Chapter no 7 - labour from William book give in easy notes
Reading File
search_medical_text
labour chapter 7 Williams Obstetrics stages mechanisms
search_medical_text
normal labour definition onset uterine contractions cervical dilation
GradeResponse
GradeResponse
search_medical_text
stages of labour first second third stage management
search_medical_text
mechanisms of labour cardinal movements engagement descent flexion rotation
Here are easy notes on Chapter 7 – Labour from Williams Obstetrics:
📘 Chapter 7 – Labour (Williams Obstetrics)
1. Definition of Labour
Labour is defined as the presence of regular, painful uterine contractions that result in:
- Cervical effacement (thinning of cervix)
- Cervical dilation (opening of cervix)
- Or both
Note: Labour onset is sometimes hard to pinpoint — hospital admission may underestimate how long early labour has been going on.
2. Stages of Labour
| Stage | Description | Duration (Primigravida) | Duration (Multigravida) |
|---|---|---|---|
| 1st Stage | Onset of true labour → Full cervical dilation (10 cm) | ~12–14 hours | ~6–8 hours |
| 2nd Stage | Full dilation → Delivery of baby | Up to 2 hours | Up to 1 hour |
| 3rd Stage | Delivery of baby → Delivery of placenta | 5–30 minutes | 5–30 minutes |
First Stage is Further Divided:
- Latent phase: Cervix dilates from 0 → 6 cm (slow)
- Active phase: Cervix dilates from 6 → 10 cm (faster, ≥1 cm/hr expected)
3. True vs. False Labour
| Feature | True Labour | False Labour (Braxton Hicks) |
|---|---|---|
| Contractions | Regular, increasing intensity | Irregular |
| Cervical change | Yes | No |
| Pain location | Back + abdomen | Abdomen only |
| Response to walking | Increases | Decreases/stops |
4. Cardinal Movements of Labour (Mechanisms)
These are the movements the fetal head makes to pass through the pelvis:
- Engagement – Head enters the pelvic inlet (biparietal diameter at level of ischial spines)
- Descent – Head moves downward through the pelvis
- Flexion – Chin tucks to chest (presents smallest diameter)
- Internal Rotation – Head rotates from transverse → anterior-posterior
- Extension – Head extends as it passes under the pubic symphysis → delivery of head
- External Rotation (Restitution) – Head rotates back to align with shoulders
- Expulsion – Anterior then posterior shoulder delivered → rest of body follows
5. Uterine Contractions
- Originate from pacemaker cells near the uterine cornua
- Spread downward (fundal dominance)
- Normal contractions: 3–5 per 10 minutes, lasting 45–60 seconds
- Pressure: 50–80 mmHg during contraction
6. Cervical Changes
- Effacement: Cervix thins and shortens (0–100%)
- Dilation: Cervix opens (0–10 cm)
- In primigravida: effacement usually occurs before dilation
- In multigravida: effacement and dilation occur together
7. Fetal Monitoring in Labour
- CTG (Cardiotocography) is used to monitor fetal heart rate
- Normal fetal heart rate: 110–160 bpm
- Key features: baseline rate, variability, accelerations, decelerations
8. Management of Each Stage
First Stage:
- Monitor contractions and cervical dilation (partogram)
- Assess fetal well-being (CTG)
- IV access, analgesia if needed
- Encourage ambulation in latent phase
Second Stage:
- Push with contractions (active pushing)
- Support perineum
- Deliver head slowly to avoid tears
- Check for nuchal cord
Third Stage:
- Active management is preferred:
- Give oxytocin 10 IU IM after delivery of baby
- Controlled cord traction
- Uterine massage
9. Complications of Labour
| Complication | Key Point |
|---|---|
| Prolonged labour | Latent phase >20 hrs (primi), >14 hrs (multi) |
| Labour arrest | Active phase: no dilation in >4 hrs with adequate contractions |
| Precipitate labour | Delivery in <3 hours — risk of fetal/maternal injury |
| Fetal distress | Abnormal CTG — may need emergency LSCS |
| Postpartum hemorrhage | Blood loss >500 mL — oxytocin is first-line treatment |
10. Key Terms to Remember
| Term | Meaning |
|---|---|
| Effacement | Cervix shortens/thins |
| Dilation | Cervix opens |
| Show | Mucus plug discharge — sign of early labour |
| ROM | Rupture of membranes |
| PROM | Premature rupture of membranes (before labour) |
| Engagement | Fetal head enters pelvic inlet |
| Station | Position of presenting part relative to ischial spines (−5 to +5) |
These notes cover the core concepts of Chapter 7 — Labour from Williams Obstetrics. For exam preparation, focus especially on stages of labour, cardinal movements, and active management of 3rd stage.
Positions of baby in uterus
Reading File
Finding Sources
Finding Sources
Searching Images
fetal positions in uterus lie presentation vertex breech transverse
Reading File
Reading File
Loading Image
Loading Image
Here are easy, well-illustrated notes on Positions of the Baby in the Uterus:
👶 Positions of the Baby in the Uterus
Key Terms (Must Know First)
| Term | Meaning |
|---|---|
| Lie | Relationship of the baby's long axis to the mother's long axis |
| Presentation | The part of the baby closest to the birth canal (pelvic inlet) |
| Position | Relationship of the presenting part to the mother's pelvis |
| Attitude | The posture of the baby's body parts |
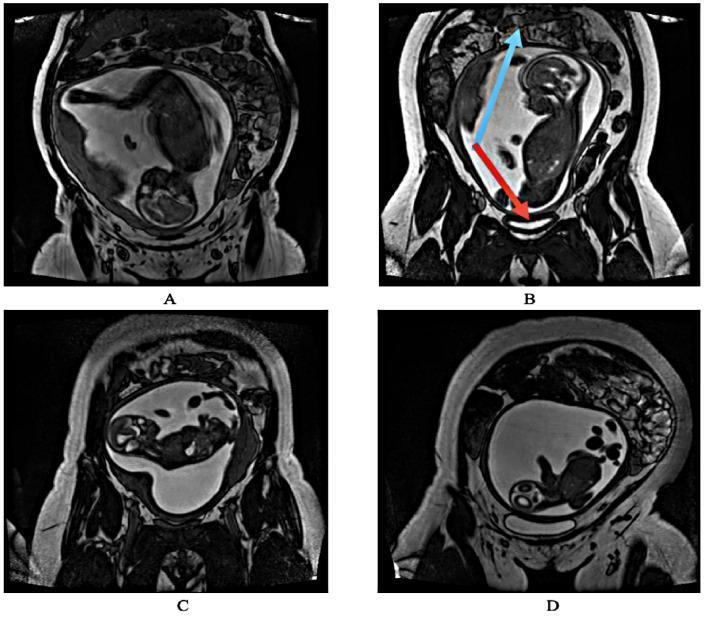
1. Fetal LIE
The lie tells us how the baby is oriented inside the uterus.
| Type | Description | Frequency |
|---|---|---|
| Longitudinal | Baby's spine parallel to mother's spine | 99% (normal) |
| Transverse | Baby lying sideways across the uterus | ~1 in 300 deliveries |
| Oblique | Baby at a diagonal angle | Uncommon, usually temporary |
MRI showing all four lies:
2. Fetal PRESENTATION
Presentation = what part enters the pelvis first.
A. Cephalic (Head-First) — Most Common ✅
The head is down. This is the normal and safest position for delivery.
Sub-types based on head position:
| Sub-type | Head Position | Presenting Diameter |
|---|---|---|
| Vertex (most common) | Head fully flexed, chin on chest | Smallest — suboccipitobregmatic (~9.5 cm) |
| Sinciput | Partially flexed | Medium |
| Brow | Partially extended | Larger — difficult delivery |
| Face | Fully extended, face presents | Mentum (chin) is the denominator |
B. Breech (Bottom/Feet First) — ~3–4% of term pregnancies
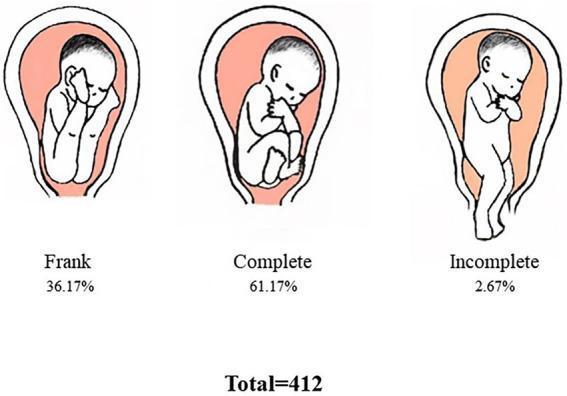
| Type | Description | Frequency |
|---|---|---|
| Frank Breech | Hips flexed, knees straight (legs up by head) | Most common ~36% |
| Complete Breech | Hips & knees both flexed (cross-legged) | ~61% |
| Incomplete/Footling | One or both feet presenting | ~2–3% |
Usually managed by caesarean section or External Cephalic Version (ECV) to turn baby head-down before labour.
C. Transverse Lie / Shoulder Presentation
- Baby lies horizontally across the uterus
- Shoulder is the presenting part
- Cannot deliver vaginally — caesarean section required
- Associated with: prematurity, high parity, placenta previa, polyhydramnios
- Risk of cord prolapse if membranes rupture — obstetric emergency!
(Creasy & Resnik's Maternal-Fetal Medicine)
3. Fetal POSITION
Position describes where the denominator (reference point of presenting part) points in the maternal pelvis.
| Presentation | Denominator |
|---|---|
| Vertex | Occiput (O) |
| Face | Mentum (M) |
| Breech | Sacrum (S) |
| Shoulder | Acromion (A) |
Common Positions in Vertex Presentation:
| Abbreviation | Full Name | Details |
|---|---|---|
| LOA | Left Occiput Anterior | Most common, favourable |
| ROA | Right Occiput Anterior | Favourable |
| LOT | Left Occiput Transverse | Common in early labour |
| ROT | Right Occiput Transverse | Common in early labour |
| LOP | Left Occiput Posterior | Causes back labour, slower |
| ROP | Right Occiput Posterior | Causes back labour, slower |
| OA | Occiput Anterior | Ideal for delivery |
| OP | Occiput Posterior | "Sunny-side up" — prolonged labour |
4. Fetal ATTITUDE
Attitude = how the baby's body parts are folded/flexed.
- Good flexion (chin on chest): presents the smallest head diameter → easy delivery
- Deflexion (head extended): presents a larger diameter → difficult delivery
5. Causes of Abnormal Fetal Position
- Placenta previa (blocks normal head engagement)
- Polyhydramnios (too much fluid → baby floats freely)
- Uterine abnormalities (fibroids, bicornuate uterus)
- Multiple pregnancy
- Grand multiparity (lax uterine muscles)
- Pelvic tumours
- Prematurity
6. How Position is Assessed
| Method | What It Checks |
|---|---|
| Leopold's Manoeuvres | Abdominal palpation — determines lie, presentation, engagement |
| Vaginal examination | Confirms presentation and position during labour |
| Ultrasound | Gold standard for confirming position |
Quick Summary Table
| Longitudinal Lie | Transverse Lie | |
|---|---|---|
| Sub-type | Cephalic (vertex/face) or Breech | Shoulder |
| Delivery | Vaginal (usually) | C-section required |
| Frequency | 99% | ~1 in 300 |
| Risk | Minimal (normal) | Cord prolapse, obstructed labour |
The ideal baby position for delivery is Left Occiput Anterior (LOA) with vertex presentation — head down, chin on chest, occiput pointing to the left-front of the mother's pelvis.
Leopold manevure
Reading File
Finding Sources
Finding Sources
Searching Images
Leopold maneuvers abdominal palpation obstetrics four maneuvers
Reading File
Reading File
Loading Image
Loading Image
Here are easy notes on Leopold's Maneuvers from Rosen's Emergency Medicine & Textbook of Family Medicine:
🤲 Leopold's Maneuvers — Easy Notes
What Are They?
Leopold's Maneuvers are 4 steps of abdominal palpation done by a doctor/midwife to find out:
- What part of the baby is at the top (fundus)
- Where the baby's back is
- What part is presenting at the pelvis
- How far the baby has descended / degree of head flexion
When performed: From 30 weeks of gestation onwards (baby is big enough to feel clearly).
Patient position: Mother lies flat on her back (supine), with knees slightly bent and abdomen exposed.
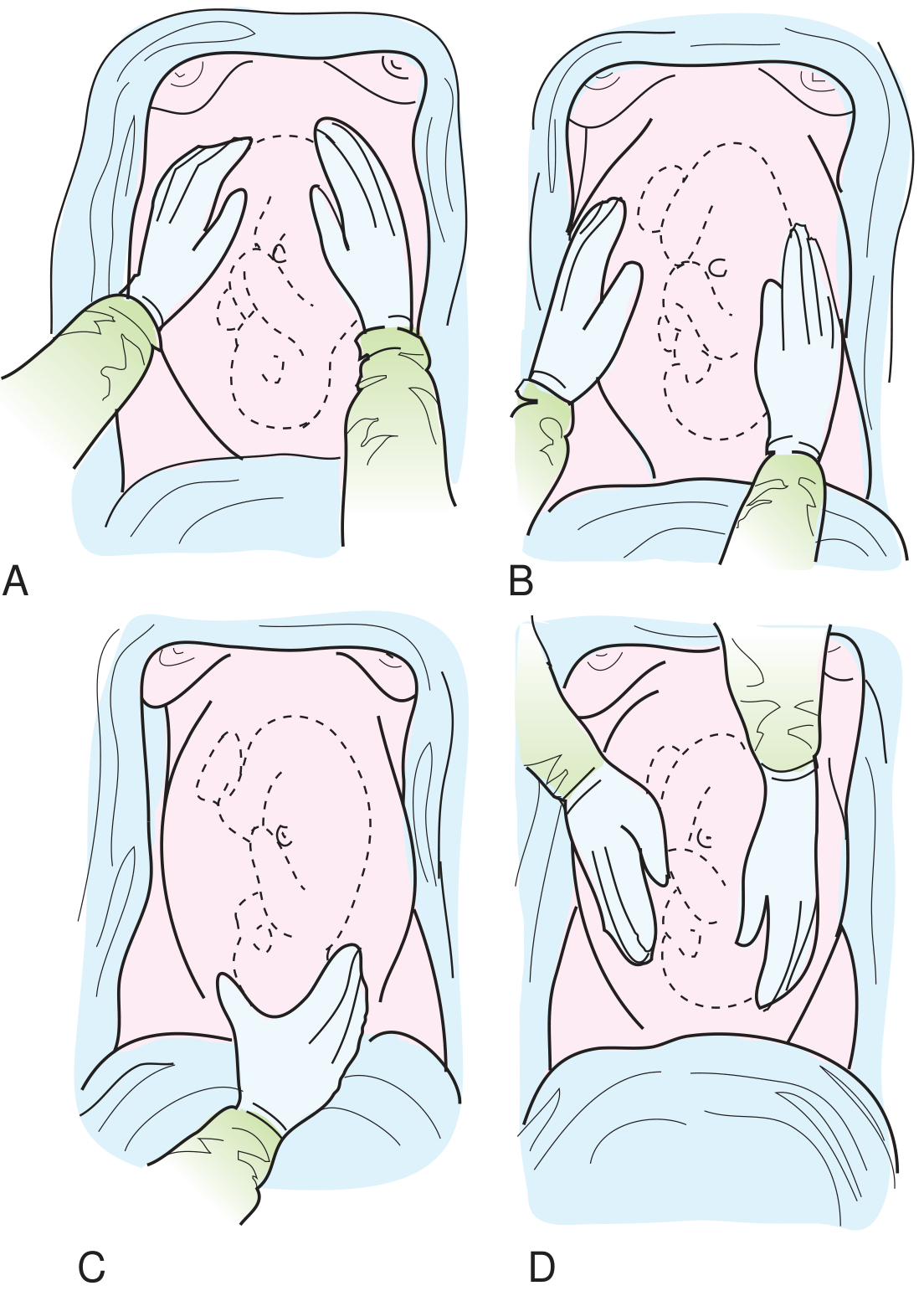
The Four Maneuvers

🅐 1st Maneuver — Fundal Grip
"What is in the fundus (top of the uterus)?"
- Doctor faces the mother's head
- Both hands placed on top of the uterus (fundus)
- Feel what part is there
| Finding | Means |
|---|---|
| Soft, irregular, bulky mass | Breech (buttocks) at fundus → head is down ✅ |
| Hard, round, ballotable mass | Head at fundus → baby is breech ⚠️ |
🅑 2nd Maneuver — Lateral / Umbilical Grip
"Where is the baby's back?"
- Hands slide down the sides of the uterus
- One hand steadies, the other palpates each side
| Finding | Means |
|---|---|
| Firm, smooth, continuous resistance | Baby's back (spine side) |
| Soft, irregular, knobby lumps | Baby's limbs (arms/legs) |
- Back on left side = Left position (LOA, LOT, LOP)
- Back on right side = Right position (ROA, ROT, ROP)
💡 Fetal heart tones are best heard through the back — this helps confirm position!
🅒 3rd Maneuver — Pawlik's Grip (Lower Pole Grip)
"What is presenting at the pelvis?"
- Use one hand (thumb and fingers) just above the symphysis pubis
- Gently grip the presenting part
| Finding | Means |
|---|---|
| Hard, round, smooth, ballotable | Head (cephalic presentation) ✅ |
| Soft, irregular | Breech |
| Nothing felt | Head deeply engaged in pelvis |
- If the part moves freely → not yet engaged
- If fixed/immovable → engaged in pelvis
🅓 4th Maneuver — Pelvic / Pawlik's Second Grip
"How far is the head descended? Is it flexed or extended?"
- Doctor turns to face the mother's feet
- Both hands placed on lower sides of uterus, fingers pointing downward toward the pelvis
- Feel for the cephalic prominence (brow/forehead)
| Finding | Means |
|---|---|
| Cephalic prominence felt on same side as small parts (limbs) | Head is well flexed (vertex) ✅ |
| Cephalic prominence felt on same side as back | Head is extended (face/brow presentation) ⚠️ |
| Hands converge easily (go deep) | Head is deeply engaged |
| Hands diverge (can't go deep) | Head is not engaged |
Quick Summary Table
| Maneuver | Area Examined | Doctor Faces | Answers |
|---|---|---|---|
| 1st — Fundal Grip | Fundus (top) | Mother's head | What's in the fundus? |
| 2nd — Lateral Grip | Sides of uterus | Mother's head | Where is the back? |
| 3rd — Pawlik's Grip | Lower pole / pubis | Mother's head | What is presenting? Engaged? |
| 4th — Pelvic Grip | Pelvis / inlet | Mother's feet | Degree of descent & flexion? |
Memory Trick 🧠
"Fundus → Flanks → Front-low → Flip & Feel"
- Top 2. Sides 3. Lower front 4. Flip around & deep pelvic
Clinical Importance
- Helps diagnose malpresentation (breech, transverse)
- Guides decision for normal delivery vs. caesarean section
- Helps locate best place to listen to fetal heart sounds
- Assesses engagement of the presenting part before labour
(Rosen's Emergency Medicine; Textbook of Family Medicine 9e)
This is a shared conversation. Sign in to Orris to start your own chat.