Sciatica
Reading File
Finding Sources
Searching PubMed
sciatica lumbar radiculopathy treatment
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Now I have comprehensive information from multiple authoritative textbooks. Let me compose the full answer.
Sciatica (Lumbar Radiculopathy)
Definition
Sciatica refers to pain radiating along the course of the sciatic nerve, from the lower back into the buttock, posterior/lateral thigh, and leg. In strict clinical use, it results from compression or irritation of the lumbar or sacral nerve roots (most commonly L4, L5, or S1) and is synonymous with lumbar radiculopathy. The term is sometimes applied loosely to any leg pain radiating from the back.
Anatomy and Mechanism
The sciatic nerve is formed from the L4-S1 nerve roots. Disc herniation - especially at L4-L5 or L5-S1 - causes the nucleus pulposus to bulge posterolaterally, compressing the exiting nerve root. The image below illustrates this mechanism:

Protruded discs at L4-L5 and L5-S1 compressing the L5 and S1 roots respectively - Adams and Victor's Principles of Neurology, 12th Ed.
Causes
Most common:
- Herniated lumbar disc (L4-L5 and L5-S1 most frequently)
- Lumbar spinal stenosis (spondylotic - degenerative hypertrophy compressing the lateral recess or central canal)
Less common but important (differential diagnosis per Goldman-Cecil Medicine):
| Category | Examples |
|---|---|
| Neurogenic - spinal | Herniated nucleus pulposus, central/lateral stenosis, synovial cyst, facet hypertrophy, arachnoiditis, tumor (neurofibroma, ependymoma, metastatic), epidural abscess, herpes zoster, Lyme disease |
| Neurogenic - extraspinal | Lumbosacral plexopathy, sciatic neuropathy, peripheral neuropathy, piriformis syndrome |
| Non-neurogenic | Hip arthritis, trochanteric bursitis, sacroiliac disease, iliotibial band syndrome, peripheral vascular disease |
Special causes:
- Piriformis syndrome - the piriformis muscle overlies (or in some individuals embeds) the sciatic nerve; spasm or hypertrophy can cause buttock pain with sciatic radiation
- Catamenial sciatica - endometriosis involving the sciatic nerve at the sciatic notch, pain timed to the premenstrual period
- Pregnancy-related - uterine traction on the nerve; referred back/leg pain in the third trimester is common
- Cauda equina compression - a large L4-5 or L5-S1 herniation, tumor, abscess, or hematoma causing bilateral leg symptoms, saddle anesthesia, and sphincter dysfunction (surgical emergency)
Root-Level Syndromes
| Disc Level | Root | Pain Distribution | Weakness | Reflex |
|---|---|---|---|---|
| L3-L4 | L4 | Anterolateral thigh, medial foreleg | Anterior tibialis (may cause foot drop) | Diminished/absent knee jerk |
| L4-L5 | L5 | Posterolateral gluteal, lateral thigh, anterolateral foreleg, dorsal foot, great toe | Extensor hallucis longus, extensor digitorum brevis | Unaffected (posterior tibial variable) |
| L5-S1 | S1 | Midgluteal, posterior thigh, posterolateral leg, lateral foot, heel, lateral toes | Plantar flexors, hamstrings | Absent/diminished ankle jerk |
- Adams and Victor's Principles of Neurology, 12th Ed., Table 10-1
Clinical Features
- Shooting, burning, or lancinating pain from the buttock down the leg
- Paresthesias (numbness, tingling) in the dermatomal distribution
- Weakness in the corresponding myotome
- Positive straight-leg raise (SLR) test - elicits radicular pain at 30-70 degrees of hip flexion (most useful for L5/S1)
- Loss of the ankle reflex (S1 root) is the single most reliable sign of disc herniation at L5-S1
Diagnosis
- Clinical: history + physical exam (SLR, neurologic exam) is usually sufficient for typical presentations
- MRI is the imaging of choice - confirms herniation, stenosis, and excludes serious pathology (tumor, abscess, fracture)
- CT if MRI is contraindicated
- EMG/NCS - useful when the clinical level is uncertain or to distinguish radiculopathy from peripheral neuropathy or plexopathy
- Diffusion tensor MRI of lumbosacral nerve roots is a newer technique under evaluation for quantitative nerve assessment (PMID: 38190195)
Red flags requiring urgent MRI: bilateral leg symptoms, saddle anesthesia, bowel/bladder dysfunction (cauda equina syndrome), fever + back pain, known malignancy, rapid neurologic worsening.
Treatment
Conservative (first-line, 6-12 weeks)
- Natural history is favorable: sciatica resolves without treatment in ~1/3 of patients within 2 weeks and in ~3/4 within 3 months
- Activity modification - avoid aggravating postures; strict bed rest is NOT superior to staying active
- Analgesics: NSAIDs first-line; short-course opioids for severe pain
- Short course of oral corticosteroids (e.g., dexamethasone) may give temporary relief in severe cases, though systematic reviews show uncertain benefit
- Physical therapy - core strengthening, posture correction; manipulation has modest benefit at best for acute pain
- Pregabalin is NOT helpful for acute or chronic sciatica (Goldman-Cecil Medicine, p. 3846)
Epidural Corticosteroid Injections
- Provide minor short-term pain relief for 2-6 weeks only
- Do NOT improve function or provide pain relief beyond 3 months
- No evidence they prevent eventual surgery
- May be useful as a temporizing measure to allow mobilization in selected patients
A 2024 systematic review of clinical practice guidelines (PMID: 38629664) reviewed medication recommendations across guidelines for lumbosacral radiculopathy - worth consulting for current consensus.
Surgical
Indications:
- Cauda equina syndrome (urgent/emergent)
- Severe or progressive neurologic deficit
- Failure of conservative management (typically after 6-12 weeks)
- Intractable, disabling pain with confirmed root compression on imaging
- Spinal instability
Options:
- Microdiscectomy or open discectomy - superior to conservative therapy at 6 months for pain relief; by 1-2 years, outcomes converge (SPORT trial data)
- Patients who elect early surgery get faster relief but similar long-term outcomes to those who delay
- For persistent sciatica (4-12 months), surgery is better than conservative care at 6 and 12 months
- Minimally invasive approaches are not clearly superior to standard approaches
A 2025 meta-analysis (PMID: 40488872) examined how symptom duration affects discectomy outcomes - longer pre-operative duration may worsen results, supporting earlier surgical decision-making in appropriate patients.
Prognosis
Most patients with sciatica from disc herniation recover without surgery. Neurologic deficits (weakness, reflex loss) tend to lag behind pain resolution. Single-level disease without extensive degenerative changes is associated with better and more durable surgical outcomes. Recurrence is common in degenerative spine disease.
Sources: Adams and Victor's Principles of Neurology (12th Ed.) | Goldman-Cecil Medicine (International Ed.) | Tintinalli's Emergency Medicine
GLP 1 RA
Reading File
Finding Sources
Searching PubMed
"GLP-1 receptor agonist" cardiovascular outcomes
Finding Sources
Searching PubMed
semaglutide obesity weight loss
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have everything needed for a comprehensive answer. Here it is:
GLP-1 Receptor Agonists (GLP-1 RAs)
Mechanism of Action
GLP-1 (glucagon-like peptide-1) is an incretin hormone secreted by L cells in the small intestinal mucosa in response to food. It is rapidly degraded by the enzyme dipeptidyl peptidase-4 (DPP-4), giving it a very short half-life that makes the native peptide unsuitable for therapy.
GLP-1 RAs are synthetic peptides engineered to resist DPP-4 degradation. They bind the GLP-1 receptor and produce several effects:
- Glucose-dependent insulin secretion from pancreatic beta cells (insulin release only when glucose is elevated - low hypoglycemia risk)
- Glucagon suppression from alpha cells (glucose-dependent)
- Delayed gastric emptying - blunts postprandial glucose excursions
- Central appetite suppression via CNS receptors - reduces food intake and body weight
- Beta cell preservation - reduces apoptosis in human islets in culture
Because the insulin-stimulating effect is glucose-dependent, GLP-1 RAs carry a low intrinsic hypoglycemia risk as monotherapy.
Individual Agents
| Drug | Source / Structure | Half-life | Dosing | HbA1c Reduction | Weight Loss |
|---|---|---|---|---|---|
| Exenatide | Exendin-4 (Gila monster venom); 53% GLP-1 homology | ~10 h | 5-10 mcg SC twice daily | 0.2-1.2% | 2-3 kg |
| Exenatide XR | Extended-release microspheres | ~1 week | 2 mg SC once weekly | slightly > twice-daily | similar |
| Liraglutide | Human GLP-1 analog; C16 acyl chain → albumin binding | ~12 h | 0.6-1.8 mg SC once daily (3 mg for obesity) | 0.8-1.5% | up to 3.2 kg |
| Dulaglutide | Two GLP-1 analogs fused to IgG4 Fc fragment | ~5 days | 0.75-4.5 mg SC once weekly | ~1.5% | moderate |
| Lixisenatide | Exendin-4 analog (+6 lysines) | ~3 h | 10-20 mcg SC once daily | 0.4-0.6% | 1-3 kg |
| Semaglutide (SC) | GLP-1 analog; Aib substitution at pos. 8 + C18 fatty diacid chain | ~1 week | 0.25→0.5→1→2 mg SC once weekly | 1.5-1.8% | substantial |
| Semaglutide (oral) | Coformulated with SNAC absorption enhancer | ~1 week | 3→7→14 mg PO once daily | 0.8-1.3% | 2-4 kg |
| Semaglutide 2.4 mg | Same molecule, higher dose | ~1 week | 2.4 mg SC weekly | - (obesity indication) | ~15% body weight |
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
Tirzepatide - Dual GIP/GLP-1 Agonist
Tirzepatide is an analog of GIP (not GLP-1) engineered to also activate GLP-1 receptors. The eicosanedioic acid acylation allows albumin binding and once-weekly dosing. Starting dose 2.5 mg SC weekly, titrated by 2.5 mg every 4 weeks to a maximum of 15 mg.
- HbA1c reduction: 1.9-2.6% (superior to any pure GLP-1 RA)
- Weight loss: 6.2-12.9 kg in T2DM; up to ~20% body weight in obesity trials
- FDA approved for T2DM (2022) and chronic weight management (2023)
- GIP action in the brain appears to act synergistically with GLP-1 receptor activation to produce greater weight loss
Approved Indications
- Type 2 diabetes - all agents listed above
- Obesity / weight management (separate higher-dose formulations):
- Liraglutide 3 mg daily (Saxenda)
- Semaglutide 2.4 mg weekly (Wegovy)
- Tirzepatide (Zepbound)
- Cardiovascular risk reduction in T2DM with established ASCVD (liraglutide, dulaglutide, semaglutide)
Treatment Algorithm (Type 2 Diabetes)
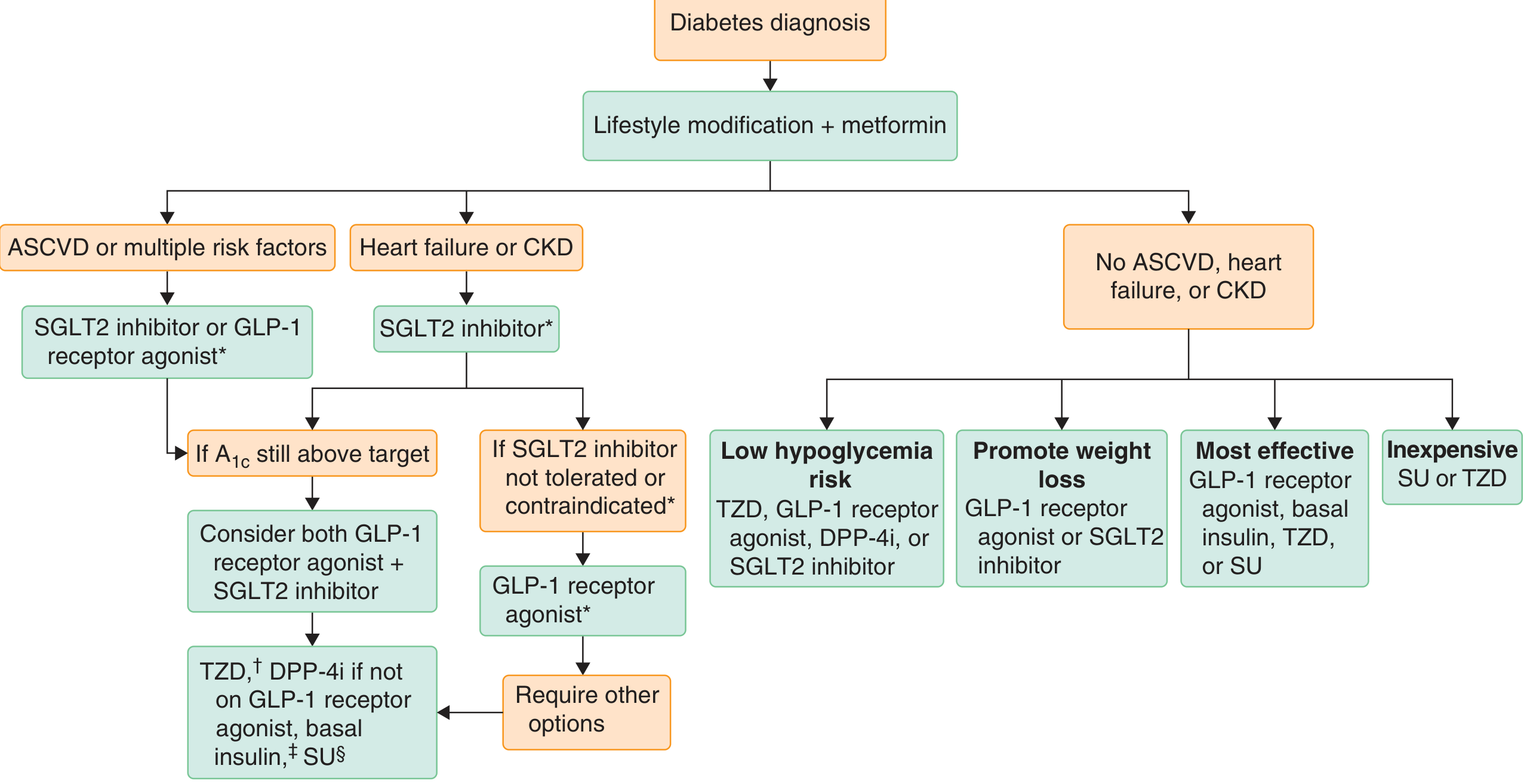
Goldman-Cecil Medicine - T2DM pharmacotherapy algorithm. GLP-1 RAs are preferred when ASCVD is present, weight loss is a goal, or hypoglycemia risk reduction is prioritized.
Cardiovascular & Renal Benefits
Cardiovascular (CVOT data)
- Liraglutide (LEADER trial): HR 0.87 for MACE (CV death, non-fatal MI, non-fatal stroke) vs. placebo in patients with established CVD
- Semaglutide (SUSTAIN-6): reduced MACE; note - increased diabetic retinopathy events observed, likely due to rapid glucose lowering
- Dulaglutide (REWIND): reduced MACE; included patients with only CV risk factors (not just established disease)
- Oral semaglutide (PIONEER 6): also reduced CV events
A 2025 Lancet Diabetes & Endocrinology meta-analysis of RCTs (PMID: 39608381) confirmed GLP-1 RAs reduce MACE, kidney disease progression, and CV death, particularly in high-risk patients.
Renal
- GLP-1 RAs reduce albuminuria and slow GKD progression in T2DM
- A 2025 Cochrane review (PMID: 39963952) and a 2025 meta-analysis in AJKD (PMID: 39863261) confirmed renal protective effects, including reduced ESKD and CV death in CKD patients on GLP-1 RAs
Note: Exenatide is renally cleared and should not be used when eGFR <30 mL/min/1.73 m². Other agents (liraglutide, semaglutide, dulaglutide) are generally safer in CKD.
Adverse Effects
| Effect | Notes |
|---|---|
| Nausea / vomiting / diarrhea | Most common; dose-related; worse at initiation, improve over weeks |
| Anorexia / weight loss | Desired effect in most patients |
| Pancreatitis | Rare but reported; use with caution in history of pancreatitis |
| Medullary thyroid carcinoma | C-cell tumors in rodents; contraindicated with personal/family history of MTC or MEN-2 |
| Diabetic retinopathy worsening | Seen with semaglutide in SUSTAIN-6, likely from rapid glucose lowering |
| Injection site reactions | Nodules with exenatide XR microsphere formulation |
| Antibody formation | ~6% with exenatide; ~70% with lixisenatide; attenuated response in a subset |
| Acute gallbladder disease | Increased risk of cholelithiasis / cholecystitis |
| Hypoglycemia | Low with monotherapy; increased when combined with sulfonylureas or insulin |
Contraindications
- Personal or family history of medullary thyroid carcinoma
- MEN type 2
- History of pancreatitis (relative contraindication - use with caution)
- Exenatide: eGFR <30 mL/min/1.73 m²
Weight Loss Efficacy Comparison (placebo-subtracted)
From Harrison's 22nd Edition antiobesity medication table:
| Agent | Placebo-subtracted weight loss |
|---|---|
| Liraglutide 3 mg | 5.4% |
| Semaglutide 2.4 mg | 12.5% |
| Tirzepatide | 17.8% |
A 2024 systematic review and meta-analysis (PMID: 38679221) confirmed long-term efficacy and safety of once-weekly semaglutide for weight loss in non-diabetic patients. A 2025 systematic review (PMID: 40186344) found that discontinuing GLP-1 RAs leads to weight regain, underscoring the need for continued therapy in obesity management.
Key Clinical Points
- GLP-1 RAs are preferred in T2DM with established ASCVD, multiple CV risk factors, or when weight loss is a goal
- They are distinct from DPP-4 inhibitors (which extend native GLP-1 action but produce more modest effects)
- The oral semaglutide formulation requires an empty stomach and no food/water for 30 minutes after ingestion for adequate absorption
- Semaglutide at 2.4 mg dose is approved for weight loss even in non-diabetic patients (BMI ≥30 or ≥27 with weight-related comorbidity)
- Tirzepatide consistently outperforms pure GLP-1 RAs on both HbA1c reduction and weight loss due to its dual GIP/GLP-1 mechanism
Sources: Katzung's Basic and Clinical Pharmacology (16th Ed.) | Goldman-Cecil Medicine (International Ed.) | Harrison's Principles of Internal Medicine (22nd Ed., 2025) | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.