wound healing
Reading File
search_medical_text
wound healing phases mechanisms
search_medical_text
wound healing impaired chronic wound management
search_medical_image
wound healing phases diagram
GradeResponse
GradeResponse
GradeResponse
Wound Healing
Wound healing is a complex, dynamic biological process involving overlapping phases of cellular and molecular activity. In adults, it typically results in fibrosis and scar formation rather than true tissue regeneration (Bailey & Love's Surgery, p. 45).
The Four Phases
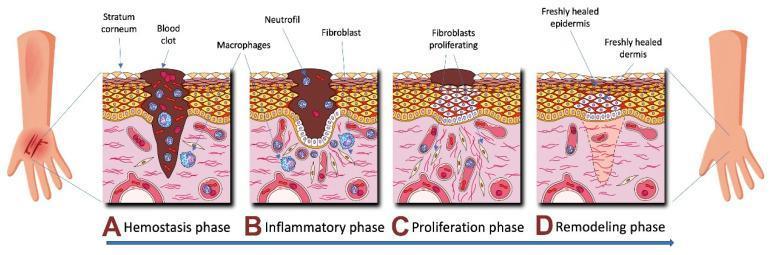
| Phase | Timing | Key Events |
|---|---|---|
| Hemostasis | Immediate (0–few hours) | Vasoconstriction, platelet aggregation, clot formation, fibrin scaffold |
| Inflammation | Days 1–4 | Neutrophil influx (debris/bacteria clearance), macrophage recruitment (growth factor release) |
| Proliferation | Days 4–21 | Fibroblast activity, collagen deposition, angiogenesis, epithelial migration, granulation tissue |
| Remodeling | Weeks to years | Collagen crosslinking and reorganization, scar maturation, wound contraction |
Phase Details
1. Hemostasis
- Damaged vessels constrict; platelets adhere and aggregate at the injury site
- Coagulation cascade activated → fibrin clot forms
- Clot acts as a scaffold and releases growth factors (PDGF, TGF-β) that recruit inflammatory cells
2. Inflammation
- Neutrophils (first 24–48 hrs): phagocytose bacteria and debris; release proteases
- Macrophages (day 2 onward): key orchestrators — release VEGF, TGF-β, IL-1, TNF-α; bridge inflammation to proliferation
- Classic signs: rubor, calor, dolor, tumor
3. Proliferation
- Fibroblasts migrate in and synthesize collagen (initially type III, later type I) and extracellular matrix
- Angiogenesis: new capillaries restore oxygen supply
- Epithelialization: keratinocytes migrate from wound edges under the scab
- Granulation tissue: pink/red vascular connective tissue fills the wound bed
4. Remodeling
- Type III collagen replaced by stronger type I collagen
- Maximum tensile strength (~80% of original) reached at ~3 months
- Myofibroblasts drive wound contraction
- Hypertrophic scars or keloids may form if remodeling is dysregulated
Types of Healing
| Type | Description | Example |
|---|---|---|
| Primary intention | Clean wound edges apposed (sutured/stapled) | Surgical incision |
| Secondary intention | Wound left open to granulate and contract | Abscess cavity |
| Tertiary intention | Delayed primary closure after initial open management | Contaminated wounds |
Chronic Wounds
Chronic wounds fail to progress through normal healing stages in a timely manner (Bailey & Love's Surgery, p. 55). Key features:
- Prolonged inflammatory phase — persistent neutrophil activity damages healthy tissue
- Persistent infection — biofilm formation common
- Elevated proteases — degrade growth factors and matrix
- Common examples: diabetic foot ulcers, venous leg ulcers, pressure injuries, arterial ulcers
Management principles:
- Treat the underlying cause (glycemic control, compression therapy, revascularization)
- Wound bed preparation (TIME framework):
- Tissue debridement (surgical, autolytic, enzymatic)
- Infection/inflammation control
- Moisture balance (appropriate dressings)
- Edge advancement (assess for non-healing epithelia)
- Advanced therapies: negative pressure wound therapy (NPWT), growth factors, skin substitutes, hyperbaric oxygen
Factors Impairing Wound Healing
| Local Factors | Systemic Factors |
|---|---|
| Infection/biofilm | Diabetes mellitus |
| Poor blood supply (ischemia) | Malnutrition (esp. vitamin C, zinc, protein) |
| Foreign body | Corticosteroids / immunosuppression |
| Radiation damage | Obesity |
| Repeated trauma | Advanced age |
| Desiccation | Renal/hepatic failure |
Fetal vs. Adult Healing
Fetal wounds (early gestation) heal without scar formation — this involves elevated hyaluronic acid, different TGF-β isoform ratios, and a more anti-inflammatory microenvironment. Understanding these differences drives regenerative medicine research aimed at scarless wound repair in adults (Bailey & Love's Surgery, p. 45).
This is a shared conversation. Sign in to Orris to start your own chat.