i am having an exam on bone cartilage histology explain it to me
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the content I need. Let me compile a comprehensive exam-ready guide.
Bone & Cartilage Histology — Exam Guide
Source: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina & Ross)
PART 1 — CARTILAGE
Overview
Cartilage is an avascular connective tissue composed of:
- Chondrocytes — the only cell type
- Extracellular matrix (ECM) — makes up >95% of cartilage volume
The ECM contains type II collagen fibrils (tension-resisting) + heavily hydrated proteoglycan aggregates (compression-bearing). This combination gives cartilage its characteristic resilience and pliability. Because it is avascular, nutrients diffuse from surrounding perichondrium through the matrix to reach the chondrocytes.
The 3 Types of Cartilage
| Feature | Hyaline | Elastic | Fibrocartilage |
|---|---|---|---|
| Dominant ECM | Type II collagen + proteoglycans | Type II collagen + elastic fibers/lamellae | Type I collagen (abundant) + minimal matrix |
| Perichondrium | Yes (except articular + growth plate) | Yes | No |
| Calcifies? | Yes (aging, endochondral ossification) | No | No |
| Locations | Articular surfaces, costal cartilages, tracheal rings, larynx, fetal skeleton, epiphyseal plate | Auricle of ear, epiglottis, Eustachian tube, vocal folds | IVD (annulus fibrosus), pubic symphysis, menisci, TMJ disc, sternal-clavicular joint |
| Function | Cushioning, smooth joint surface, structural support | Flexibility/elasticity | Resists compression and shearing |
| Stain for elastic | — | Orcein (elastic fibers stain brown) | — |
Hyaline Cartilage — Close-Up
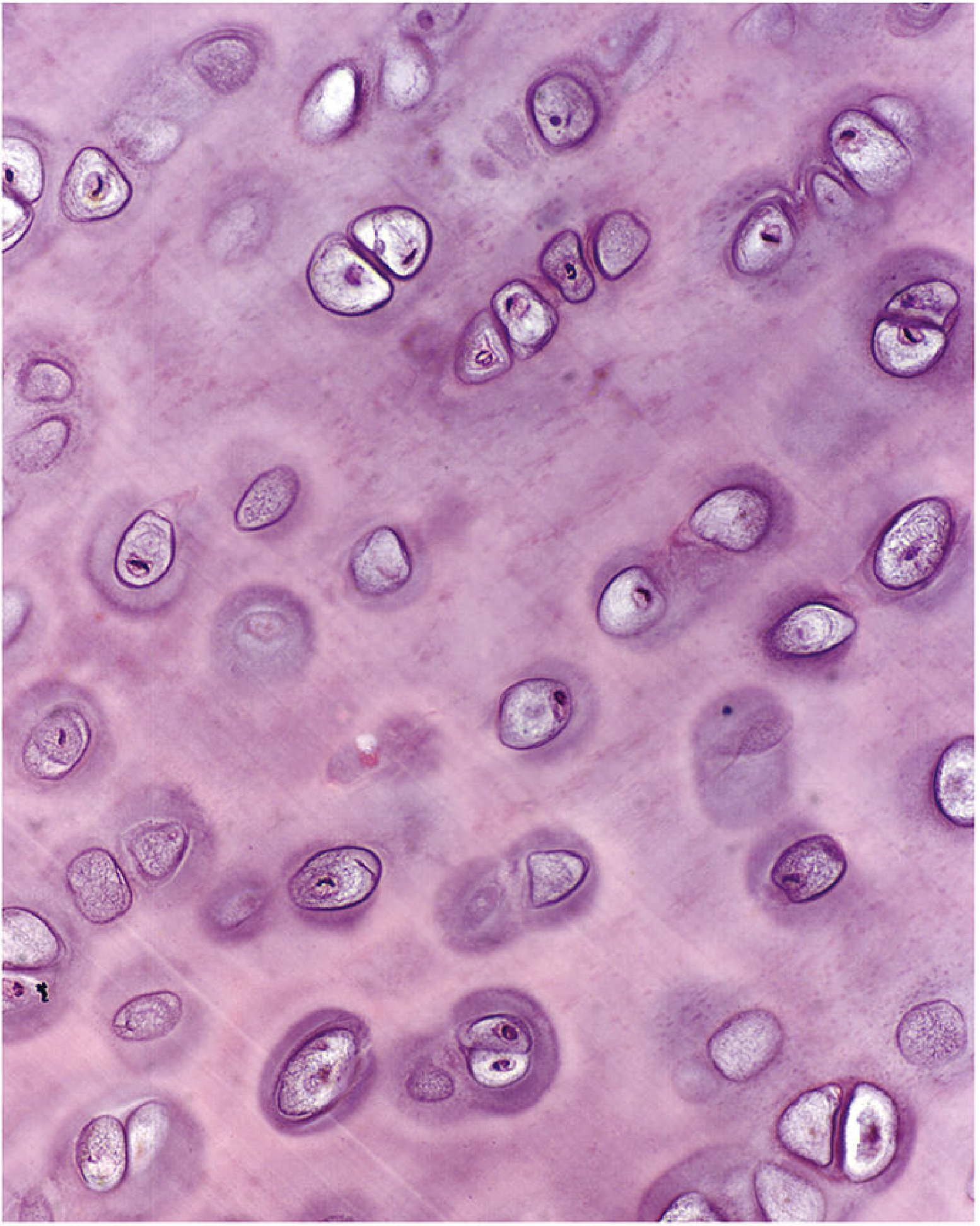
H&E ×450: Chondrocytes in lacunae dispersed within the extensive, lightly basophilic matrix. Pairs of chondrocytes = isogenous groups (daughter cells from mitotic division still sharing a lacuna).
Key cellular terms:
- Chondroblasts — active cells on the surface/perichondrium; secrete matrix
- Chondrocytes — mature cells within lacunae; maintain matrix
- Isogenous groups — clusters of 2–8 chondrocytes derived from one progenitor; a marker of interstitial growth
Matrix zones (from cell outward):
- Capsular (pericellular) matrix — immediately surrounds each chondrocyte; highest concentration of sulfated proteoglycans + type VI collagen; intensely basophilic/metachromatic
- Territorial matrix — surrounds the isogenous group; less intensely stained
- Interterritorial matrix — between groups; least stained; bulk of the matrix
Staining properties:
- Matrix stains basophilic with H&E (sulfated proteoglycans attract hematoxylin)
- Matrix stains metachromatic with toluidine blue (sulfated GAGs)
Elastic Cartilage
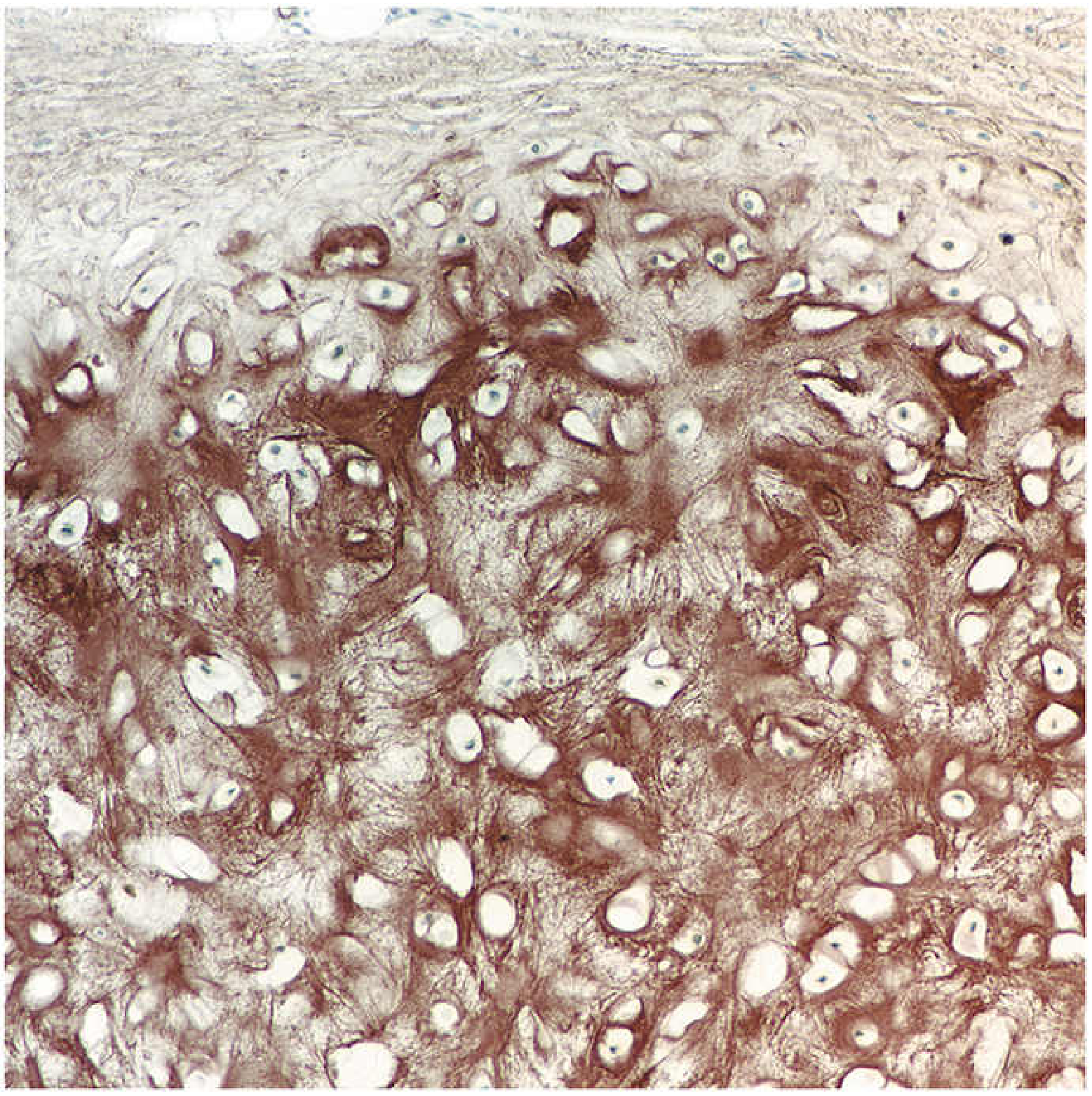
Orcein stain ×180: Dense network of brown elastic fibers among chondrocytes. Perichondrium visible at top.
Looks like hyaline cartilage on H&E but has abundant elastic fibers visible only with orcein or Weigert stains. Does not calcify with aging — clinically important distinction.
Fibrocartilage
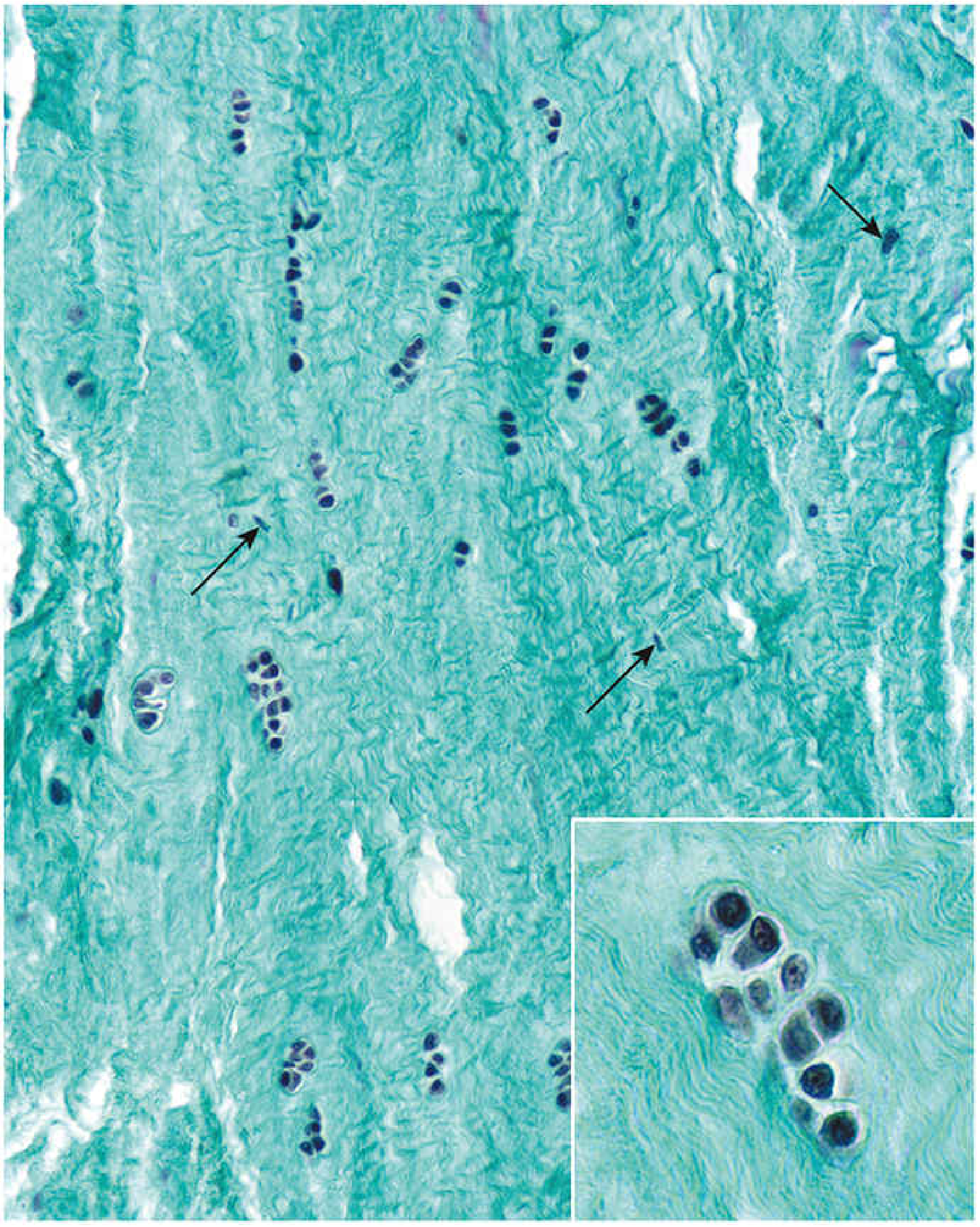
Gomori trichrome ×60: Dense green type I collagen bundles. Chondrocytes (round nuclei) arranged in rows and isogenous groups among fibroblasts (elongated, flattened nuclei). Inset shows an isogenous group at high magnification.
Key exam point: Fibrocartilage has no perichondrium, contains fibroblasts alongside chondrocytes, and its ECM is dominated by type I collagen (unlike other cartilage types).
Cartilage Growth
- Appositional growth — new chondrocytes arise from the inner chondrogenic layer of the perichondrium and add to the surface → increases width
- Interstitial growth — chondrocytes within the matrix divide mitotically → expands cartilage from within → seen as isogenous groups; occurs mainly during fetal/early life
Cartilage Repair
Hyaline cartilage has very limited repair capacity — avascular, chondrocytes cannot easily migrate. Damage typically heals as fibrocartilage scar.
PART 2 — BONE
General Classification
| Type | Description |
|---|---|
| Compact (cortical) | Dense outer shell; consists primarily of osteons (Haversian systems) |
| Spongy (cancellous) | Internal lattice of trabeculae; spaces filled with marrow |
| Woven (immature) | Developing bone; collagen fibers randomly oriented; temporary |
| Lamellar (mature) | Organized concentric lamellae; collagen fibers in alternating parallel arrays |
Bone Cells (Must Know All 4)
| Cell | Origin | Function | Key Feature |
|---|---|---|---|
| Osteoprogenitor | Mesenchymal stem cells (bone marrow) | Precursor; divides to replenish osteoblasts | Activated by CBFA1/RUNX2 transcription factor |
| Osteoblast | Osteoprogenitor cells | Secretes osteoid (unmineralized matrix); mineralization triggered by matrix vesicles | Cuboidal cells lining bone surface; abundant rER + Golgi |
| Osteocyte | Trapped osteoblasts | Maintain bone matrix; mechanosensing | Enclosed in lacunae; communicate via canaliculi (cell processes); network = canalicular system |
| Osteoclast | Hematopoietic progenitors (monocyte lineage) | Resorb bone | Large multinucleated cells; sit in Howship's lacunae (resorption pits); ruffled border faces bone |
RANK–RANKL pathway: Osteoblasts express RANKL → binds RANK on osteoclast precursors → osteoclast differentiation. PTH acts on osteoblasts (not osteoclasts directly) to upregulate RANKL. OPG (osteoprotegerin) from osteoblasts blocks RANKL → inhibits osteoclastogenesis.
Bone ECM (Osteoid)
- Organic (35%): ~90% type I collagen; non-collagenous proteins (osteocalcin, osteopontin, bone sialoprotein)
- Inorganic (65%): Hydroxyapatite — Ca₁₀(PO₄)₆(OH)₂ — deposited along collagen fibrils
The Osteon (Haversian System)
The structural unit of compact bone:
Central Haversian canal (blood vessels + nerves)
↑ surrounded by
Concentric lamellae (mineralized bone matrix in rings)
↑ between lamellae
Lacunae (osteocytes) → connected by → Canaliculi
↑ outer boundary
Cement line (marks boundary of one osteon)
- Volkmann (perforating) canals — run perpendicular to the long axis; connect Haversian canals to each other and to the periosteum/endosteum
- Interstitial lamellae — remnants of old, remodeled osteons between current osteons
- Circumferential lamellae — outer and inner rings of lamellar bone just beneath periosteum/endosteum
Ground section ×80: Circular osteons with central Haversian canals (dark = air or India ink). Interstitial lamellae fill spaces between osteons. Circumferential lamellae visible at periphery.
Bone Formation — Two Methods
1. Intramembranous Ossification
- No cartilage precursor — bone forms directly in mesenchyme
- Bones formed: Flat bones of skull, mandible, clavicle
- Sequence: mesenchymal condensation → osteoprogenitors → osteoblasts secrete osteoid → mineralization → woven bone → remodeled to lamellar bone
2. Endochondral Ossification
- Uses a hyaline cartilage model as scaffold
- Most bones in the body form this way

Fetal digit H&E ×210: Epiphyses (E) = cartilage. Hypertrophic chondrocytes (HC) in center. Calcified cartilage matrix (CCM) darker staining. Periosteal bony collar (BC) forming around shaft.
Stages:
- Cartilage model forms (hyaline)
- Chondrocytes at center hypertrophy → matrix calcifies
- Periosteal bony collar forms around diaphysis (via intramembranous ossification of periosteum)
- Blood vessels invade → primary ossification center in diaphysis
- Secondary ossification centers form in epiphyses later (most postnatal)
- Epiphyseal growth plate (physis) persists between primary and secondary centers until skeletal maturity
Epiphyseal Growth Plate — Zones (Proximal → Distal)
| Zone | What's Happening | Key H&E Feature |
|---|---|---|
| Reserve (resting) zone | Small chondrocytes, storing lipid/glycogen | Cells scattered, matrix pale |
| Proliferative zone | Rapid mitosis → columns (stacks) of flat chondrocytes | Columns ("coins stacked") = interstitial growth |
| Hypertrophic zone | Cells enlarge; matrix calcification begins | Large clear cytoplasm |
| Calcified cartilage zone | Chondrocytes die; matrix mineralized | Dark-staining matrix |
| Resorption (ossification) zone | Osteoclasts resorb cartilage; osteoblasts lay down bone | Bone trabeculae on calcified cartilage spicules |
Mnemonic: "Really Pretty Healthy Children" → Reserve, Proliferative, Hypertrophic, Calcified
Periosteum & Endosteum
| Periosteum | Endosteum | |
|---|---|---|
| Location | Outer surface of bone | Inner surface (marrow cavity, trabeculae, canals) |
| Layers | Outer fibrous + inner osteogenic (cambium) layer | Single layer of osteoprogenitors + osteoblasts |
| Function | Appositional growth, fracture repair | Remodeling, fracture repair |
Bone Remodeling & Calcium Regulation
- BMU (bone remodeling unit): Coupled osteoclasts + osteoblasts working together
- PTH: ↑ osteoclast activity (via RANKL on osteoblasts) → bone resorption → ↑ blood Ca²⁺
- Calcitonin: Inhibits osteoclasts → ↓ bone resorption → ↓ blood Ca²⁺
- Vitamin D (1,25-OH₂D₃ / calcitriol): ↑ Ca²⁺ absorption from gut + ↑ renal reabsorption
Fracture Repair (Secondary / Indirect)
- Hematoma formation
- Periosteal cells activated → form soft callus (fibrocartilage)
- Soft callus replaced by hard (bony) callus via endochondral ossification
- Callus remodeled to lamellar bone
Quick High-Yield Summary Table
| Feature | Cartilage | Bone |
|---|---|---|
| Vascularity | Avascular | Vascular (Haversian + Volkmann canals) |
| Main collagen | Type II (hyaline/elastic), Type I (fibrocartilage) | Type I |
| Cell in matrix | Chondrocyte (in lacuna) | Osteocyte (in lacuna + canaliculi) |
| Nutrition | Diffusion through matrix | Canalicular system + blood vessels |
| Mineralization | Hyaline only (aging/ossification) | Always — hydroxyapatite |
| Repair capacity | Very limited → fibrocartilage scar | Good — callus formation |
| Growth | Interstitial + appositional | Appositional only (adult) |
Source: Histology: A Text and Atlas with Correlated Cell and Molecular Biology, 9th ed. (Pawlina & Ross)
explain me bone and cartilage histology for a mbbs first year student
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Excellent - I have all the key diagrams and histology images. Now let me compile the complete, student-friendly explanation.
Bone & Cartilage Histology — MBBS First Year Guide
Source: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Ross & Pawlina, 9th ed.)
PART 1 — CARTILAGE
What is cartilage?
Think of cartilage as a firm but slightly rubbery connective tissue — like the tip of your nose or your ear. It has two basic ingredients:
- Chondrocytes — the only cells in cartilage, sitting inside little spaces called lacunae (singular: lacuna = "little lake")
- Extracellular matrix (ECM) — makes up over 95% of the tissue; contains type II collagen (for tension) + proteoglycans/GAGs (for compression and water-holding)
The single most important fact about cartilage: it is avascular (no blood vessels inside it). Nutrients diffuse through the matrix from blood vessels in the surrounding perichondrium. This is why cartilage heals so poorly after injury.
The 3 Types of Cartilage — The Big Picture
| Hyaline | Elastic | Fibrocartilage | |
|---|---|---|---|
| Matrix | Type II collagen + proteoglycans | Type II collagen + elastic fibers | Mostly type I collagen |
| Perichondrium? | Yes (except articular cartilage & growth plate) | Yes | No |
| Calcifies? | Yes (with age, and during ossification) | No | No |
| Appearance on H&E | Glassy, homogeneous, pale/basophilic | Like hyaline but elastic fibers need special stain | Fibrous-looking, dense collagen bundles |
| Special stain needed? | None | Orcein or resorcin-fuchsin (elastic fibers stain brown) | None (collagen visible on H&E) |
| Where found | Articular surfaces, costal cartilages, tracheal rings, larynx, fetal skeleton, epiphyseal plate | Auricle of ear (pinna), epiglottis, Eustachian tube, vocal folds | Intervertebral discs, pubic symphysis, menisci of knee, TMJ disc |
| Function | Cushioning, smooth joint surface, template for bone formation | Flexibility and elasticity | Resists both compression AND shearing forces |
1. Hyaline Cartilage (Most Important)
H&E ×450: The pale pink background is the ECM. Each dark oval = a chondrocyte nucleus sitting inside a lacuna. Groups of 2-4 cells in one lacuna = isogenous groups (daughter cells from recent division still sharing space).
Key points for exams:
- Named "hyaline" from Greek hyalos = glassy, because the matrix looks glassy/translucent in life
- Matrix stains basophilic (blue-purple) with H&E because sulfated proteoglycans attract hematoxylin
- Matrix stains metachromatic with toluidine blue (another common exam point)
Three matrix zones around each cell (from inside out):
- Capsular/pericellular matrix — immediately around the chondrocyte; darkest staining; richest in sulfated proteoglycans and type VI collagen
- Territorial matrix — surrounds the isogenous group; less intensely stained
- Interterritorial matrix — between groups; least stained; bulk of the matrix
Now see the perichondrium and matrix zones together:
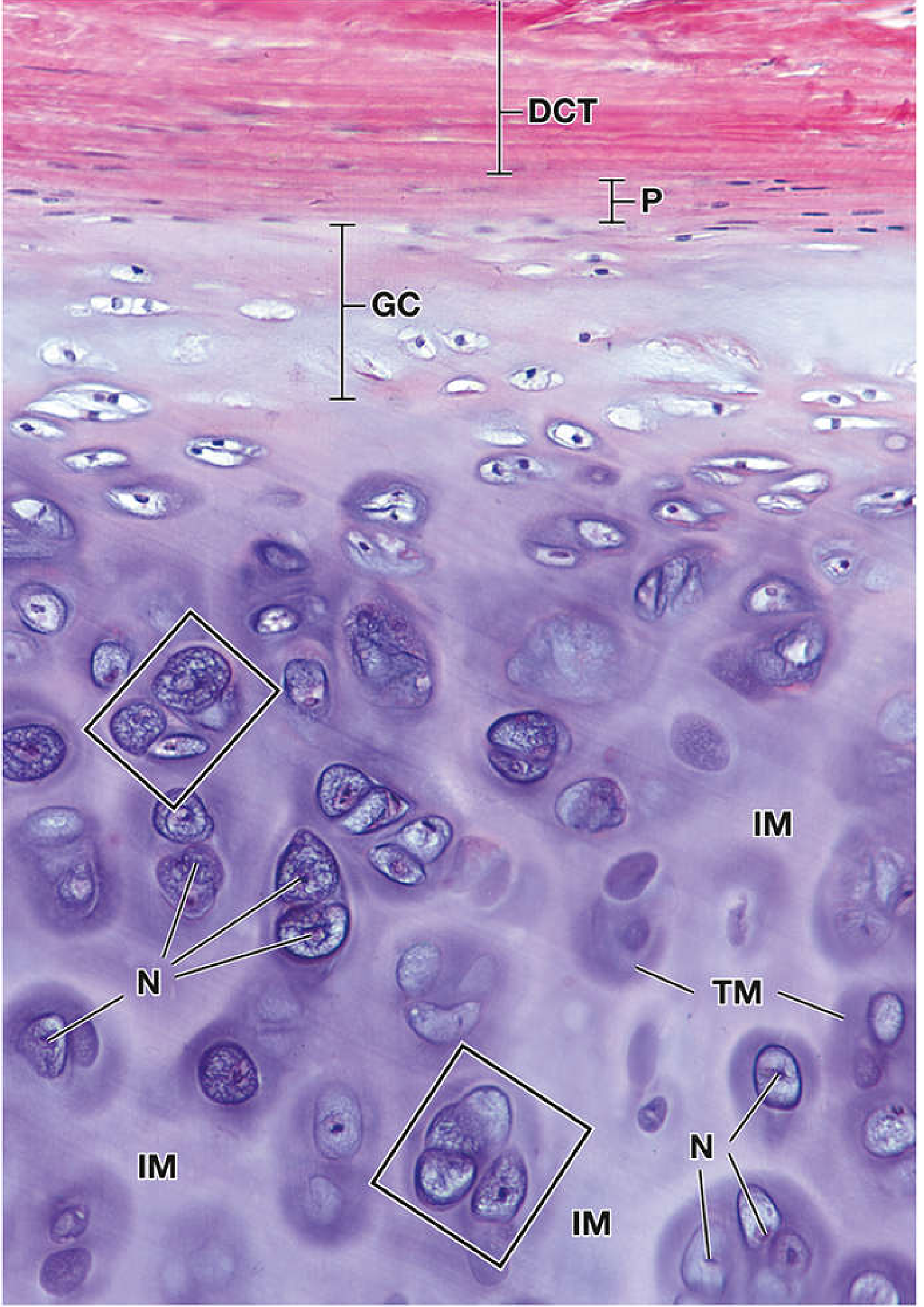
Top = dense connective tissue (DCT) → perichondrium (P) → growing cartilage layer (GC) with chondroblasts → mature chondrocytes with dark territorial matrix (TM) around them. Rectangles = isogenous groups = evidence of interstitial growth.
The perichondrium has two layers:
- Outer fibrous layer — collagen fibers, fibroblasts; mechanical protection
- Inner chondrogenic layer — contains chondroblasts (immature cells); responsible for appositional growth
2. Elastic Cartilage
Orcein stain ×180: The dense brown network = elastic fibers. Chondrocytes are visible as small blue nuclei in lacunae. Perichondrium is the pale layer at the very top.
Exam tip: On H&E alone, elastic cartilage looks identical to hyaline. You need the orcein stain to see the elastic fibers. Remember: elastic cartilage is the only type that does not calcify with aging.
3. Fibrocartilage
Gomori trichrome ×60: Dense green bundles = type I collagen. Chondrocytes (round nuclei) arranged in rows. Arrows = fibroblasts (elongated nuclei). Inset: isogenous group in a lacuna.
Three things that make fibrocartilage unique:
- No perichondrium
- Contains both chondrocytes and fibroblasts
- Collagen is type I (not type II like other cartilage)
Cartilage Growth — Two Ways
| Method | How it works | Where it happens |
|---|---|---|
| Appositional growth | Chondroblasts from the inner perichondrium add new cells + matrix to the surface | At the periphery; increases width |
| Interstitial growth | Chondrocytes already inside the matrix divide → isogenous groups push apart + lay down new matrix | From within; increases volume; mainly fetal/early life |
Why cartilage can't repair well
Because it is avascular and chondrocytes are trapped inside lacunae, they cannot migrate to a wound site. Damage typically heals with fibrocartilage scar tissue instead of true hyaline cartilage — this is why joint cartilage damage (like in osteoarthritis) is so problematic clinically.
PART 2 — BONE
What makes bone different from cartilage?
Bone is also a connective tissue, but it differs from cartilage in these critical ways:
| Feature | Cartilage | Bone |
|---|---|---|
| Vascularity | Avascular | Richly vascular |
| Matrix hardness | Firm but pliable | Rigid (mineralized) |
| Main collagen | Type II | Type I |
| Cells communicate via | Diffusion | Canalicular system |
| Repair | Very limited | Good |
The rigidity of bone comes from hydroxyapatite crystals [Ca₁₀(PO₄)₆(OH)₂] deposited along type I collagen fibrils. About 65% of bone weight is mineral; 35% is organic (mostly type I collagen).
Types of Bone Tissue
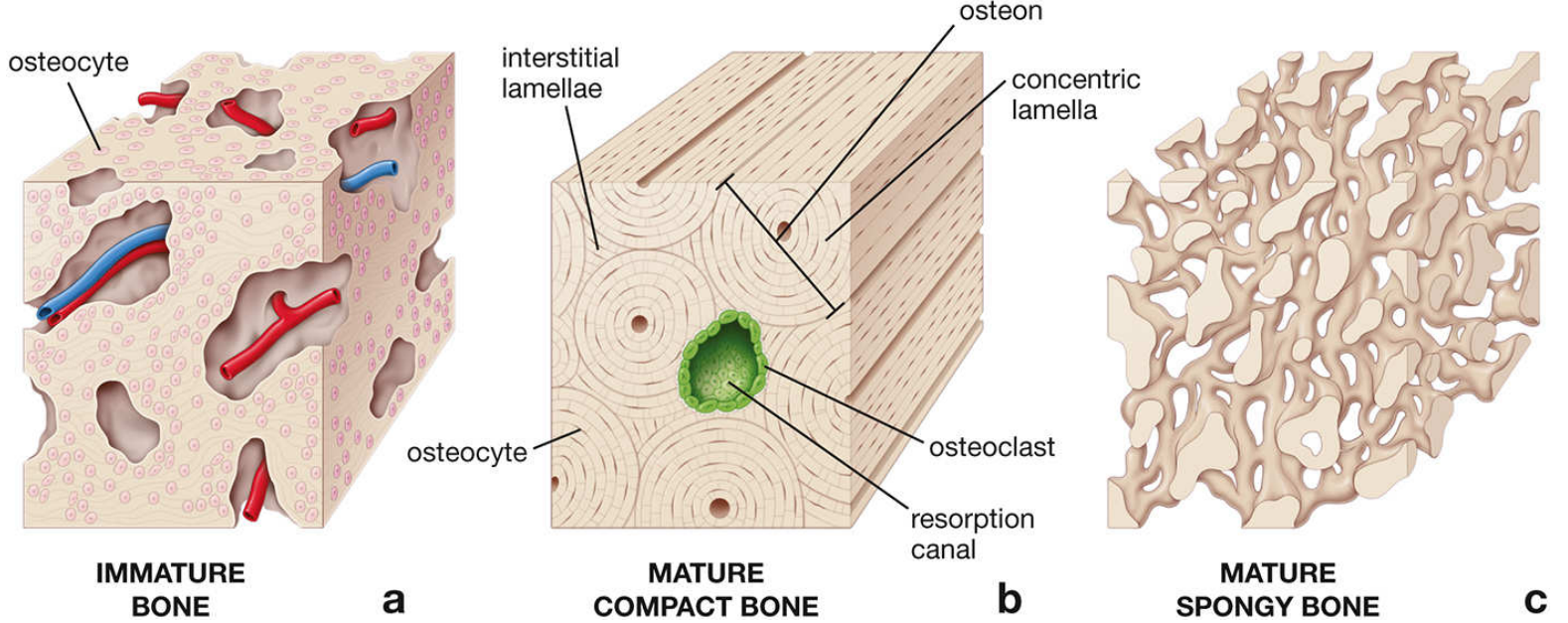
Two structural types:
- Compact (cortical) bone — solid, dense outer shell; organized into osteons
- Spongy (cancellous) bone — internal lattice of trabeculae; spaces filled with marrow
Two developmental types:
- Woven (immature) bone — collagen fibers randomly arranged, more cells per area, stains more with hematoxylin; seen in embryo and fracture healing (temporary)
- Lamellar (mature) bone — collagen fibers in organized parallel layers (lamellae); stains more with eosin; this is what adult bone looks like
The 4 Bone Cells (Know all of them!)
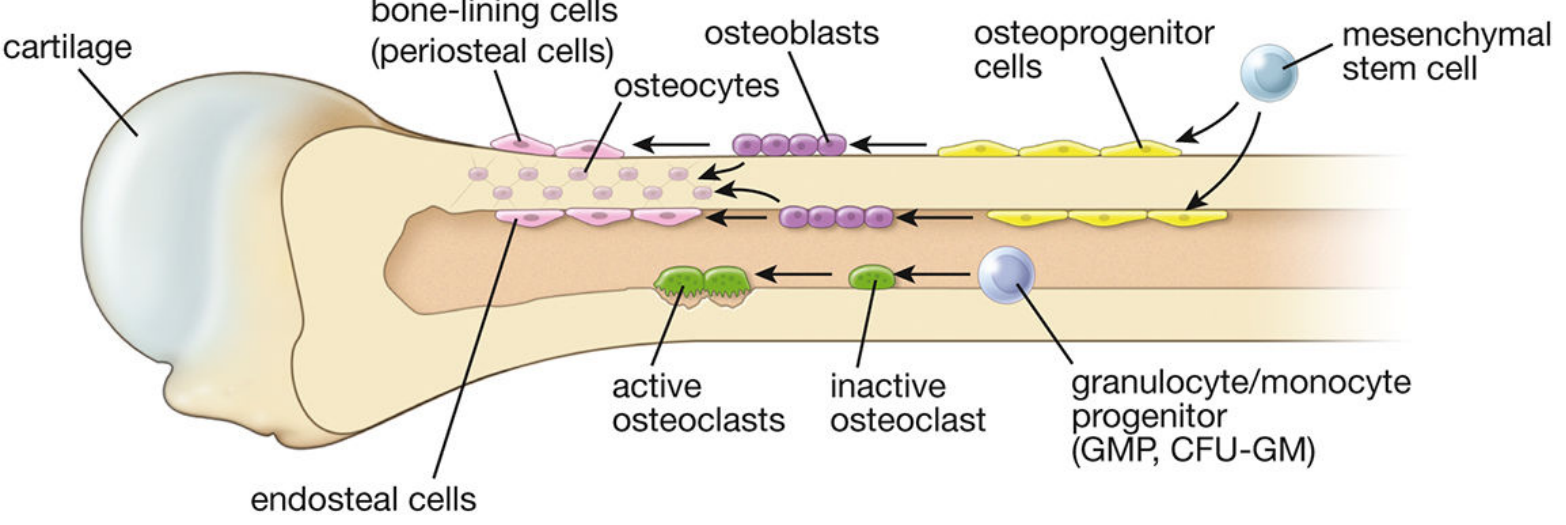
1. Osteoprogenitor cells
- Origin: mesenchymal stem cells in bone marrow
- Appearance: flat/squamous cells with pale elongated nucleus, little cytoplasm
- Location: inner periosteum (cambium layer) and endosteum
- Activated by transcription factor RUNX2/CBFA1 → differentiate into osteoblasts
2. Osteoblasts (bone-forming cells)
- Cuboidal cells lining bone surfaces
- Full of rough ER + large Golgi → actively synthesize protein
- Secrete osteoid (unmineralized bone matrix = type I collagen + glycoproteins)
- Mineralization triggered by matrix vesicles they release
- Once surrounded by matrix, they become osteocytes
3. Osteocytes (mature bone cells — most abundant)
- Trapped former osteoblasts sitting in lacunae within mineralized matrix
- Send long thin processes through channels called canaliculi
- These processes touch each other and touch osteoblasts → forms the canalicular network
- Function: maintain bone matrix, sense mechanical stress
4. Osteoclasts (bone-resorbing cells)
- Origin: hematopoietic progenitors (monocyte/macrophage lineage — completely different from the others!)
- Appearance: very large, multinucleated (6-50 nuclei), acidophilic cytoplasm
- Have a ruffled border (finger-like projections facing the bone surface) — this is where acid and enzymes are secreted to dissolve bone
- Sit in Howship's lacunae (shallow resorption pits they carve out)
- Controlled by RANK-RANKL pathway: osteoblasts express RANKL → binds RANK on osteoclast precursors → activates osteoclasts
The Osteon (Haversian System) — The Structural Unit of Compact Bone
This is the most tested structure in bone histology. Think of it like a hollow log:
Central Haversian canal (blood vessels + nerves + loose CT)
↑ surrounded by
Concentric lamellae (rings of mineralized bone matrix)
↑ between lamellae
Lacunae (containing osteocytes) ←→ connected by → Canaliculi
↑ outer boundary
Cement line (basophilic line separating one osteon from another)
Other canal types:
- Volkmann (perforating) canals — run at RIGHT ANGLES to the Haversian canals; connect Haversian canals to each other and to the periosteum/endosteum; do NOT have concentric lamellae around them (key distinction from Haversian canals)
Other lamellar patterns in compact bone:
- Circumferential lamellae — rings running all the way around the bone, just inside the periosteum (outer) and endosteum (inner)
- Interstitial lamellae — irregular fragments between osteons; remnants of old osteons that got partially resorbed during remodeling
Periosteum and Endosteum
| Periosteum | Endosteum | |
|---|---|---|
| Location | Covers outer surface of bone | Lines marrow cavity, trabeculae, Haversian + Volkmann canals |
| Layers | Outer fibrous + inner osteogenic (cambium) layer | Single layer of osteoprogenitors + osteoblasts |
| Function | Appositional growth; fracture repair; attachment of muscles/tendons (Sharpey's fibres anchor into it) | Remodeling; fracture repair |
Bone Formation — Two Methods
Method 1: Intramembranous Ossification (simpler)
- Bone forms directly in mesenchyme — no cartilage template
- Bones formed: flat bones of skull, mandible, clavicle
- Steps: mesenchymal condensation → mesenchymal cells → osteoblasts → secrete osteoid → mineralize → woven bone → remodel to lamellar bone
Method 2: Endochondral Ossification (forms most of the skeleton)
- Bone forms on top of a hyaline cartilage model
- All long bones, short bones, vertebrae, ribs form this way
- Steps in brief:
- Hyaline cartilage model forms (shape of future bone)
- Cartilage in the center (diaphysis) hypertrophies and calcifies
- Periosteal bony collar forms around the diaphysis shaft
- Blood vessels invade → primary ossification center forms in diaphysis
- Secondary ossification centers form later in the epiphyses
- Epiphyseal growth plate (physis) remains between primary and secondary centers → source of bone elongation in children
The Epiphyseal Growth Plate — 5 Zones (Proximal to Distal)
This is a classic exam question. Learn the zones in order:
| Zone | What's happening | H&E appearance |
|---|---|---|
| 1. Reserve (resting) | Small inactive chondrocytes, storing nutrients | Scattered cells, pale matrix |
| 2. Proliferative | Rapid mitosis → cells form columns like a stack of coins | Flat cells in vertical columns |
| 3. Hypertrophic | Cells enlarge dramatically; matrix begins to calcify | Very large, clear cytoplasm |
| 4. Calcified cartilage | Chondrocytes die; matrix fully mineralized | Darkly stained matrix, dead/absent cells |
| 5. Resorption (ossification) | Osteoclasts remove calcified cartilage; osteoblasts lay down new bone | Bone trabeculae on cartilage spicules |
Memory trick: "Really Pretty Healthy Children" → Reserve, Proliferative, Hypertrophic, Calcified (the 5th zone = resorption is implied after calcification)
The growth plate closes at skeletal maturity (late teens) → becomes the epiphyseal line → bone can no longer elongate.
Calcium Regulation in Bone
Bone is the major calcium reservoir of the body (99% of body calcium is in bone).
| Hormone | Source | Effect on bone | Net effect on blood Ca²⁺ |
|---|---|---|---|
| PTH (parathyroid hormone) | Parathyroid glands | Activates osteoclasts (via RANKL pathway) → bone resorption ↑ | ↑ blood Ca²⁺ |
| Calcitonin | Thyroid gland (C cells) | Inhibits osteoclasts | ↓ blood Ca²⁺ |
| Vitamin D (calcitriol) | Kidney (activated) | ↑ Ca²⁺ absorption from gut + ↑ renal reabsorption | ↑ blood Ca²⁺ |
Fracture Repair (Secondary/Indirect Healing)
- Hematoma — blood clot fills fracture gap
- Soft callus — periosteal cells proliferate → form fibrocartilage bridging the gap
- Hard (bony) callus — fibrocartilage replaced by woven bone via endochondral ossification
- Remodeling — woven bone remodeled to lamellar bone; excess callus removed by osteoclasts
Quick Comparison — The Most Important Exam Points
| Feature | Hyaline Cartilage | Elastic Cartilage | Fibrocartilage | Bone |
|---|---|---|---|---|
| Main collagen | Type II | Type II | Type I | Type I |
| Vascularity | None | None | None | Rich |
| Cells | Chondrocytes | Chondrocytes | Chondrocytes + fibroblasts | 4 types |
| Perichondrium | Yes | Yes | No | Periosteum |
| Special stain | None | Orcein | None | Ground section / H&E |
| Calcifies? | Yes (aging) | No | No | Always |
| Repair | Very poor | Very poor | Poor | Good |
Source: Histology: A Text and Atlas with Correlated Cell and Molecular Biology, 9th ed. (Ross & Pawlina)
This is a shared conversation. Sign in to Orris to start your own chat.