Simple Mastoidectomy in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
simple mastoidectomy cortical mastoidectomy surgical technique steps indications
search_medical_text
mastoidectomy anatomy mastoid air cells MacEwen triangle surgical landmarks complications
search_medical_image
simple mastoidectomy surgical diagram cortical mastoidectomy anatomy
GradeResponse
GradeResponse
GradeResponse
search_medical_text
acute mastoiditis coalescent mastoiditis surgical treatment cortical mastoidectomy Schwartze operation
search_medical_text
mastoid surgery postauricular incision Körner's septum tegmen sigmoid sinus facial nerve
search_medical_image
mastoid antrum MacEwen triangle surgical anatomy lateral semicircular canal tegmen sigmoid sinus
GradeResponse
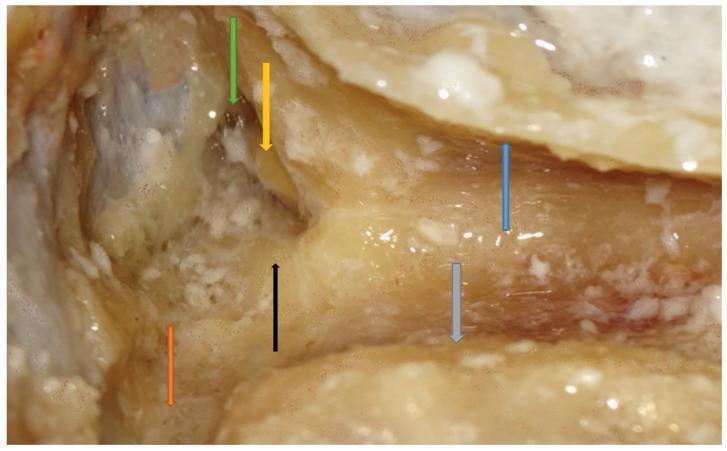
Figure 1: Intraoperative surgical photograph of right cortical (simple) mastoidectomy. The mastoid antrum is opened (green arrow), with the lateral semicircular canal prominence (black arrow) serving as the critical depth landmark, the incus short process visible (yellow arrow), middle cranial fossa dura superiorly (white membrane), sinodural angle (orange arrow), sigmoid sinus (grey arrow), and the preserved posterior canal wall (blue arrow).
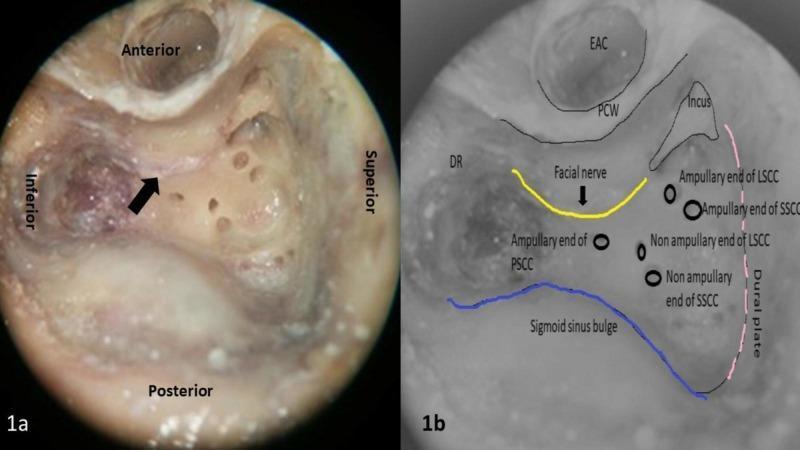
Figure 2: Left temporal bone surgical anatomy. (1a) Intraoperative field showing facial nerve (black arrow) in posterior canal wall. (1b) Annotated overlay: facial nerve (yellow), sigmoid sinus (blue), tegmen/dural plate (pink dotted), EAC, PCW, digastric ridge (DR), lateral (LSCC), posterior (PSCC) and superior (SSCC) semicircular canals.
11. FLOW CHARTS
FLOWCHART 1: Indications and Pathway to Simple Mastoidectomy
ACUTE OTITIS MEDIA
│
┌───────────┴───────────┐
No complications Complications develop
│ │
Antibiotics ASSESS TYPE
(resolves) │ │
Mastoiditis Intracranial
│ complications
┌────────────┤
Responds to Coalescent/
antibiotics Subperiosteal
│ abscess formed
Observe │
SIMPLE MASTOIDECTOMY
+ IV Antibiotics
│
┌─────────────┼─────────────┐
Resolves Persists: check Chol-
(cure) for cholesteatoma esteatoma
│ → Modified
Re-evaluate Radical /
Canal wall
down
FLOWCHART 2: Surgical Steps — Simple Mastoidectomy
┌─────────────────────────────────────────────────┐
│ PRE-OPERATIVE PREPARATION │
│ (Consent, GA, positioning, monitoring) │
└──────────────────┬──────────────────────────────┘
↓
┌─────────────────────────────────────────────────┐
│ POSTAURICULAR INCISION │
│ (1 cm posterior to postauricular sulcus) │
└──────────────────┬──────────────────────────────┘
↓
┌─────────────────────────────────────────────────┐
│ PERIOSTEAL ELEVATION │
│ Expose mastoid cortex, MacEwen's triangle, │
│ posterior EAC, temporal line, mastoid tip │
└──────────────────┬──────────────────────────────┘
↓
┌─────────────────────────────────────────────────┐
│ CORTEX REMOVAL │
│ Large cutting burr → MacEwen's triangle │
│ (Saucerization — wide approach) │
└──────────────────┬──────────────────────────────┘
↓
┌─────────────────────────────────────────────────┐
│ IDENTIFY ANTRUM │
│ Follow temporal line → Tegmen │
│ Blue-line lateral semicircular canal (LSCC) │
│ Antrum lies anterosuperior to LSCC │
│ Verify communication with aditus │
└──────────────────┬──────────────────────────────┘
↓
┌─────────────────────────────────────────────────┐
│ EXENTERATE ALL MASTOID AIR CELLS │
│ Tip, tegmental, retrofacial, perilabyrinthine, │
│ sinus, periantral cells │
└──────────────────┬──────────────────────────────┘
↓
┌─────────────────────────────────────────────────┐
│ FINAL CHECK │
│ Tegmen intact? Sigmoid exposed safely? │
│ LSCC preserved? PCW intact? Aditus open? │
│ Facial nerve safe? No cholesteatoma missed? │
└──────────────────┬──────────────────────────────┘
↓
┌─────────────────────────────────────────────────┐
│ WOUND CLOSURE │
│ Haemostasis → drain (if infected) → │
│ periosteum → subcutaneous → skin sutures → │
│ pressure dressing │
└─────────────────────────────────────────────────┘
FLOWCHART 3: Complications — Recognition and Management
INTRAOPERATIVE COMPLICATIONS
│
├── Facial nerve injury
│ → Immediate nerve monitoring alert
│ → Stop drilling, identify nerve
│ → If cut: immediate repair/grafting
│
├── Sigmoid sinus tear
│ → Pressure with Gelfoam/Surgicel
│ → Bone wax over sinus
│
├── Dural tear / CSF leak
│ → Pack with fat graft/temporalis fascia
│ → Neurosurgery consult if severe
│
└── Entry into semicircular canal
→ Immediate stop, avoid suction
→ Pack with fat (SHL inevitable)
POST-OPERATIVE COMPLICATIONS
│
├── Wound infection → Antibiotics, drain
├── Facial paresis → Steroids, monitoring
├── Sensorineural hearing loss → Evaluate PTA
├── CSF otorrhea → Conservative/surgical repair
└── Recurrent/residual disease → Re-exploration
12. COMPLICATIONS
Intraoperative
| Complication | Cause | Management |
|---|---|---|
| Facial nerve injury | Over-drilling near second genu or vertical segment | Immediate nerve decompression; primary repair or nerve grafting |
| Dural injury / CSF leak | Excessive drilling over tegmen | Fat/fascia packing; lumbar drainage; neurosurgical consult |
| Sigmoid sinus injury | Drilling over posterior mastoid | Pressure with Surgicel/Gelfoam; bone wax; rarely ligation |
| Injury to lateral semicircular canal | Drilling too medially | Immediate stop; fat plug; permanent SNHL |
| Injury to dural sinuses → air embolism | Air entry into open sinus | Pack, left lateral decubitus, aspire via central line |
Early Post-operative
- Wound infection and hematoma
- Post-operative facial palsy (usually neuropraxia → steroids)
- Vertigo (labyrinthine irritation)
- Tinnitus
Late Post-operative
- Recurrent mastoiditis
- Persistent otorrhea
- Sensorineural hearing loss (SNHL)
- Meningitis
- Residual/recurrent cholesteatoma (if combined with tympanoplasty)
- Keloid scar
13. POST-OPERATIVE CARE
| Period | Management |
|---|---|
| Immediate | Monitor vital signs, facial nerve function, ear discharge |
| Day 1–2 | IV antibiotics (continued for 5–7 days); pressure dressing change |
| Day 3–5 | Drain removal (if placed); oral antibiotics |
| 2 weeks | Suture removal; ear packing removed; ear toilet |
| 6 weeks | PTA reassessment; healing check |
| 3–6 months | Full audiological assessment |
- Ear drops: Topical antibiotic + steroid drops post-operatively
- Avoid water entry for 6 weeks
- Avoid nose blowing for 2 weeks
14. DIFFERENCES: SIMPLE vs. MODIFIED RADICAL vs. RADICAL MASTOIDECTOMY
| Feature | Simple Mastoidectomy | Modified Radical | Radical |
|---|---|---|---|
| Canal wall | Preserved | Removed | Removed |
| Middle ear | Untouched | Partly preserved | Obliterated |
| Ossicles | Preserved | Some preserved | All removed |
| TM | Preserved | Reconstructed | Absent |
| Cavity | Communicates only through aditus | Open exteriorized | Open exteriorized |
| Indication | Acute mastoiditis, COM-safe | COM-unsafe with hearing | COM-unsafe, no hearing |
| Eponym | Schwartze operation | Bondy's operation | Heath's/Stacke's |
15. MODIFICATIONS AND RELATED PROCEDURES
15.1 Combined Approach Tympanoplasty (CAT)
(Jansen 1958, Portmann & Chabrol)
- Simple mastoidectomy + posterior tympanotomy + tympanoplasty
- Canal wall up (CWU) technique
- Preserves EAC anatomy while clearing mastoid disease
- Two-stage procedure often needed to detect residual cholesteatoma
15.2 Posterior Tympanotomy
- Extension of simple mastoidectomy
- Opens facial recess (between facial nerve, chorda tympani, and EAC)
- Access for cochlear implant insertion
- Access for posterior tympanum
15.3 Endolymphatic Sac Surgery (Decompression/Shunt)
- Simple mastoidectomy is the approach
- Indicated in Meniere's disease refractory to medical treatment
16. RECENT ADVANCES (RGUHS-Relevant)
16.1 Endoscopic-Assisted Mastoidectomy
- Combines microscopic mastoidectomy with endoscopic visualization of difficult corners
- Better illumination of sinus tympani, facial recess, and protympanum
- Reduces need for canal wall down in selected cases
- (El-Anwar et al., 2015; Bennett et al., 2016)
16.2 Image-Guided Surgery (Navigation)
- CT/MRI-based intraoperative navigation
- Reduces risk to facial nerve and sigmoid sinus
- Especially useful in revision surgery and obliterated mastoids
- Medtronic NIM-Response® and Stryker Navigation systems in common use
16.3 Intraoperative Facial Nerve Monitoring
- Continuous EMG-based monitoring (NIM-3 system)
- Significantly reduces incidence of permanent facial nerve injury
- Now considered standard of care in mastoid surgery (AAO-HNS Guidelines)
16.4 Powered Irrigation Systems
- Constant saline irrigation integrated with drill (Medtronic Midas Rex)
- Prevents thermal injury to labyrinth and nerve
- Reduces bone dust and improves visualization
16.5 Laser-Assisted Mastoidectomy
- CO₂ or KTP laser for precise bone removal near critical structures
- Useful near facial nerve and semicircular canals
- Limited by cost and availability (Jovanovic et al., 2004)
16.6 Robotic Mastoidectomy
- Robotic drill systems with pre-programmed CT-guided trajectories
- Achieves sub-millimeter accuracy
- Prototype systems (RobOtol®, Helix Otosurgery Robot) in clinical trials
- (Williamson et al., 2015; Labadie et al., 2012)
16.7 3D Temporal Bone Simulation & Training
- Virtual reality mastoidectomy simulators (Voxel-Man® TempoSurg)
- Allows resident training without patient risk
- Validated tool for competency assessment (Alrwaily et al., 2017)
16.8 Piezoelectric Bone Surgery (Piezosurgery)
- Ultrasonic bone cutting devices
- Selective — cuts bone but spares soft tissue (nerves, dura, vessels)
- Applications in difficult mastoid dissections (Schlee et al., 2014)
17. TEXTBOOK PERSPECTIVES SUMMARY
| Textbook | Key Emphasis on Simple Mastoidectomy |
|---|---|
| Scott Brown (8th ed.) | Detailed surgical anatomy; MacEwen's triangle; step-by-step technique; complications |
| Cummings (7th ed.) | Indications, combined approach tympanoplasty, cochlear implant access, intraoperative monitoring |
| Stell & Maran | Classic surgical technique; periosteal approach; saucerization principles |
| Zakir Hussain | Indications in acute mastoiditis; Bezold's abscess; post-operative care; complications |
| Dhingra (7th ed.) | Clear concise surgical steps; types of mastoidectomy comparison; complications table |
| Hazarika | Emphasis on Indian surgical practice; acute coalescent mastoiditis; CSOM approach |
18. MNEMONIC AIDS
Landmarks of Mastoid Surgery — "TSLFD"
- Tegmen = roof
- Sigmoid sinus = posterior
- Lateral semicircular canal = medial guide
- Facial nerve = medial danger
- Digastric ridge = inferior
Air cell groups — "S-T-R-P-T-P"
- Sinus tip
- Tegmental
- Retrofacial
- Perilabyrinthine
- Tip
- Periantral
19. VIVA/EXAM POINTS (RGUHS Focus)
- Schwartze's operation = Simple/Cortical mastoidectomy (1873)
- MacEwen's triangle is the surface marking of the mastoid antrum
- Körner's septum = petrosquamous suture; surgical pitfall
- Antrum is 1.5–2 cm deep to the surface in adults; just 1.25 cm at birth
- Lateral semicircular canal = single most important surgical landmark
- Posterior canal wall is PRESERVED in simple mastoidectomy — key difference from radical
- Three dangerous structures: Dura (tegmen), Sigmoid sinus, Facial nerve
- Sclerotic mastoid = most difficult type to operate on
- Bezold's abscess = pus tracking below digastric muscle into neck → mastoidectomy + drainage
- Minimum 48–72 hours of IV antibiotics before declaring failure and proceeding to surgery
20. SUMMARY TABLE
| Aspect | Detail |
|---|---|
| Eponym | Schwartze operation (1873) |
| Incision | Postauricular, 0.5–1 cm behind crease |
| Approach | MacEwen's triangle, periosteal elevation |
| Key landmark | Lateral semicircular canal (blue-line) |
| Antrum depth | 1.5–2 cm in adults; 1.25 cm at birth |
| Preserved structures | Posterior canal wall, ossicles, TM, middle ear |
| Exenterated | All mastoid air cells |
| Boundaries | Tegmen (sup), sigmoid (post), PCW (ant), LSCC (med), digastric (inf) |
| Anaesthesia | GA preferred; hypotensive technique |
| Complications | Facial palsy, CSF leak, SNHL, sinus injury |
| Recent advance | Navigation, endoscopy, robotic, piezoelectric |
References
- Scott Brown's Otorhinolaryngology, Head & Neck Surgery, 8th Edition — Chapter on Mastoid Surgery
- Cummings Otolaryngology: Head and Neck Surgery, 7th Edition — Chapter 139 (Mastoid Surgery)
- Stell and Maran's Head and Neck Surgery — Temporal Bone Section
- Zakir Hussain — Textbook of ENT & Head and Neck Surgery
- Dhingra PL — Diseases of Ear, Nose & Throat, 7th Edition
- Hazarika P — Textbook of Ear, Nose & Throat, 4th Edition
- Bailey & Love's Short Practice of Surgery, 28th Edition, p. 774
- Williamson RA et al. — "Robotic mastoidectomy" — Laryngoscope, 2015
- El-Anwar MW et al. — "Endoscope-assisted cortical mastoidectomy" — Eur Arch ORL, 2015
- AAO-HNS Clinical Practice Guidelines — Tympanostomy Tubes & Mastoidectomy, 2020
This answer is formatted for a 50-mark RGUHS University examination answer. For maximum marks, use headings, draw diagrams of MacEwen's triangle and the surgical steps, include flowcharts, and quote the landmark texts cited above.
This is a shared conversation. Sign in to Orris to start your own chat.