Gonnococcal urethritis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gonococcal urethritis" AND treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material to write a full answer. Let me compile everything.
Gonococcal Urethritis
Etiology & Epidemiology
Gonococcal urethritis (GU) is caused by Neisseria gonorrhoeae, a gram-negative diplococcus. It is a sexually transmitted infection and one of the most commonly reported STIs globally. In the United States alone, over 468,000 cases of gonorrhea were reported in 2016, with case counts rising year-on-year.
-
Incubation period: 2-6 days (range 2-14 days)
-
N. gonorrhoeae adheres to columnar and cuboidal mucosal epithelium of the urethra and endocervical canal
-
Up to 10% of infected men are asymptomatic; in women, ~50% carry the infection silently
-
Campbell-Walsh-Wein Urology, p. 1647
-
Goldman-Cecil Medicine, p. 3092
Clinical Features
In Men
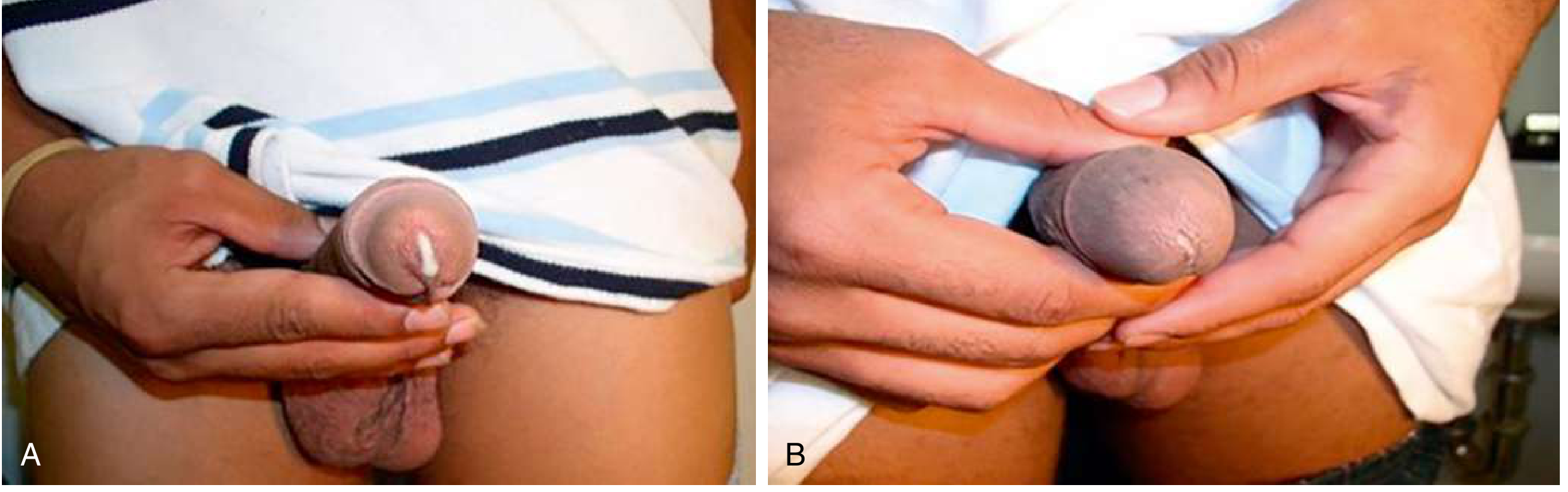
The hallmark presentation is acute anterior urethritis characterized by:
- Profuse, purulent urethral discharge - typically white, yellow, or green
- Dysuria (burning on urination)
- Meatal irritation, meatal erythema, penile lymphedema
- In ~25% of men, symptoms may be milder and discharge only apparent after urethral "milking/stripping"
- Without treatment, symptoms spontaneously resolve in ~6 months, but the patient remains infectious
Compare to non-gonococcal urethritis (NGU), where discharge is thin, clear, or gray (see clinical photo below).
In Women
- Primary site = endocervical canal
- Symptoms: increased vaginal discharge, dysuria, intermenstrual bleeding, menorrhagia
- Urethritis may cause dysuria
- Often asymptomatic until complications develop (PID, tubal scarring, infertility, ectopic pregnancy)
Local Complications (by spread/ascent)
| Site | Complication |
|---|---|
| Urethra | Urethral stricture (post-GU) |
| Epididymis | Epididymitis (unilateral testicular pain + swelling + urethritis) |
| Prostate | Prostatitis |
| Seminal vesicles | Vesiculitis |
| Cowper/Tyson glands | Periurethral abscess |
| Female reproductive tract | Salpingitis, PID, infertility, ectopic pregnancy |
| Neonate (birth canal) | Ophthalmia neonatorum |
Disseminated Gonococcal Infection (DGI)
-
Fever, arthritis, tenosynovitis, acral cutaneous pustules
-
Rarely: endocarditis, meningitis
-
Dermatology 2-Volume Set 5e, p. 1758
Diagnosis
Clinical Criteria for Urethritis (any one of):
- Mucopurulent/purulent urethral discharge on exam
- Gram stain of urethral secretion: ≥2 WBCs per oil-immersion field
- Positive leukocyte esterase on first-void urine
-
10 WBCs/hpf from first-void urine
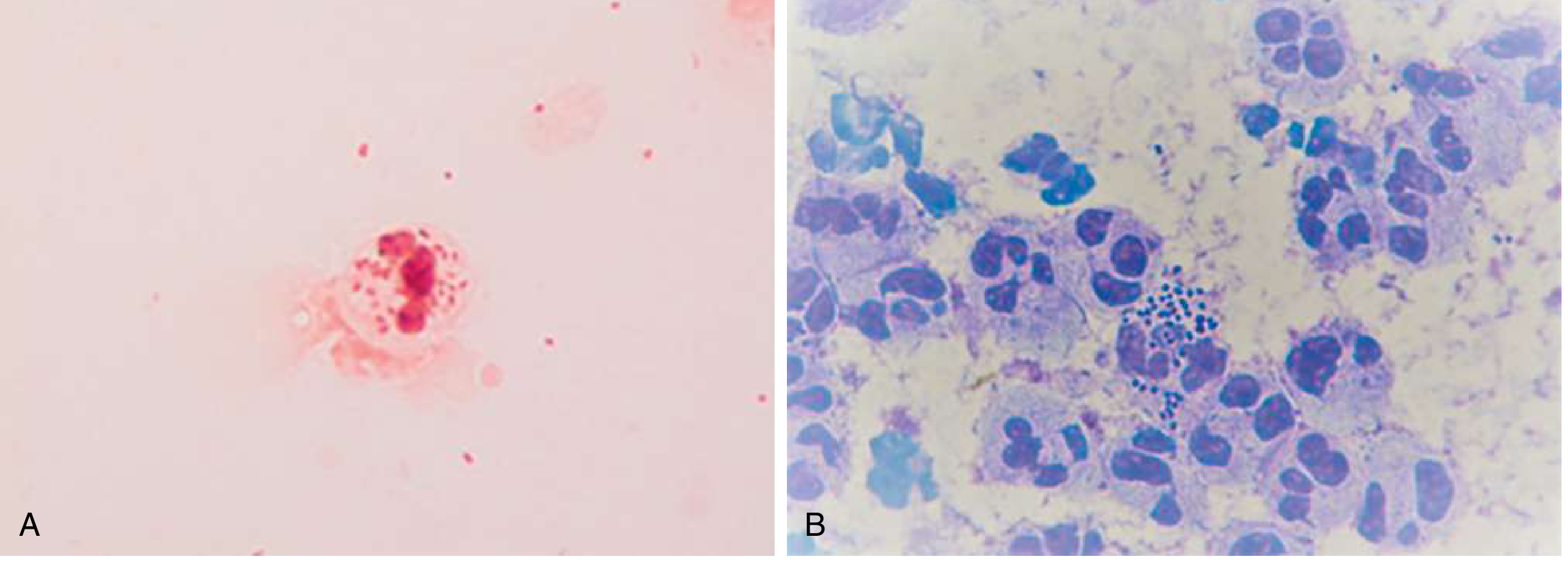
Point-of-Care: Gram Stain
The diagnostic standard when available:
- Positive: polymorphonuclear leukocytes (PMNs) with intracellular gram-negative diplococci (IGNDs) = diagnostic for GU in symptomatic men
- Sensitivity ~95% in symptomatic men with discharge; lower in asymptomatic cases
- A negative Gram stain does not rule out GU
NAAT (Nucleic Acid Amplification Test) - Preferred Method
- Higher sensitivity than culture or microscopy; now the preferred diagnostic modality
- Specimen: first-catch urine or urethral/penile meatal swab in men; urine or self-collected vaginal swab in women
- Can simultaneously test for Chlamydia trachomatis
- Multiple FDA-cleared platforms available for concurrent GC/CT detection
- Not FDA-cleared for rectal, oropharyngeal, or conjunctival specimens - culture preferred there
Culture
-
Requires urethral swab; lower sensitivity than NAAT
-
Collect before NAAT swab to maximize sample
-
Preferred/required in:
- Sexual assault of prepubescent boys
- Suspected treatment failure
- Antimicrobial resistance monitoring
- Rectal, pharyngeal, conjunctival infections
-
Campbell-Walsh-Wein Urology, pp. 1648-1649
Treatment
First-Line (CDC Recommended)
Ceftriaxone 500 mg IM single dose (for most patients) Ceftriaxone 1 g IM if weight >150 kg If Chlamydia co-infection cannot be excluded: + Doxycycline 100 mg PO BID x 7 days
Note: Older regimens used ceftriaxone 250 mg + azithromycin 1 g. CDC updated recommendations (2020 onwards) to ceftriaxone 500 mg monotherapy after rising azithromycin resistance.
Antibiotic Resistance - Key Concern
N. gonorrhoeae has developed resistance to virtually every class used historically:
| Antibiotic class | Resistance status |
|---|---|
| Penicillin | ~16% resistant |
| Tetracycline | ~25% resistant |
| Fluoroquinolones (ciprofloxacin) | ~19% resistant; no longer recommended |
| Azithromycin | Rising reduced susceptibility; removed from first-line |
| Cefixime (oral cephalosporin) | Reduced susceptibility emerging (0.8%) |
| Ceftriaxone | Low (<0.1%) - current mainstay |
The Gonococcal Isolate Surveillance Project (GISP) monitors US resistance trends since 1986.
Alternative Regimens (if ceftriaxone unavailable)
- Cefixime 800 mg PO single dose (less preferred due to resistance trends)
- Gentamicin 240 mg IM + azithromycin 2 g PO (for cephalosporin allergy)
Treatment Failure
Defined as:
- No symptom resolution within 3-5 days AND no sexual contact in that period
- Positive test-of-cure without sexual contact
Action: obtain culture with antimicrobial susceptibility testing.
- Campbell-Walsh-Wein Urology, pp. 1648-1649
Post-Treatment Management
- Test for co-infections: Chlamydia, syphilis, HIV (all patients with gonorrhea)
- Sexual abstinence: for 7 days after treatment AND until all partners are treated
- Partner notification: all sexual contacts within 60 days of symptom onset should be evaluated, tested, and presumptively treated
- Test-of-cure: recommended at 3-4 months given high rates of reinfection
- Expedited partner therapy (EPT) should be considered
Differential Diagnosis of Urethral Discharge
| Cause | Discharge | Onset | Key features |
|---|---|---|---|
| N. gonorrhoeae | Profuse, purulent, yellow-green | 2-6 days | IGNDs on Gram stain |
| C. trachomatis | Thin, clear-gray | 7-21 days | Most common NGU cause |
| M. genitalium | Thin | Variable | 2nd most common NGU cause |
| Ureaplasma urealyticum | Minimal | Variable | Weak association, young men |
| T. vaginalis | Variable | Variable | High prevalence regions |
| HSV/adenovirus | Scant | Variable | May have vesicles/systemic Sx |
- Textbook of Family Medicine 9e; Campbell-Walsh-Wein Urology
Recent Guideline Update (2025-2026)
The German evidence-based guideline on penile urethritis (2025) and recent BASHH NGU guideline 2026 both emphasize the growing role of point-of-care NAAT testing and highlight M. genitalium as an increasingly important pathogen in treatment-refractory urethritis. These guidelines reinforce dual-organism testing (GC+CT) as the standard at first presentation.
This is a shared conversation. Sign in to Orris to start your own chat.