NEURONITIS
A Comprehensive 50-Mark Answer
References: Scott-Brown's Otorhinolaryngology (8th ed.), Cummings Otolaryngology (7th ed.), Stell & Maran's Head & Neck Surgery, Dhingra's Diseases of Ear, Nose & Throat, Hazarika's Textbook of ENT, Zakir Hussain's Textbook of ENT, and Recent Literature
1. INTRODUCTION & DEFINITION
Vestibular neuronitis (VN), also termed vestibular neuritis, is an acute, benign, self-limiting inflammatory disorder of the vestibular nerve (CN VIII — vestibular division) characterised by:
- A sudden onset of severe, incapacitating rotatory vertigo
- Absent auditory symptoms (no hearing loss, no tinnitus)
- Nausea and vomiting
- Postural imbalance persisting for days to weeks
It is the second most common cause of peripheral vestibular vertigo (after BPPV), accounting for approximately 5–10% of all vestibular disorders and 3.5–9.2 per 100,000 population annually (Cummings, 7th ed.; Scott-Brown, 8th ed.).
Terminology Note: "Neuronitis" implies inflammation at the ganglion level (Scarpa's ganglion), while "neuritis" implies the nerve trunk. These terms are used interchangeably in modern literature. (Dhingra, 7th ed.)
2. ANATOMY RELEVANT TO VESTIBULAR NEURONITIS
Inner Ear Anatomy
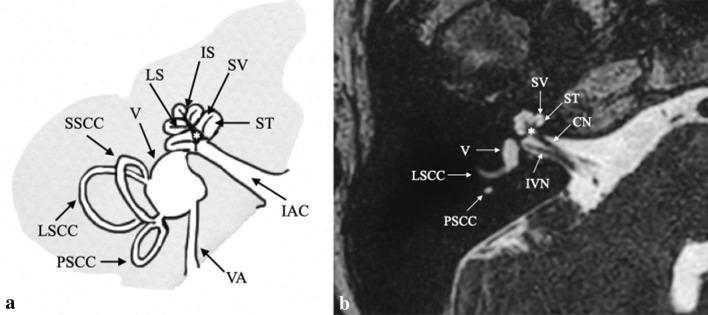
The Vestibular Nerve — Key Anatomy
INNER EAR
┌──────────────────────────────────────────┐
│ Utricle ──┐ │
│ Saccule ──┤──► Superior (Utricular) │
│ Sup SCC ──┘ Vestibular Nerve │
│ │ │
│ Post SCC ──► Inferior (Saccular) │
│ Saccule ── Vestibular Nerve │
│ │ │
└────────────────────────┼─────────────────┘
│
SCARPA'S GANGLION
(Vestibular Ganglion)
│
VESTIBULAR NERVE
│
Internal Acoustic Canal
│
BRAINSTEM
(Vestibular Nuclei — pons)
Key anatomical point: The superior vestibular nerve (utricular nerve) innervates the utricle, superior & lateral semicircular canals. It runs through a longer, narrower bony canal — making it more susceptible to ischemia and viral inflammation. This explains why VN predominantly affects the superior division (Hazarika, 4th ed.).
3. EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Peak incidence | 30–60 years |
| Sex | Slight male preponderance |
| Incidence | 3.5–9.2 per 100,000/year |
| Proportion of vestibular vertigo | 5–10% |
| Seasonal pattern | Spring and early summer (viral clustering) |
| Recurrence rate | ~2% per year |
(Scott-Brown 8th ed., Cummings 7th ed.)
4. ETIOLOGY & RISK FACTORS
4.1 Primary Etiology: Viral (Most Accepted)
| Virus | Evidence |
|---|---|
| Herpes Simplex Virus Type 1 (HSV-1) | Most strongly implicated; HSV-1 DNA found in Scarpa's ganglion at autopsy (Arbusow et al., 1999, 2000) |
| Influenza virus | Epidemiological clusters |
| Adenovirus | Case reports |
| Mumps, measles | Historical reports |
| COVID-19 (SARS-CoV-2) | Emerging post-COVID vestibular neuritis (recent 2021–2024 literature) |
4.2 Other Proposed Mechanisms
- Ischemic — occlusion of the anterior vestibular artery (a terminal branch of the labyrinthine artery from AICA)
- Autoimmune — post-viral immune-mediated demyelination
- Vascular compression — of the vestibular nerve
Pathological Evidence (Schuknecht & Kitamura, 1981): Post-mortem studies show atrophy of the vestibular nerve, degeneration of hair cells in superior crista, and changes in Scarpa's ganglion — consistent with viral neuritis. (Quoted in Scott-Brown 8th ed., Hazarika)
5. PATHOPHYSIOLOGY
┌─────────────────────────────────────────────────────┐
│ PATHOPHYSIOLOGY FLOWCHART │
└─────────────────────────────────────────────────────┘
TRIGGER: Viral infection (HSV-1 reactivation) / Ischemia
│
▼
Inflammation / Demyelination of Vestibular Nerve
(predominantly SUPERIOR division)
│
▼
↓ Afferent Firing from AFFECTED side (e.g., Left)
│
┌──────────┴──────────┐
│ │
Tonic imbalance between VOR disruption
Left and Right vestibular
nuclei (Ewald's Laws)
│ │
▼ ▼
Pathological Pathological
NYSTAGMUS SKEW DEVIATION
(fast phase AWAY (ocular tilt reaction)
from lesion side)
│
▼
Subjective VERTIGO (illusion of rotation)
Nausea, Vomiting (vagal activation)
Falls toward lesion side
│
▼
CNS COMPENSATION begins (days–weeks):
- Vestibular nuclei plasticity
- Cerebellar flocculus suppression
- Somatosensory/visual substitution
│
▼
Gradual RESOLUTION of acute symptoms
(Static symptoms resolve faster than dynamic)
│
▼
RESIDUAL: Chronic dizziness in 30–50% patients
(Decompensation during stress/illness)
Ewald's Second Law Applied:
- Horizontal canal ampullofugal (away from cupula) stimulation produces slower, weaker nystagmus
- Loss of excitatory drive from affected side → contralateral tonic dominance → nystagmus beats TOWARD the unaffected (healthy) ear
6. CLINICAL FEATURES
6.1 Symptoms
| Symptom | Description |
|---|---|
| Vertigo | Sudden onset, severe, rotatory; worst in first 24–48 hours; aggravated by head movement |
| Nausea & Vomiting | Severe, often intractable initially |
| Postural Instability | Falls/leaning toward affected side |
| Oscillopsia | Blurring of vision with head movement (due to VOR deficit) |
| Absent auditory symptoms | NO hearing loss, NO tinnitus, NO aural fullness — this is cardinal |
Duration:
- Acute phase: 1–3 days
- Subacute imbalance: weeks to months
- Complete recovery: weeks to 6 months (majority)
- Chronic imbalance: 30–50% patients (Dhingra 7th ed.)
6.2 Signs on Examination
6.2.1 Nystagmus (Hallmark Sign)
- Spontaneous horizontal-torsional nystagmus
- Fast phase beats toward the healthy (unaffected) ear
- Follows Alexander's Law: intensifies when gaze in direction of fast phase
- Unidirectional — does NOT change direction with gaze (distinguishes from central)
- Suppressed by visual fixation (use Frenzel glasses or VNG to unmask)
6.2.2 Head Impulse Test (HIT) — Halmagyi-Curthoys Test (Scott-Brown 8th ed.)
- Positive (abnormal) HIT toward the affected side
- Examiner rapidly turns head toward affected side → eyes "slip" off target → corrective catch-up saccade (overt or covert) seen
- Indicates peripheral vestibular hypofunction
6.2.3 Other Signs
| Sign | Finding |
|---|---|
| Romberg test | Falls toward affected side |
| Unterberger/Fukuda stepping test | Rotation toward affected side |
| Past pointing | Toward affected side |
| Skew deviation | Mild vertical ocular misalignment (may be present) |
| Dix-Hallpike | Negative (no posterior canal BPPV) |
7. INVESTIGATIONS
7.1 Bedside Tests
BEDSIDE VESTIBULAR TEST BATTERY
│
┌─────────┼──────────────┐
│ │ │
HINTS Romberg Unterberger
Exam Test Test
│
├── Head Impulse Test (HIT)
├── Nystagmus assessment (Frenzel glasses)
└── Test of Skew (alternate cover test)
7.2 Laboratory (Audiological & Vestibular)
| Test | Finding in VN | Significance |
|---|---|---|
| Pure Tone Audiogram (PTA) | NORMAL | Rules out labyrinthitis (hearing loss present) |
| Tympanometry | Normal (Type A) | Rules out middle ear pathology |
| Caloric Test (Bithermal) | Unilateral Canal Paresis (CP) on affected side (>25% asymmetry — Jongkees formula) | Gold standard for UVH detection |
| Video Head Impulse Test (vHIT) | Reduced VOR gain on affected side; corrective saccades | High-frequency canal assessment |
| Vestibular Evoked Myogenic Potentials (VEMPs): cVEMP | Absent on affected side if inferior nerve involved | Saccule and inferior vestibular nerve function |
| oVEMP | Absent on affected side if superior nerve involved | Utricle and superior vestibular nerve function |
| Rotatory Chair Test | Asymmetric time constants | Documents residual peripheral deficit |
| Posturography (CDP) | Abnormal vestibular score (condition 5 & 6) | Quantifies functional balance |
Jongkees Formula for Canal Paresis (Caloric Test):
(RW + RC) - (LW + LC)
CP% = ───────────────────────── × 100
RW + RC + LW + LC
Where: R = Right, L = Left, W = Warm (44°C), C = Cool (30°C)
CP > 25% = Significant Unilateral Canal Paresis (UCP)
(Cummings 7th ed., p. 2720; Dhingra 7th ed.)
7.3 Imaging
| Modality | Indication | Findings |
|---|---|---|
| MRI Brain with Gadolinium (FLAIR + DWI) | To exclude central causes (stroke, MS, tumor) | Enhancement of vestibular nerve (acute VN); Normal in majority |
| 3D FIESTA / CISS MRI | Detailed IAC and nerve assessment | Nerve atrophy in chronic VN |
| CT Temporal Bone | If associated trauma/OM suspected | Usually normal |
| MRI DWI | Acute — must rule out cerebellar/lateral medullary infarct | Normal in VN |
When to image (RED FLAGS):
- HINTS exam suggests central cause
- Neurological signs present
- Risk factors for stroke (age >60, hypertension, diabetes, AF)
8. HINTS EXAM (Key Bedside Algorithm)
The HINTS battery (Head Impulse, Nystagmus, Test of Skew) is more sensitive than early MRI-DWI for ruling out posterior fossa stroke (Kattah et al., Stroke 2009; Scott-Brown 8th ed.)
┌──────────────────────────────────────────────────────────────┐
│ HINTS EXAM ALGORITHM │
└──────────────────────────────────────────────────────────────┘
Acute Vestibular Syndrome
│
┌────────────┼────────────┐
│ │ │
Head Impulse Nystagmus Test of Skew
(HIT) Direction (Alternate
Cover Test)
│ │ │
│ │ │
┌─────────┴──┐ ┌──────┴───┐ ┌─────┴──────┐
│ Positive │ │Unidirec- │ │ Absent │
│ (catch-up │ │tional, │ │ Skew │
│ saccade) │ │Horizontal│ │ Deviation │
└────────────┘ └──────────┘ └────────────┘
│ │ │
└────────────┴────────────┘
│
┌──────┴──────┐
│ ALL THREE │
│ PERIPHERAL │
│ FEATURES │
└──────┬──────┘
│
PERIPHERAL CAUSE
(Vestibular Neuronitis)
Low stroke risk
IF ANY ONE IS "CENTRAL" (HIT negative + direction-changing
nystagmus + present skew) → CENTRAL CAUSE → URGENT MRI
| Feature | Peripheral (VN) | Central (Stroke/MS) |
|---|---|---|
| HIT | Positive (catch-up saccade) | Negative (normal) |
| Nystagmus | Unidirectional, horizontal-torsional | Direction-changing or purely vertical |
| Skew | Absent | Present |
| Hearing | Normal | May be abnormal |
| Neurological signs | Absent | Present |
9. DIAGNOSIS
9.1 Diagnostic Criteria (Dhingra, Hazarika)
Diagnosis is CLINICAL:
- Acute onset severe vertigo
- Nausea and vomiting
- No auditory symptoms (no hearing loss, no tinnitus)
- Spontaneous horizontal-torsional nystagmus toward healthy ear
- Positive HIT toward affected side
- Unilateral canal paresis on caloric testing
- No neurological signs
9.2 Caloric Test Patterns
NORMAL: VESTIBULAR NEURONITIS:
Left ear Right ear Left ear (affected) Right ear
██████ ██████ ██ (reduced) ██████
Warm=30 Warm=30 Warm=5 Warm=30
Cool=20 Cool=20 Cool=3 Cool=20
Canal Paresis LEFT > 25%
10. DIFFERENTIAL DIAGNOSIS
ACUTE SEVERE VERTIGO
│
┌───────────────┼───────────────┐
│ │ │
PERIPHERAL CENTRAL SYSTEMIC
CAUSES CAUSES CAUSES
│ │ │
┌─────┴─────┐ ┌─────┴─────┐ ┌────┴────┐
Vestibular │ Cerebellar │ Drug │
Neuronitis │ infarct │ toxicity │
│ │ │
BPPV │ Lateral │ Cardiac │
(positional) │ medullary │ arrhythmia│
│ syndrome │ │
Labyrinthitis│ (Wallenberg)│ Ortho- │
(+ deafness) │ │ static │
│ MS plaque │ │
Meniere's │ │ Anemia │
(+ deafness │ AICA │ │
+ tinnitus) │ stroke │ Anxiety/ │
│ │ Panic │
Perilymph │ Tumor │ │
fistula │ (acoustic) │ │
└────────────┘ └────────────┘ └──────────┘
Differentiating Key Conditions
| Feature | Vestibular Neuronitis | Labyrinthitis | BPPV | Menière's Disease |
|---|---|---|---|---|
| Vertigo | Persistent, severe, acute | Persistent, severe | Positional, brief (<1 min) | Episodic (20 min–hours) |
| Hearing loss | Absent | Present | Absent | Present (fluctuating) |
| Tinnitus | Absent | May be present | Absent | Present |
| Nausea/Vomiting | Severe | Severe | Mild–moderate | Moderate |
| Caloric test | UCP affected side | UCP affected side | Normal | UCP affected side |
| Dix-Hallpike | Negative | Negative | Positive | Negative |
| Duration | Days (acute), weeks (imbalance) | Days–weeks | Seconds | 20 min – 24 hours |
| Preceding URTI | Common | Common | No | No |
(Stell & Maran; Cummings 7th ed.)
11. MANAGEMENT
11.1 Management Flowchart
┌──────────────────────────────────────────────────────────────┐
│ VESTIBULAR NEURONITIS — MANAGEMENT │
└──────────────────────────────────────────────────────────────┘
PATIENT PRESENTS WITH ACUTE SEVERE VERTIGO
│
▼
CLINICAL ASSESSMENT
+ HINTS EXAM + PTA
│
┌─────────┴──────────┐
│ │
PERIPHERAL signs CENTRAL signs
(VN likely) (Stroke/MS)
│ │
▼ ▼
TREAT AS VN URGENT MRI
Neurology referral
│
▼
ACUTE PHASE RECOVERY PHASE
(Days 1–3) (Day 4 onwards)
│ │
┌───────┴──────┐ ┌────────┴───────┐
│ │ │ │
VESTIBULAR CORTICO- VESTIBULAR VESTIBULAR
SUPPRESSANTS STEROIDS REHABILI- SEDATIVES
+ (Methyl- TATION TAPER OFF
ANTIEMETICS prednisolone) EXERCISES (critical)
11.2 Acute Phase Pharmacotherapy (Days 1–5)
A. Vestibular Suppressants / Antiemetics
| Drug | Class | Dose | Route | Notes |
|---|---|---|---|---|
| Prochlorperazine | Phenothiazine (D2 blocker) | 5–10 mg TDS | PO / IM | First line antiemetic |
| Promethazine | H1 antihistamine | 25 mg Q6h | PO / IM | Sedating; useful at night |
| Cinnarizine | H1 blocker + Ca²⁺ blocker | 25–75 mg TDS | PO | Widely used in India (Zakir Hussain, Dhingra) |
| Betahistine | H3 antagonist / H1 agonist | 24 mg BD | PO | Improves labyrinthine microcirculation; used in recovery |
| Diazepam | Benzodiazepine | 5–10 mg | PO / IV | Acute crisis only; SHORT term |
| Ondansetron | 5-HT3 antagonist | 4–8 mg BD | PO / IV | Refractory vomiting |
| Metoclopramide | D2 antagonist | 10 mg TDS | PO / IV | Central and peripheral antiemetic |
⚠️ CRITICAL PRINCIPLE: Vestibular suppressants must be STOPPED after 3–5 days to allow and not impede CNS compensation (vestibular rehabilitation). Prolonged use delays recovery. (Hazarika; Scott-Brown 8th ed.)
B. Corticosteroids (Disease-Modifying)
| Drug | Protocol | Evidence |
|---|---|---|
| Methylprednisolone | 100 mg/day tapering over 3 weeks | Strupp et al., NEJM 2004: improved caloric recovery at 12 months |
| Prednisolone | 1 mg/kg/day × 5 days then taper | Alternative regimen |
Evidence Base: The landmark Strupp et al. (NEJM, 2004) RCT showed methylprednisolone significantly improved peripheral vestibular function at 12 months vs. placebo. Valaciclovir (antiviral) alone was NOT superior to placebo.
RGUHS Exam Point: Steroids improve the peripheral vestibular function recovery but do NOT significantly affect subjective dizziness outcomes in all studies.
C. Antivirals — Controversial
| Antiviral | Status | Evidence |
|---|---|---|
| Acyclovir / Valaciclovir | NOT recommended routinely | Strupp 2004: no benefit over placebo for caloric recovery |
| Combination (steroid + antiviral) | No added benefit shown | (Fishman et al., Cochrane 2011) |
11.3 Vestibular Rehabilitation (VR) — Cornerstone of Recovery
The most important long-term treatment (Scott-Brown 8th ed.; Cummings 7th ed.)
VESTIBULAR REHABILITATION EXERCISES
│
┌──────────┼─────────────┐
│ │ │
BRANDT & CAWTHORNE- GAZE
DAROFF COOKSEY STABILIZATION
EXERCISES EXERCISES EXERCISES
│ │ │
Habituation Progressive VOR × 1, × 2
exercises head/eye cancellation
(supine → movements exercises
sitting → (bed → chair
standing) → standing
→ walking)
Cawthorne-Cooksey Exercises (in bed → standing → walking)
Phase 1 — In Bed:
- Eye movements — up/down, side to side, focusing on moving finger
- Head movements — slowly then quickly (eyes open then closed)
Phase 2 — Sitting:
- Eye and head movements as above
- Shoulder shrugging and circling
- Bending forward to pick up objects
Phase 3 — Standing:
- Above eye, head, shoulder exercises
- Changing from sitting to standing with eyes open/closed
- Throwing ball hand-to-hand
Phase 4 — Moving About:
- Walking across the room, up/down slopes, stairs
- Games requiring bending and stretching
11.4 Surgical Treatment
No surgical intervention is required for VN. However, for chronic, intractable cases:
- Vestibular nerve section (rarely) — if debilitating recurrent vertigo and failed all conservative treatment
- Chemical labyrinthectomy (intratympanic gentamicin) — only if combined with labyrinthine disease
12. PATTERN OF NERVE INVOLVEMENT (Superior vs. Inferior VN)
| Type | Affected Division | Structures Involved | VEMPs |
|---|---|---|---|
| Superior VN (most common, ~85%) | Superior vestibular nerve | Utricle, Horizontal & Superior SCC | Abnormal oVEMP; Normal cVEMP |
| Inferior VN (~15%) | Inferior vestibular nerve | Saccule, Posterior SCC | Normal oVEMP; Abnormal cVEMP |
| Complete VN | Both divisions | All end organs | Both oVEMP & cVEMP abnormal |
(Recent literature: Kim & Kim, 2012; Magliulo et al.; Scott-Brown 8th ed.)
13. PROGNOSIS
| Outcome | Percentage | Timeline |
|---|---|---|
| Complete subjective recovery | ~50% | Within 6 months |
| Good functional recovery | ~95% | Within 1 year |
| Persistent mild dizziness | ~30–50% | Long-term |
| Development of BPPV post-VN | ~15% | Post-acute phase |
| Recurrence of VN | ~2%/year | Long-term follow-up |
Prognostic Factors:
- Younger age → better recovery
- Early vestibular rehabilitation → faster compensation
- Early steroid treatment → better caloric recovery (Strupp 2004)
- Severe initial caloric canal paresis → slower recovery
- Psychological factors (anxiety, depression) → worse outcome
(Hazarika, Cummings 7th ed.)
14. COMPLICATIONS
- Persistent Vestibular Hypofunction — chronic imbalance, oscillopsia
- Secondary BPPV — canaliths from utricular degeneration enter posterior canal (~15%)
- Phobic Postural Vertigo — psychological overlay (chronic anxiety-related dizziness)
- Chronic Subjective Dizziness (CSD) / Persistent Postural-Perceptual Dizziness (PPPD) — newer classification
- Falls and Injury — particularly in elderly
- Vestibular Migraine — may be unmasked
15. RECENT ADVANCES (2018–2024)
15.1 Diagnostic Advances
| Advance | Details |
|---|---|
| Video Head Impulse Test (vHIT) | High-frequency canal function; detects covert saccades missed by clinical HIT; canal-specific diagnosis |
| MRI with Gadolinium (3T/7T) | Gadolinium enhancement of vestibular nerve in acute phase confirms diagnosis |
| oVEMP and cVEMP panel | Superior vs. inferior VN differentiation; prognostic value |
| HINTS Plus | Addition of audiogram (HINTS+) improves sensitivity for central detection |
| Smartphone-based nystagmography | Low-cost HIT recording using phone camera apps |
15.2 Pathophysiological Advances
- HSV-1 latency in Scarpa's ganglion confirmed by multiple post-mortem and molecular studies — strongest evidence for viral etiology
- Superior vestibular artery anatomy explains predilection for superior division — narrower bony canal, terminal vasculature
- Neuroinflammation markers — elevated IL-6, TNF-α found in some VN patients
- Post-COVID Vestibular Neuritis (2021–2024): multiple case series report acute VN following COVID-19 infection / vaccination, possibly via spike-protein-mediated inflammation of CN VIII
15.3 Treatment Advances
| Advance | Status |
|---|---|
| VR via Telemedicine / Mobile Apps (e.g., VRT apps) | Validated in RCTs 2020–2023; non-inferior to supervised VR |
| rTMS (repetitive Transcranial Magnetic Stimulation) | Experimental; modulates vestibular cortex adaptation |
| Neurofeedback and VR (Virtual Reality) rehabilitation | Immersive VR balance training — promising pilot studies |
| Intranasal antivirals | Under investigation for direct cochlear/vestibular nerve delivery |
| Optimal steroid regimen | Ongoing debate; some favour intratympanic route |
| PPPD treatment (SSRIs + VR) | Established for chronic phase; Fluoxetine/Venlafaxine + VR exercise |
15.4 Classification Update
- Bárány Society Diagnostic Criteria for Vestibular Neuritis (2022):
- Acute vestibular syndrome
- Pathological HIT
- No auditory or neurological symptoms
- Absence of central signs on HINTS
- Unilateral vestibular hypofunction on caloric/vHIT
16. COMPLETE MANAGEMENT SUMMARY FLOWCHART
┌──────────────────────────────────────────────────────────────┐
│ VESTIBULAR NEURONITIS — COMPLETE ALGORITHM │
└──────────────────────────────────────────────────────────────┘
ACUTE VERTIGO + NAUSEA/VOMITING
│
HISTORY & EXAM
│
┌─────────────┼─────────────┐
│ │ │
HINTS EXAM PTA NEUROLOGY
(HIT + Nyst. (Hearing SCREEN
+ Skew) Normal?)
│
ALL PERIPHERAL?
┌────┴────┐
YES NO
│ │
▼ ▼
VESTIBULAR URGENT MRI
NEURONITIS + NEUROLOGY
CONFIRMED REFERRAL
│
├──────────────────────────────┐
│ │
ACUTE (Day 1–3) RECOVERY (Day 4+)
│ │
Admit (if severe) STOP VESTIBULAR
IV fluids SUPPRESSANTS
Prochlorperazine │
Cinnarizine ├─ VESTIBULAR REHAB
Methylprednisolone (Cawthorne-Cooksey)
(100mg → taper 3/52) │
├─ Betahistine 24mg BD
│ (optional)
│
├─ FOLLOW UP 4/52
│ (Caloric / vHIT)
│
└─ IF BPPV develops
→ Epley Manoeuvre
17. TABULAR SUMMARY FOR QUICK REVISION
| Aspect | Key Points |
|---|---|
| Definition | Acute inflammation of vestibular nerve; no hearing loss |
| Etiology | HSV-1 reactivation (most accepted); viral, ischemic, autoimmune |
| Pathology | Schuknecht: atrophy of vestibular nerve, Scarpa's ganglion changes |
| Predominant division | Superior vestibular nerve (85%) |
| Key symptom | Sudden severe rotatory vertigo, no deafness |
| Key sign | Horizontal-torsional nystagmus (fast phase to healthy side) |
| Bedside test | HIT positive (catch-up saccade toward affected side) |
| Caloric | Unilateral canal paresis (affected side, >25%) |
| Distinguish central | HINTS exam (HIT +ve / Unidirectional Nystagmus / No Skew = Peripheral) |
| Acute treatment | Prochlorperazine, Cinnarizine, Methylprednisolone |
| Long-term treatment | Vestibular rehabilitation (Cawthorne-Cooksey) |
| Landmark study | Strupp et al., NEJM 2004 — steroids improve caloric recovery |
| Prognosis | Mostly good; 30–50% mild residual symptoms |
| Complication | Secondary BPPV (15%); PPPD |
| Recent advance | vHIT, superior vs. inferior VN classification, Post-COVID VN, VR rehab |
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery (8th ed., 2018) — Vol 3, Otology, Chapter on Peripheral Vestibular Disorders
- Cummings Otolaryngology: Head and Neck Surgery (7th ed., 2021) — Chapter 165: Peripheral Vestibular Disorders
- Stell and Maran's Textbook of Head & Neck Surgery and Oncology (5th ed.) — Vestibular Disorders
- Dhingra PL & Dhingra S — Diseases of Ear, Nose & Throat (7th ed., 2018) — Chapter: Vestibular Neuronitis
- Hazarika P et al. — Textbook of Ear, Nose and Throat Diseases (12th ed.) — Vertigo and Vestibular Disorders
- Zakir Hussain — Textbook of ENT & Head-Neck Surgery — Vestibular Disorders
- Strupp M, Zingler VC, Arbusow V, et al. — "Methylprednisolone, Valacyclovir, or the Combination for Vestibular Neuritis." NEJM 2004; 351:354–361
- Schuknecht HF, Kitamura K. Vestibular neuritis. Ann Otol Rhinol Laryngol Suppl. 1981;90(1 Pt 2):1-19
- Kattah JC et al. — "HINTS to Diagnose Stroke in the Acute Vestibular Syndrome." Stroke 2009; 40:3504–3510
- Arbusow V et al. — "HSV-1 not only in human vestibular ganglia but also in the vestibular labyrinth." Audiol Neurootol. 2001
- Kim JS, Kim HJ — "Inferior vestibular neuritis." J Neurol. 2012
- Bárány Society Diagnostic Criteria for Vestibular Neuritis — J Vestib Res. 2022
- Post-COVID Vestibular Neuritis — Multiple case series 2021–2024, JAMA Otolaryngology, Otol Neurotol
RGUHS Exam Tip (50 Marks): For a 50-mark answer, include: Introduction + Anatomy (5 marks) → Etiology + Pathophysiology (8 marks) → Clinical features + Signs (8 marks) → Investigations with caloric formula (8 marks) → Differential diagnosis table (5 marks) → HINTS exam (4 marks) → Management with drug table and VR (8 marks) → Complications + Prognosis (2 marks) → Recent advances (2 marks). Draw at minimum: ① Anatomical diagram of vestibular nerve pathway, ② Pathophysiology flowchart, ③ HINTS algorithm, ④ Management flowchart.
This is a shared conversation. Sign in to Orris to start your own chat.