Can you help me understand most common 10 ecg patterns
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Searching the Web
10 most common ECG patterns clinical interpretation guide
I now have comprehensive material from Braunwald's Heart Disease, Tintinalli's Emergency Medicine, Fuster & Hurst's The Heart, plus web sources. Here is the full, detailed guide:
The 10 Most Common ECG Patterns
How to Read Any ECG (Quick Framework First)
Before pattern recognition, always run through 5 steps systematically:
- Rate - Count R-R intervals (300/large boxes between R peaks, or complexes x 6 on a 10-sec strip)
- Rhythm - Regular or irregular? Regularly irregular or irregularly irregular?
- Axis - Look at leads I and aVF: both up = normal, I up/aVF down = left axis, I down/aVF up = right axis
- Intervals - PR (0.12-0.20s), QRS (<0.12s), QTc
- ST/T waves & morphology - Elevations, depressions, inversions, Q waves
1. Normal Sinus Rhythm (NSR)
The baseline you compare everything else against.
| Parameter | Normal Value |
|---|---|
| Rate | 60-100 bpm |
| P waves | Upright in I, II, aVF; before every QRS |
| PR interval | 0.12-0.20 sec (3-5 small boxes) |
| QRS duration | ≤0.10 sec (≤2.5 small boxes) |
| Rhythm | Regular |
Key teaching point: P wave must precede every QRS with a constant PR interval. If this is present, you have sinus rhythm and can focus on everything else (ST changes, axis, intervals).
2. Sinus Tachycardia
Same as NSR, just fast.
- Rate > 100 bpm, all other morphology normal
- P wave before every QRS, regular rhythm
- Common causes: Pain, fever, hypovolemia, PE, hyperthyroidism, anxiety, drugs (caffeine, stimulants)
- Critical point: Sinus tachycardia is a symptom, not a primary arrhythmia. Always treat the underlying cause. Never cardiovert.
3. Sinus Bradycardia
Same as NSR, just slow.
- Rate < 60 bpm, all other morphology normal
- Common causes: Athletic heart, sleep, increased vagal tone, beta-blockers, hypothyroidism, inferior MI (RCA supplies SA node)
- Treatment: Only if symptomatic (dizziness, syncope, hypotension) - atropine 0.5 mg IV, or transcutaneous pacing in severe cases
4. Atrial Fibrillation (AFib)
The most common sustained cardiac arrhythmia.
From Tintinalli's Emergency Medicine:
"Absence of discernible P waves with flat or chaotic isoelectric baseline. QRS complexes narrow unless preexisting bundle branch block or preexcitation syndrome. Irregularly irregular ventricular rhythm."
| Feature | Finding |
|---|---|
| P waves | Absent - replaced by chaotic fibrillatory baseline (f waves) |
| Rhythm | Irregularly irregular (the hallmark) |
| QRS | Narrow (unless BBB or WPW) |
| Rate | Variable (ventricular rate 100-180 bpm if uncontrolled) |
Clinical consequences: Loss of atrial kick (up to 30% of cardiac output in some patients), risk of thromboembolism (stroke), and rapid ventricular rates. Risk stratify with CHA₂DS₂-VASc score for anticoagulation decisions.
5. AV Blocks (1st, 2nd, 3rd Degree)
Three distinct patterns with very different clinical urgency:
First-Degree AV Block
- PR interval > 0.20 sec (>1 large box), constant
- Every P wave conducts - just delayed
- Usually benign, often no treatment needed
Second-Degree AV Block - Mobitz Type I (Wenckebach)
- PR interval progressively lengthens until a P wave is blocked (no QRS follows)
- Then the cycle resets - "group beating" appearance
- Mnemonic: "Longer, longer, longer... DROP - then you have a Wenckebach"
- Block is at the AV node level - usually benign, rarely needs pacing
Second-Degree AV Block - Mobitz Type II
- PR interval constant, then a P wave is suddenly not conducted (no warning)
- Block is below the AV node (Bundle of His or bundle branches)
- Dangerous - can progress unpredictably to complete block; often requires pacemaker
Third-Degree (Complete) AV Block
- Complete dissociation between P waves and QRS complexes
- P waves march through at their own rate; QRS at their own (escape) rate
- If ventricular escape: wide QRS (20-40 bpm) - medical emergency
- If junctional escape: narrow QRS (40-60 bpm) - more stable but still urgent
- Requires emergent pacing
6. Right Bundle Branch Block (RBBB)
Classic mnemonic: "William MaRRow" - WiRRoW for RBBB
| Feature | Finding |
|---|---|
| QRS duration | ≥ 0.12 sec (≥3 small boxes) - wide complex |
| V1 | rSR' pattern ("rabbit ears" or "M" shaped) |
| V5/V6 | Wide, slurred S wave |
| T waves | Inverted in V1-V2 (right "strain" pattern) |
- Cause: RCA disease, PE (acute RBBB + S1Q3T3), congenital heart disease, normal variant in athletes
- Isolated RBBB rarely progresses to complete heart block - Fuster & Hurst's, p.1233
7. Left Bundle Branch Block (LBBB)
Classic mnemonic: "WiLLiaM" - W in V1, M in V5/V6
| Feature | Finding |
|---|---|
| QRS duration | ≥ 0.12 sec - wide complex |
| V1 | Broad, deep QS or rS wave |
| V5/V6 | Tall, broad, notched R wave - no septal Q |
| Lateral leads | Discordant ST-T changes (ST opposite to QRS direction) |
- New LBBB in a patient with chest pain = STEMI equivalent until proven otherwise (Sgarbossa criteria apply)
- Associated with dilated cardiomyopathy, severe LV disease, worse prognosis
- Fuster & Hurst's: "LBBB in patients with cardiomyopathy is associated with significant ventricular dyssynchrony, worsening HF, and increased mortality."
8. ST-Elevation - STEMI
The most time-critical pattern you will ever see.
- ST elevation ≥ 1 mm in ≥2 contiguous limb leads, or ≥ 2 mm in contiguous precordial leads
- New LBBB counts as STEMI equivalent
- Reciprocal ST depression in opposite leads (confirms true elevation)
Localization by territory:
| Leads with ST Elevation | Territory | Artery |
|---|---|---|
| V1-V4 | Anterior | LAD |
| II, III, aVF | Inferior | RCA (or LCx) |
| I, aVL, V5-V6 | Lateral | LCx |
| V1-V3 (posterior: tall R in V1-V2) | Posterior | RCA/LCx |
| V4R-V5R | Right ventricle | RCA proximal |
From Textbook of Family Medicine: "STEMI occurs secondary to a sudden interruption of coronary blood supply to a part of the myocardium as a result of a complete thrombotic occlusion of a coronary artery. Emergent and complete revascularization is the most important goal - primary angioplasty within 90 minutes (door-to-balloon time)."
Evolutionary changes: Hyperacute T waves → ST elevation → Q wave formation → T inversion → Q waves persist permanently
9. ST Depression and T-Wave Inversions (Ischemia/NSTEMI)
Subendocardial ischemia or NSTEMI pattern:
- ST depression ≥ 0.5 mm in ≥2 contiguous leads
- T-wave inversions (symmetrical, deep T inversions = Wellens' syndrome in V2-V3 = critical LAD stenosis)
- Horizontal or downsloping ST depression is more specific for ischemia than upsloping
Key patterns to know:
- Wellens' A: Biphasic T waves in V2-V3 (deeply ominous - proximal LAD lesion)
- Wellens' B: Deep symmetrical T inversions in V2-V3
- De Winter T waves: Upsloping ST depression + tall peaked T waves in precordial leads = LAD occlusion STEMI equivalent (no ST elevation!)
- Diffuse ST depression + ST elevation in aVR: Left main or proximal LAD occlusion
Strain pattern: Down-sloping ST depression + T inversion in lateral leads (I, aVL, V5-V6) with LVH = "LV strain," not necessarily ischemia
10. Left Ventricular Hypertrophy (LVH)
Very common - seen in hypertension, aortic stenosis, HCM.
Voltage criteria (any one sufficient for diagnosis):
| Criterion | Threshold |
|---|---|
| Sokolow-Lyon | S in V1 + R in V5 or V6 > 35 mm |
| Cornell | R in aVL + S in V3 > 28 mm (men) or > 20 mm (women) |
| R in aVL alone | > 11 mm |
| R in V5 or V6 | > 26 mm |
LV "strain" pattern: ST depression + T-wave inversion in I, aVL, V4-V6 (opposite direction to QRS)
- Left axis deviation commonly present
- LAE (left atrial enlargement): Notched P wave ("P mitrale") in lead II, biphasic P in V1
Bonus: Quick Reference Table
| Pattern | Rate | Rhythm | P Wave | QRS | Key Finding |
|---|---|---|---|---|---|
| NSR | 60-100 | Regular | Before every QRS | Narrow | Baseline normal |
| Sinus Tach | >100 | Regular | Before every QRS | Narrow | Treat the cause |
| AFib | Variable | Irregularly irregular | Absent/chaotic | Narrow* | "Irregularly irregular" |
| Atrial Flutter | ~150 | Regular (2:1) | Sawtooth waves | Narrow* | 300 atrial / 150 ventricular |
| 1° AVB | 60-100 | Regular | Before every QRS | Narrow | PR > 0.20s |
| 2° AVB Mobitz I | Variable | Regularly irreg. | Progressively longer PR then dropped | Narrow | Wenckebach |
| 3° AVB | ~30-60 | Regular but dissociated | March through independently | Wide or narrow | Complete dissociation |
| RBBB | Normal | Regular | Normal | Wide ≥0.12s | rSR' in V1 |
| LBBB | Normal | Regular | Normal | Wide ≥0.12s | Broad R in V5/V6, no septal Q |
| STEMI | Variable | Variable | Variable | Variable | ST elevation ≥1-2mm in contiguous leads |
| LVH | Normal | Regular | ± wide/notched | ± wide | Voltage criteria + strain pattern |
*Wide QRS with AFib/flutter if BBB or WPW present
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
- Fuster and Hurst's The Heart, 15th Edition
- Textbook of Family Medicine, 9e
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Can you summarize every ecg with visual presentation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have a rich set of textbook ECG images. Let me compile the full visual guide:
10 Common ECG Patterns - Visual Reference Guide
1. Normal Sinus Rhythm (NSR)
What to look for: Regular P before every QRS, PR 0.12-0.20s, QRS <0.12s, rate 60-100 bpm, upright P in leads I, II, aVF.
| Feature | Normal Value |
|---|---|
| Rate | 60-100 bpm |
| Rhythm | Regular |
| P waves | Upright in I, II, aVF - before every QRS |
| PR interval | 0.12-0.20 sec |
| QRS | Narrow ≤0.10 sec |
Clinical tip: This is your baseline. Every abnormal pattern is a deviation from this.
2. Sinus Tachycardia / Sinus Bradycardia
Same morphology as NSR - just the rate is different.
- Tachycardia: Rate > 100 bpm. All complexes identical to NSR. Always treat the underlying cause (pain, fever, PE, bleeding, drugs).
- Bradycardia: Rate < 50 bpm (Braunwald's defines pathologic threshold at 50 bpm). Normal P wave contour, upright in I, II, aVF. Often physiologic in athletes. Treat only if symptomatic.
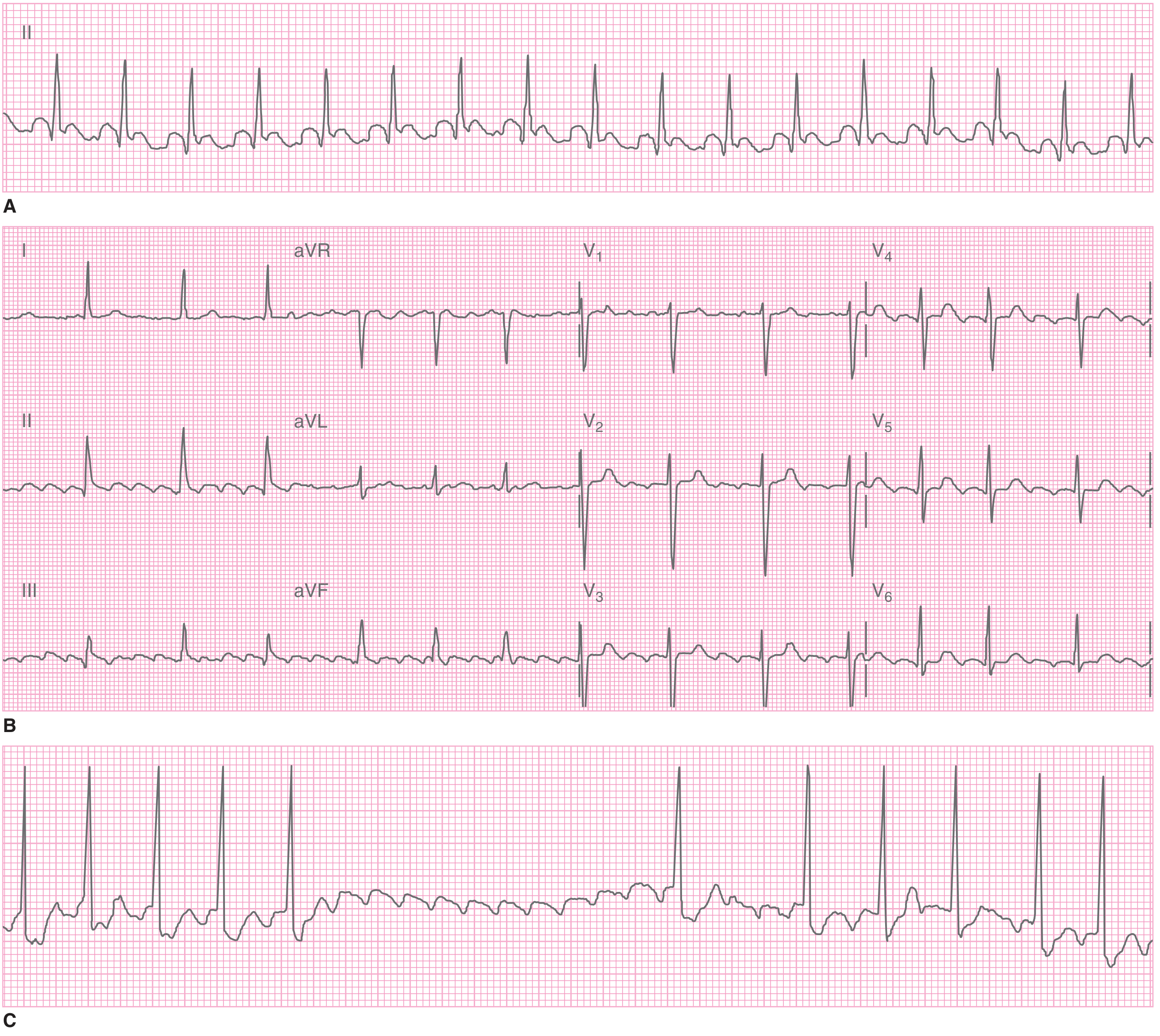
3. Atrial Fibrillation (AFib) - Three Real Examples
The three strips below show three actual patients with AFib - each looks slightly different, but all share the cardinal features:
Three examples of AFib (Tintinalli's Emergency Medicine). A. Rapid ventricular rate with chaotic baseline. B. Controlled ventricular rate, clearly irregular rhythm. C. Slower response, irregular rhythm remains.
Key features (ALL must be present):
- No P waves - replaced by chaotic fibrillatory (f) waves
- Irregularly irregular ventricular rhythm - the hallmark
- QRS narrow (unless BBB or WPW coexist)
- Atrial rate > 400-600 bpm, ventricular rate depends on AV node
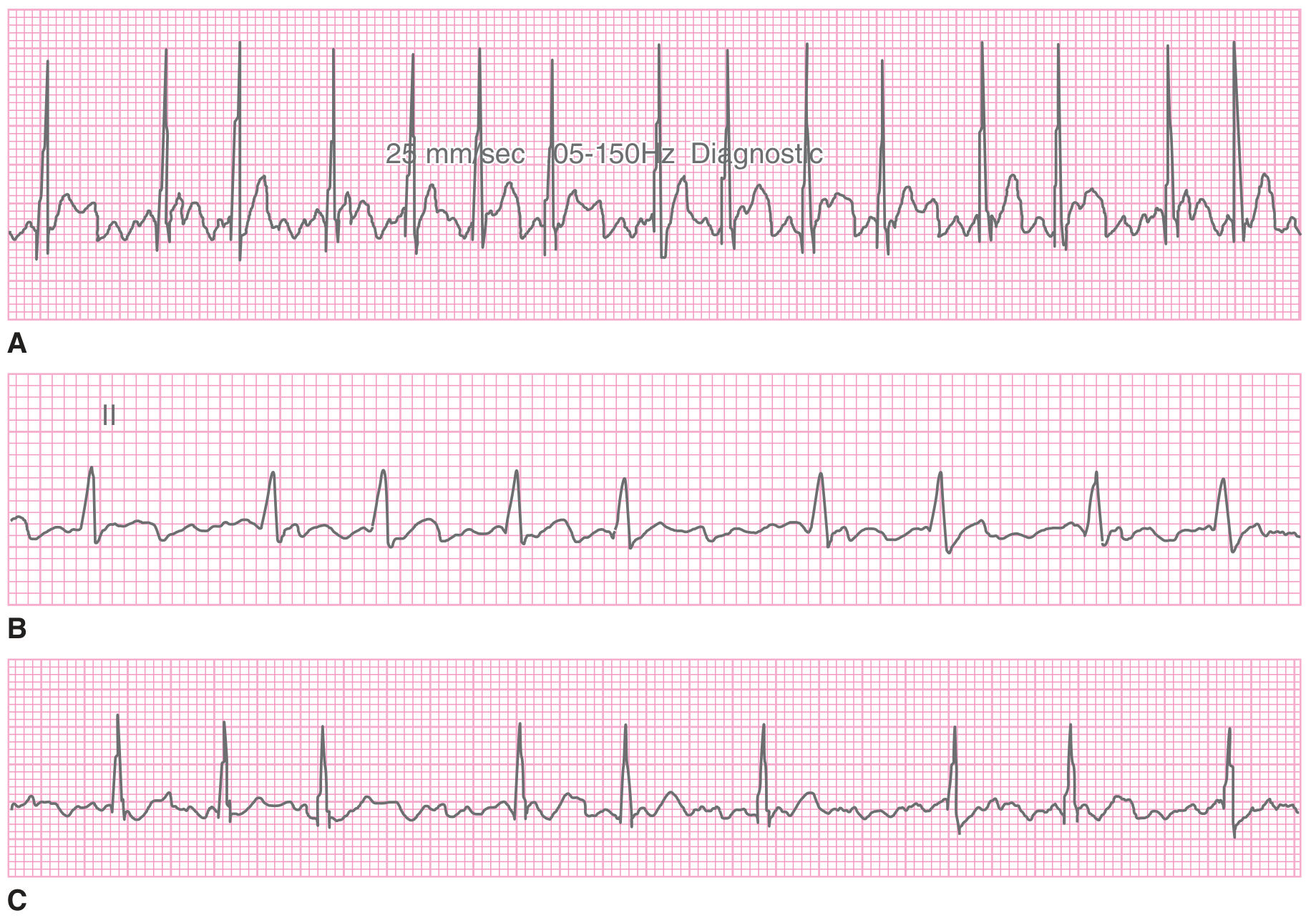
Atrial flutter (close relative): Regular "sawtooth" flutter waves at ~300 bpm, most visible in II, III, aVF and V1. Usually conducts with 2:1 block → ventricular rate ~150 bpm.
Atrial Flutter (Tintinalli's). A. Regular narrow tachycardia at 155 bpm. B. 12-lead showing sawtooth flutter waves best in II, III, aVF. C. Carotid sinus massage slows conduction and unmasks flutter waves.
4. AV Blocks
Idioventricular Escape Rhythm (seen in 3rd degree block)
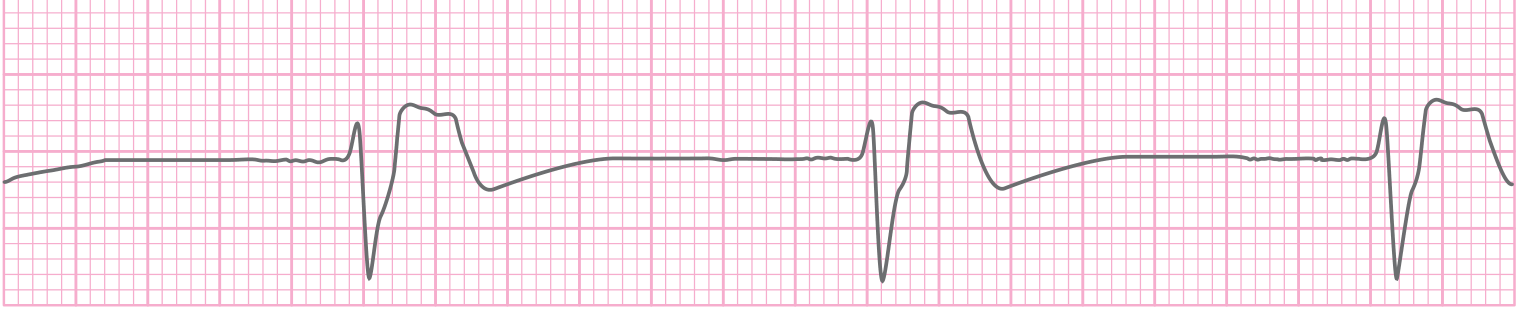
Idioventricular escape rhythm at ~30 bpm (Tintinalli's). Wide, slow QRS complexes - a ventricular escape rhythm seen in complete (3rd degree) AV block or severe bradycardia.
Summary of all AV blocks:
| Block | PR Interval | P:QRS Ratio | Key Feature | Urgency |
|---|---|---|---|---|
| 1st degree | Prolonged (>0.20s), constant | 1:1 | All P waves conduct | Benign |
| 2nd degree Mobitz I | Progressive lengthening then dropped beat | >1:1 | Wenckebach - "longer, longer, drop" | Usually benign |
| 2nd degree Mobitz II | Constant PR, then sudden non-conducted P | >1:1 | Sudden drop, no warning | Dangerous - needs pacer |
| 3rd degree (complete) | No relationship | Independent | Full AV dissociation | Emergency |
From Morgan & Mikhail's Clinical Anesthesiology: "Mobitz type II... conduction block is nearly always in or below the His bundle and frequently progresses to complete (third-degree) AV block."
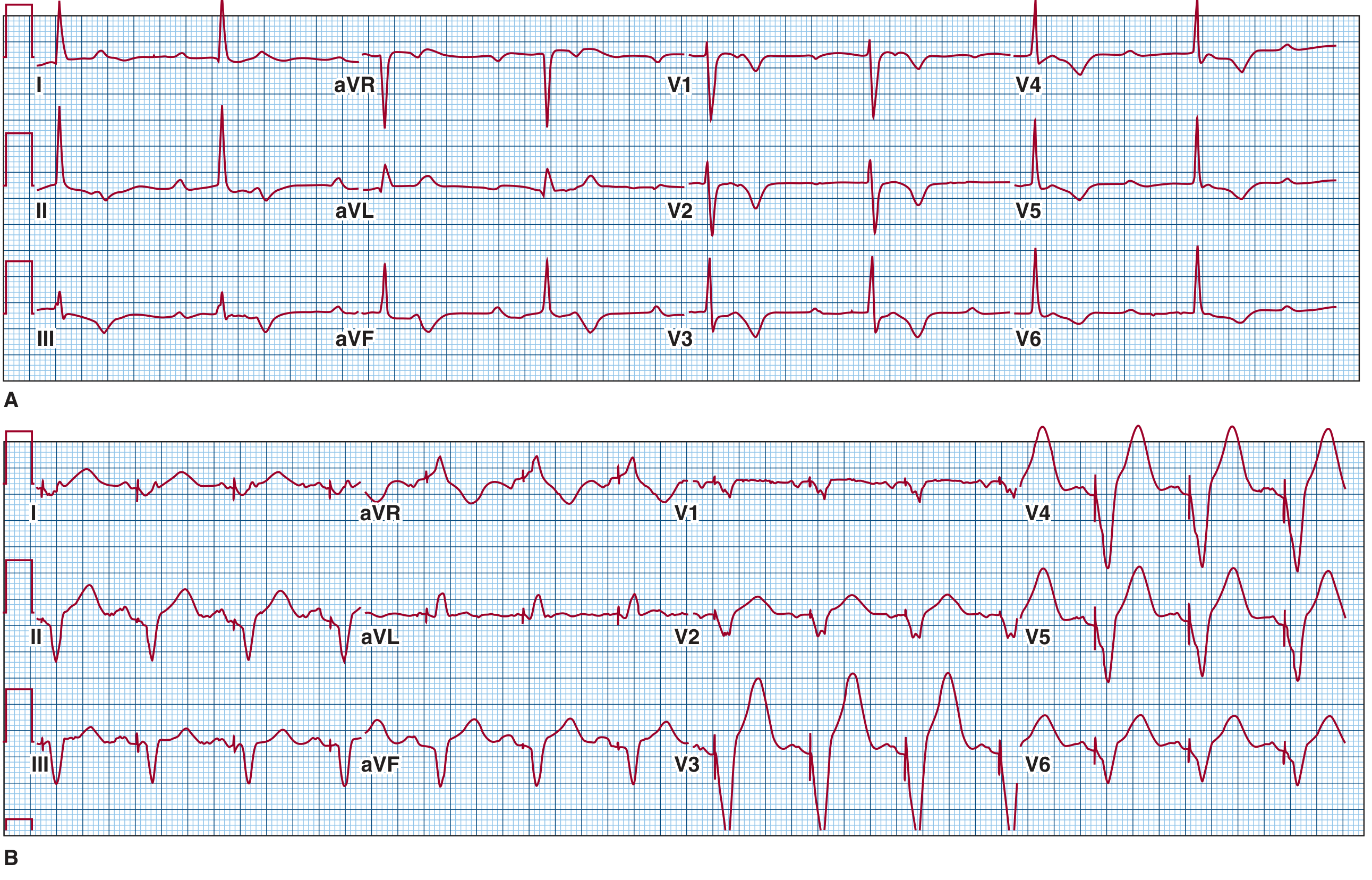
5. Right Bundle Branch Block (RBBB)
Complete AV block and paced rhythm - the ECG below shows complete AV block (Panel A) and RV pacing producing a LBBB-like pattern (Panel B):
Fuster & Hurst's The Heart - A. Complete AV nodal block: P waves march independently, slow escape rhythm. B. RV pacing: Wide QRS complexes with LBBB-like morphology (RV pacing mimics LBBB because activation starts from the right ventricle).
RBBB - Key ECG features:
- QRS ≥ 0.12 sec (wide complex)
- rSR' pattern in V1 ("rabbit ears" or M shape)
- Wide, slurred S wave in I, V5, V6
- T-wave inversion in V1-V3 (right "strain")
- Mnemonic: WiRRoW - W in V1, M in V6 for RBBB... or remember "MaRRoW" = M in V1 for RBBB
Morgan & Mikhail: "A conduction delay or block in the right bundle-branch results in a typical RBBB QRS pattern on the surface ECG (M-shape or rSR' in V1)."
6. Left Bundle Branch Block (LBBB)
LBBB - Key ECG features:
- QRS ≥ 0.12 sec (wide complex)
- Broad, deep QS or rS in V1 (W shape)
- Tall, broad, notched R in V5/V6 (M shape) - no septal Q waves in lateral leads
- Discordant ST-T changes (ST depression/T inversion OPPOSITE to main QRS direction)
- Mnemonic: WiLLiaM - W in V1, M in V6 for LBBB
Critical clinical point: New LBBB + chest pain = treat as STEMI equivalent. Apply Sgarbossa criteria to detect superimposed MI.
7. ST-Elevation Myocardial Infarction (STEMI) - Multiple Territories
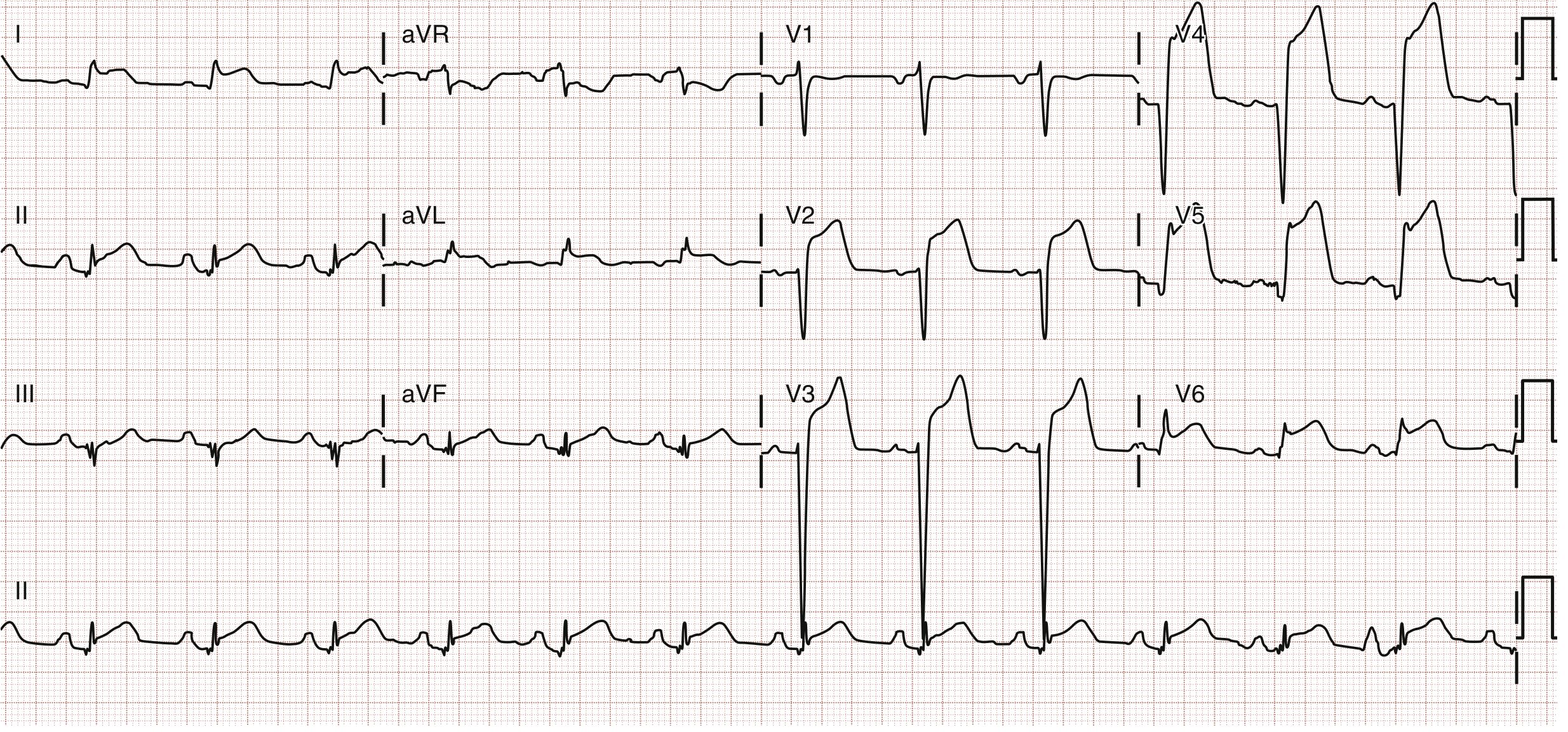
Anterior STEMI (LAD territory - V1 to V4)
Anterior wall STEMI (Rosen's Emergency Medicine). ST elevation in V1-V4, obliquely straight morphology. LAD 90% stenosis confirmed on catheterization.
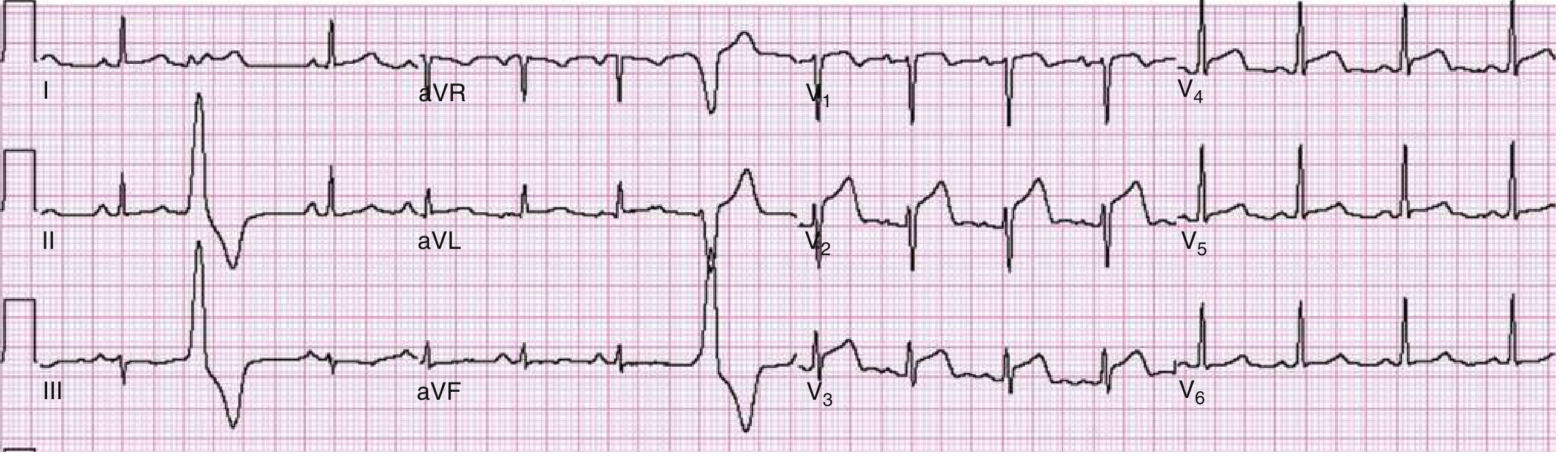
Anterolateral STEMI (LAD + LCx - V2-V6, I, aVL)
Anterolateral STEMI (Rosen's). Massive STE in V2-V6, I, aVL. Patient had prior LAD stent - emergency cath revealed 100% in-stent thrombosis.
ST Elevation in aVR = Left Main / Proximal LAD Occlusion
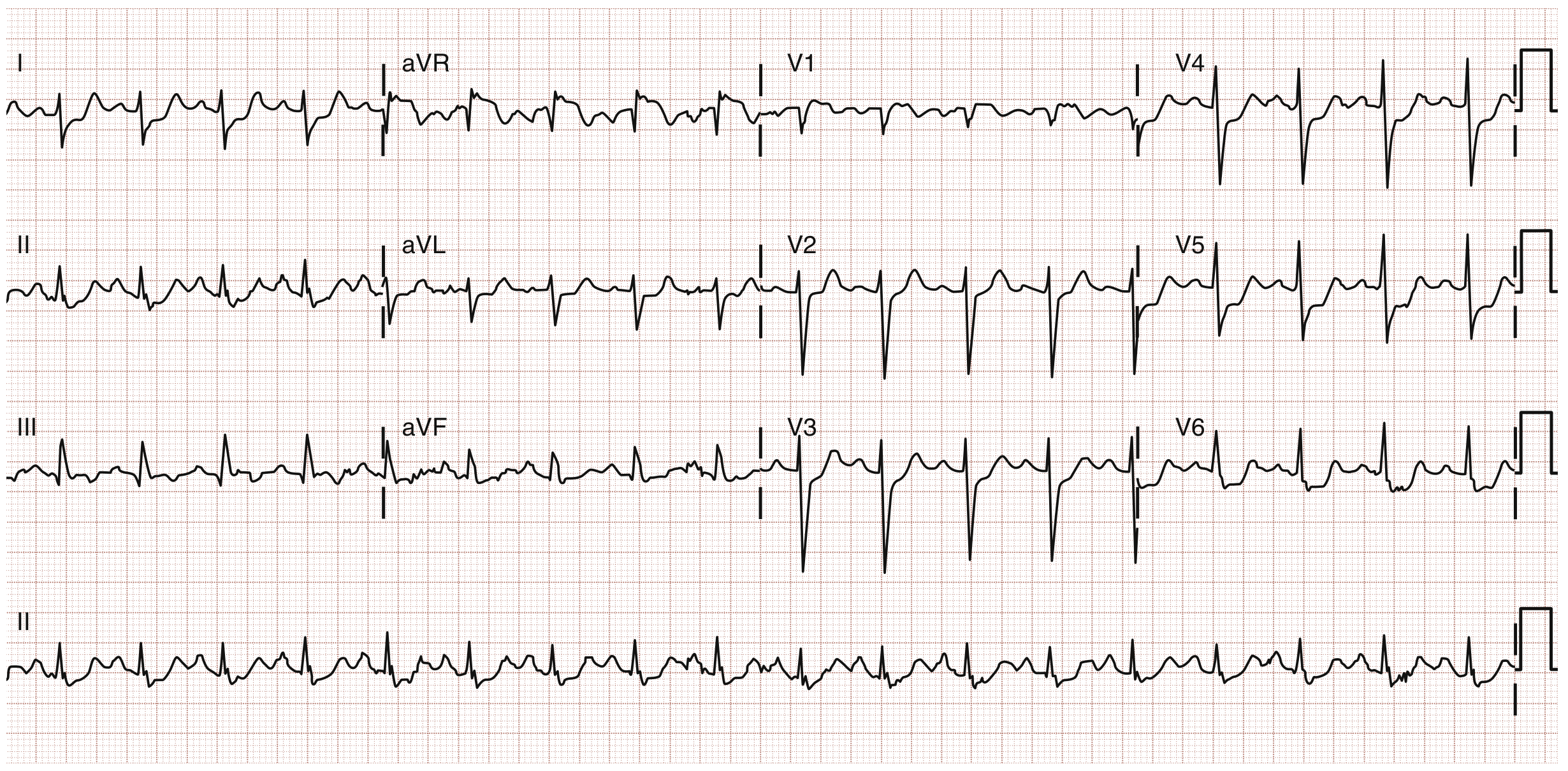
ST elevation in aVR + diffuse ST depression (Rosen's). ST elevation >1 mV in aVR plus widespread ST depression → left main coronary artery 80% stenosis found on catheterization.
Right Ventricular Infarction (Inferior STEMI + RV involvement)
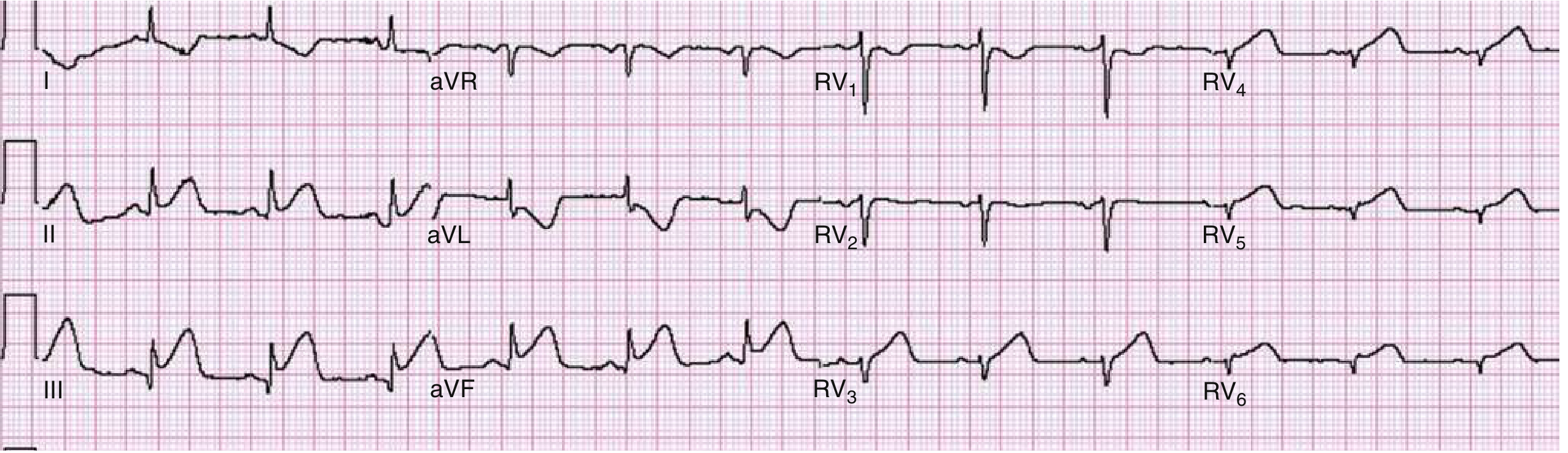
Right ventricular infarction (Rosen's). Right-sided leads (RV1-RV6). Standard limb leads show inferior STEMI (II, III, aVF) + reciprocal depression in I and aVL. Right-sided leads confirm RV infarction with STE in RV3-RV6.
STEMI territory summary from Rosen's Emergency Medicine:
| Location | Leads with STE | Artery |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Lateral | I, aVL, V5, V6 | LCx |
| Inferior | II, III, aVF | RCA |
| RV | V6R (right-sided) | Proximal RCA |
| Posterior | V8, V9 elevation; V1-V3 depression | RCA/LCx |
8. ST Depression / Ischemia Pattern (NSTEMI/Unstable Angina)
- Horizontal or downsloping ST depression ≥ 0.5 mm in ≥2 contiguous leads = subendocardial ischemia
- Symmetrical deep T inversions in precordial leads (especially V2-V3) = Wellens' syndrome (critical proximal LAD stenosis)
- De Winter T waves: Upsloping ST depression + tall peaked T waves in precordial leads = LAD occlusion without classic STE
9. Left Ventricular Hypertrophy (LVH) with Strain Pattern
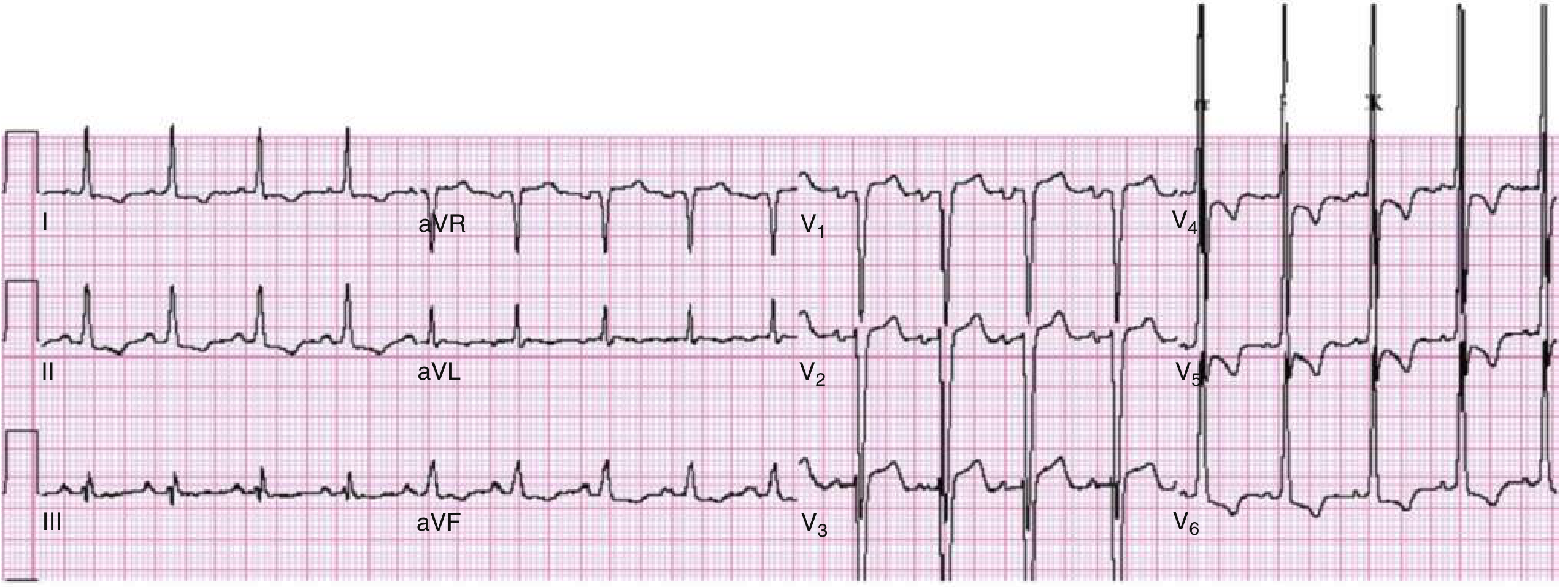
LVH with repolarization/strain pattern (Rosen's). Large amplitude R waves in V4-V6 + asymmetric T inversions (strain) in lateral leads. V1-V3 show concave ST elevation - the RIGHT precordial mirror of LV strain. This pattern is seen in ~75% of voltage-positive LVH. Do NOT confuse with ischemia.
Voltage criteria (any one is sufficient):
- S in V1 + R in V5 or V6 > 35 mm (Sokolow-Lyon)
- R in aVL > 11 mm
- Cornell criteria: R aVL + S V3 > 28 mm (men) / > 20 mm (women)
LV strain pattern: Asymmetric ST depression + T inversion in I, aVL, V4-V6 (concave morphology, opposite to QRS direction)
Common causes: Hypertension (most common), aortic stenosis, hypertrophic cardiomyopathy, coarctation of aorta.
10. Ventricular Tachycardia (VT) / Ventricular Fibrillation (VF)
VT - Key ECG features:
- Rate > 100 bpm (often 150-250 bpm)
- Wide QRS ≥ 0.12 sec - all complexes look the same (monomorphic)
- AV dissociation (P waves independent of QRS) - pathognomonic when visible
- Fusion beats and capture beats (diagnostic when present)
- Concordance in precordial leads (all positive or all negative) strongly favors VT over SVT with aberrancy
Torsades de Pointes (polymorphic VT):
- QRS complexes continuously shift axis, appearing to "twist" around the baseline
- Occurs in setting of prolonged QTc (drugs, electrolyte abnormalities, congenital LQTS)
VF - Key ECG features (from Fuster & Hurst's):
- "Rapid, irregular, dysmorphic pattern with no clearly defined QRS complex"
- Chaotic, disorganized waveforms
- No cardiac output - immediate defibrillation required
- Survival decreases 7-10% for every minute of delay in defibrillation
Quick Visual Identification Cheat Sheet
| Pattern | Rate | Rhythm | P Wave | QRS Width | Signature Finding |
|---|---|---|---|---|---|
| NSR | 60-100 | Regular | Before every QRS | Narrow | Textbook normal |
| Sinus Tach | >100 | Regular | Normal | Narrow | Fast NSR |
| Sinus Brady | <60 | Regular | Normal | Narrow | Slow NSR |
| AFib | Variable | Irregularly irregular | Absent | Narrow* | No P waves + chaos |
| A-Flutter | ~150 | Regular | Sawtooth | Narrow* | 300 atrial / 150 ventricular |
| 1° AVB | 60-100 | Regular | Normal | Narrow | PR > 0.20s |
| Mobitz I | Variable | Group beating | Progressive PR | Narrow | Wenckebach drop |
| Mobitz II | Variable | Regular then pause | Constant PR | Wide | Sudden non-conducted P |
| 3° AVB | ~30-60 | Dissociated | March through independently | Wide | Complete dissociation |
| RBBB | Normal | Regular | Normal | ≥ 0.12s | rSR' in V1 + slurred S in I/V6 |
| LBBB | Normal | Regular | Normal | ≥ 0.12s | Broad R in V5/V6, no septal Q |
| STEMI | Variable | Variable | Variable | Variable | STE ≥ 1-2 mm in contiguous leads |
| NSTEMI/UA | Variable | Variable | Variable | Narrow | ST depression / T inversions |
| LVH | 60-100 | Regular | ± wide/notched | Narrow-wide | Voltage criteria + lateral strain |
| VT | 150-250 | Regular (wide) | Dissociated | Wide | Wide complex tachycardia + AV dissociation |
| VF | - | Chaotic | None | None | No QRS - immediate shock |
*Narrow unless BBB or WPW coexist
Sources: Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, Fuster & Hurst's The Heart 15th Ed, Braunwald's Heart Disease, Morgan & Mikhail's Clinical Anesthesiology
This is a shared conversation. Sign in to Orris to start your own chat.