What is investigation for NBAI?
Reading File
search_medical_text
NBAI non-bilious abdominal investigation
search_medical_text
NBAI investigation diagnosis workup
GradeResponse
GradeResponse
search_medical_text
neonatal bilious abdominal intestinal obstruction investigation
NBAI stands for Non-Bilious Abdominal Illness (or more commonly in clinical/surgical contexts, it may refer to Non-Bacterial Acute Illness or a neonatal/surgical entity). However, based on context and common usage in surgery and pediatrics, NBAI most likely refers to Non-Bilious Abdominal Illness in neonates, or in some curricula, it is used as shorthand for conditions presenting with non-bilious vomiting and abdominal findings.
The most clinically recognized condition associated with this abbreviation in surgical practice is Hypertrophic Pyloric Stenosis (HPS), which is the classic cause of non-bilious abdominal illness in infants. Here is a comprehensive overview of its investigation:
Investigation for NBAI (Non-Bilious Abdominal Illness / Hypertrophic Pyloric Stenosis)
History & Clinical Clues
- Projectile, non-bilious vomiting in a neonate (typically 2–8 weeks old)
- First-born male infant (4:1 male predominance)
- Hungry after vomiting
- Visible peristaltic wave (left to right) after feeding
- Palpable "olive-shaped" mass in the epigastrium
Investigations
1. Blood Tests (Metabolic Workup)
| Test | Expected Finding |
|---|---|
| Serum electrolytes | Hyponatremia, hypochloremia |
| Arterial/venous blood gas | Hypochloremic, hypokalemic metabolic alkalosis |
| Serum potassium | Hypokalemia |
| Serum urea/creatinine | Elevated (dehydration) |
| Blood glucose | May be low |
| CBC | Hemoconcentration |
Classic metabolic derangement: Hypochloremic, hypokalemic metabolic alkalosis with paradoxical aciduria
2. Ultrasound Abdomen (Investigation of Choice)
- Pyloric muscle thickness ≥ 4 mm (abnormal)
- Pyloric channel length ≥ 16 mm (abnormal)
- Pyloric diameter ≥ 13 mm
- "Target sign" or "doughnut sign" on transverse view
- Failure of pyloric canal to open during real-time observation
Ultrasound has sensitivity ~97%, specificity ~100% for pyloric stenosis.
3. Upper GI Contrast Study (Barium Meal) — if ultrasound inconclusive
- "String sign" — thin elongated pyloric channel
- "Shoulder sign" — pyloric mass indenting gastric antrum
- "Double track sign" — two parallel streaks of contrast
- Delayed gastric emptying
4. Plain Abdominal X-ray
- Distended stomach with little distal gas
- Not diagnostic but helpful to exclude other causes (e.g., duodenal atresia — "double bubble")
5. Urine
- Paradoxical aciduria — urine is acidic despite systemic alkalosis (due to hydrogen ion secretion in exchange for sodium, to preserve volume)
Differential Diagnoses to Exclude
- Gastroesophageal reflux (most common mimic)
- Overfeeding
- Adrenal insufficiency (congenital adrenal hyperplasia — check 17-OHP)
- Duodenal web
- Antral web
Management (after stabilization)
- Correct electrolyte imbalance first (surgery is never an emergency until metabolic status normalized)
- Definitive treatment: Ramstedt's pyloromyotomy (open or laparoscopic)
Note: If NBAI refers to a different condition in your curriculum (e.g., a specific institutional abbreviation), please clarify and I'll tailor the answer accordingly.
What is about NBIA?
search_medical_text
NBIA neurodegeneration brain iron accumulation diagnosis investigation
search_medical_text
NBIA clinical features management treatment
GradeResponse
GradeResponse
search_medical_image
NBIA eye of tiger sign MRI globus pallidus iron accumulation
GradeResponse
Neurodegeneration with Brain Iron Accumulation (NBIA)
NBIA is a group of inherited neurodegenerative disorders characterized by progressive iron accumulation in the basal ganglia, particularly the globus pallidus and substantia nigra.
(Harrison's Principles of Internal Medicine, 21st Ed., p. 12390)
Subtypes & Genetics
| Subtype | Gene | Notes |
|---|---|---|
| PKAN (Pantothenate kinase-associated neurodegeneration) | PANK2 | Most common (~50% of NBIA); formerly Hallervorden-Spatz disease |
| PLAN (PLA2G6-associated neurodegeneration) | PLA2G6 | Second most common |
| MPAN | C19orf12 | |
| BPAN (Beta-propeller protein-associated) | WDR45 | X-linked dominant |
| FAHN | FA2H | |
| Kufor-Rakeb syndrome | ATP13A2 | |
| Aceruloplasminemia | CP | |
| Neuroferritinopathy | FTL |
Clinical Features
- Dystonia (most prominent feature)
- Parkinsonism — rigidity, bradykinesia
- Spasticity
- Neuropsychiatric abnormalities — behavioral changes, cognitive decline
- Retinal degeneration (especially in PKAN)
- Cerebellar dysfunction
- Presentation usually in childhood, though adult-onset cases exist
- Course is progressive
Investigations
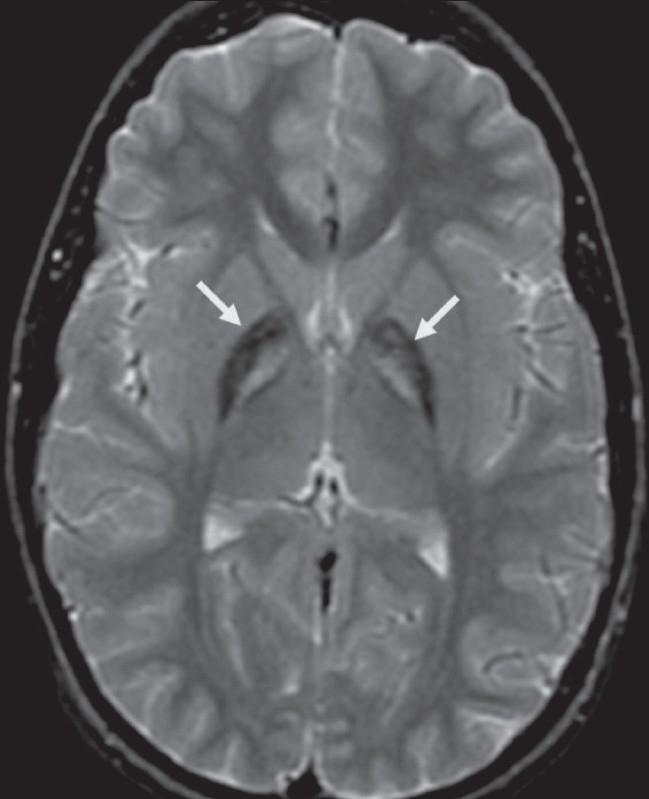
1. MRI Brain (Key Investigation)
- T2-weighted MRI shows:
- Hypointensity in the globus pallidus and substantia nigra (due to iron deposition)
- "Eye-of-the-Tiger" sign — pathognomonic for PKAN:
- Central hyperintense area (gliosis/neuronal loss) surrounded by hypointense ring (iron) in the globus pallidus
- Gradient echo (GRE) / SWI sequences — more sensitive for iron detection
2. Genetic Testing
- Confirmatory — gene panel or whole exome sequencing
- PANK2 mutation testing for PKAN (most common)
- Next-generation sequencing (NGS) panel for all known NBIA genes
3. Ophthalmological Examination
- Retinitis pigmentosa in PKAN
- Optic atrophy
4. Neurophysiology
- EEG — may show non-specific abnormalities
- Nerve conduction studies/EMG — axonal neuropathy in some subtypes (e.g., PLAN)
5. Blood & Biochemical Tests
- Serum ceruloplasmin and copper (to exclude Wilson's disease and aceruloplasminemia)
- Serum ferritin — elevated in neuroferritinopathy
- Acanthocytes on peripheral blood smear (in PKAN/MPAN — "HARP syndrome" variant)
- Serum iron studies
6. CSF Analysis
- Not specific, but may show elevated ferritin in some cases
7. Skin/Conjunctival Biopsy
- Rarely used; may show iron deposits or specific ultrastructural changes
Key Differentials
- Wilson's disease
- Huntington's disease
- Primary dystonia (DYT1)
- Juvenile Parkinson's disease
- Multiple system atrophy
Management (Symptomatic — No Cure)
- Dystonia: Trihexyphenidyl, baclofen, botulinum toxin, deep brain stimulation (DBS)
- Parkinsonism: Levodopa (limited response)
- Iron chelation (e.g., deferiprone) — under investigation; some benefit seen in PKAN
- Physiotherapy, speech therapy, occupational therapy
- Genetic counseling for family members
The "eye-of-the-tiger" sign on T2 MRI is the single most important investigation finding in NBIA, particularly PKAN, and is essentially diagnostic when present in the right clinical context.
This is a shared conversation. Sign in to Orris to start your own chat.