I want to know about pcos in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"polycystic ovary syndrome"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have very comprehensive content to write a detailed PCOS overview. Let me compile the full answer now.
Polycystic Ovary Syndrome (PCOS) - A Comprehensive Overview
PCOS is one of the most common endocrine disorders in women of reproductive age, affecting 5-10% of women worldwide. It was first described in 1935 by Stein and Leventhal as the association of amenorrhea, bilateral polycystic ovaries, and obesity. The condition receives considerable attention due to its high prevalence and wide-ranging reproductive, metabolic, and cardiovascular consequences.
1. Definition & Diagnostic Criteria
PCOS is a syndrome of ovarian dysfunction characterized by a triad of:
- Hyperandrogenism (HA) - clinical or biochemical
- Chronic anovulation / oligo-ovulation
- Polycystic ovarian (PCO) morphology on ultrasound
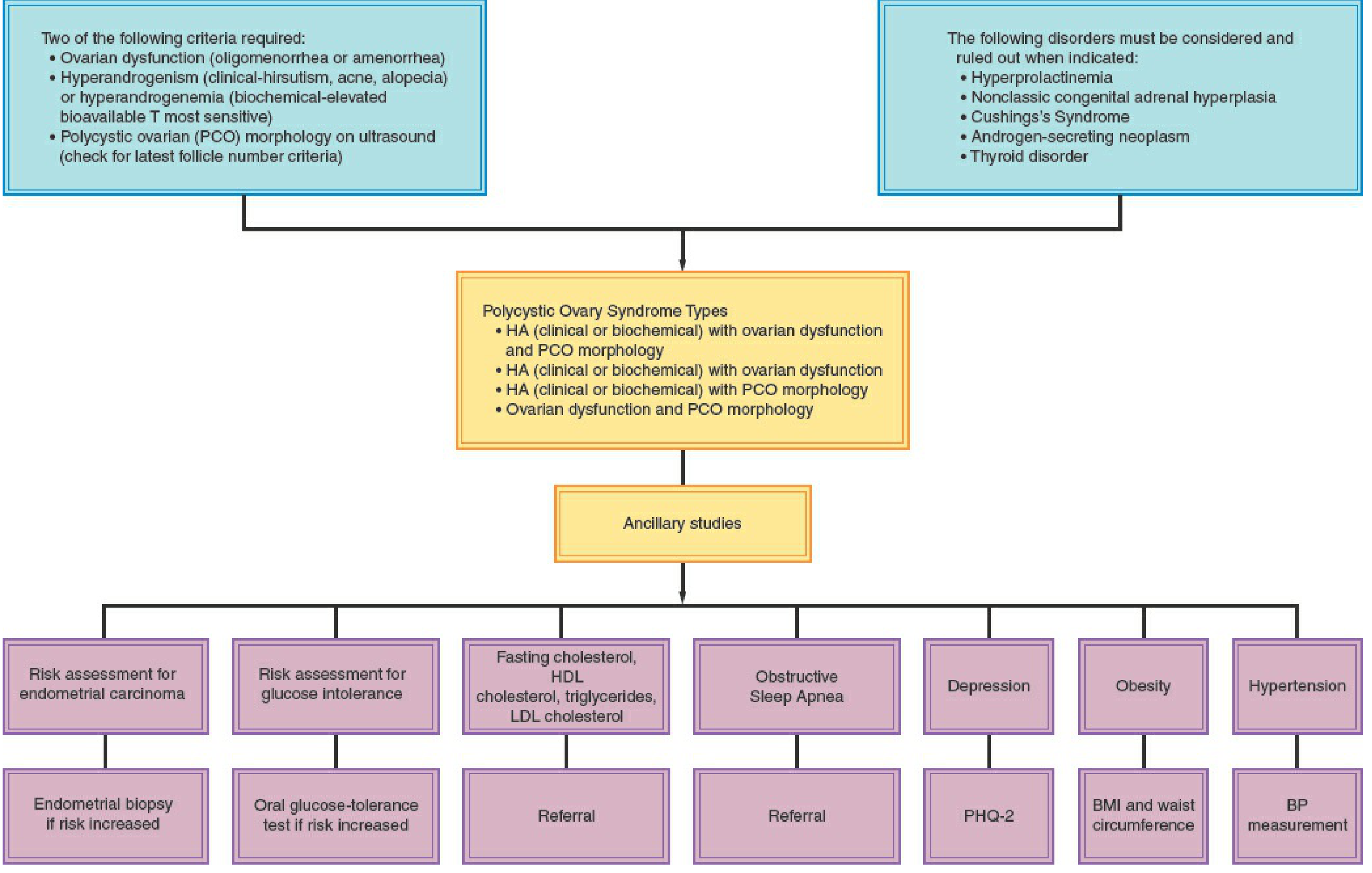
Rotterdam Criteria (2003) - Most Widely Used
Diagnosis requires 2 out of 3 of the following (after exclusion of other disorders):
| Criterion | Details |
|---|---|
| Menstrual dysfunction | Amenorrhea or oligomenorrhea |
| Hyperandrogenism | Clinical (hirsutism, acne, alopecia) or biochemical (elevated free/total testosterone) |
| PCO morphology on ultrasound | ≥20 follicles in either ovary (2-9 mm diameter) and/or ovarian volume >10 mL |
This generates 4 phenotypes:
- HA + ovarian dysfunction + PCO morphology
- HA + ovarian dysfunction
- HA + PCO morphology
- Ovarian dysfunction + PCO morphology
Important: In adolescents, diagnosis should be based on persistent anovulation AND clinical/biochemical HA - PCO morphology alone is insufficient.
The 1990 NIH criteria required both chronic anovulation AND clinical/biochemical HA, making it more restrictive than Rotterdam.
Diagnostic Algorithm
2. Etiology & Genetics
- PCOS appears to be a familial disorder inherited as a complex genetic trait - polygenic and/or multifactorial
- Many affected girls have alterations in insulin signaling
- Typically begins at or near puberty with hirsutism and irregular menses from menarche
- Obesity worsens the phenotype by increasing hyperinsulinemia
- Can also arise in adulthood coinciding with emergence of obesity
Conditions to Exclude (Differential Diagnosis)
- Hyperprolactinemia
- Nonclassic congenital adrenal hyperplasia (CAH) - measure basal 17-OHP
- Cushing's syndrome
- Androgen-secreting neoplasm
- Thyroid disorder
- Hypo/hypergonadotropic disorders
3. Pathophysiology
Hyperandrogenism and anovulation in PCOS arise from abnormalities in four endocrine compartments:
A. Ovarian Compartment (primary)
- The ovary is the most consistent contributor of excess androgens
- Dysregulation of CYP17 (the androgen-forming enzyme in both adrenals and ovaries) is a key pathogenetic mechanism
- The ovarian stroma, theca, and granulosa all contribute, stimulated by elevated LH
- Total and free testosterone levels correlate directly with LH levels
- Serum total testosterone is usually no more than twice the upper normal range (20-80 ng/dL); levels >200 ng/dL suggest ovarian hyperthecosis
B. Adrenal Compartment
- Plays a contributory role
- Hyperfunctioning CYP17 coexists in both adrenals and ovaries in PCOS
- DHEAS is elevated in some women
C. Peripheral (adipose tissue)
- Adipose tissue converts androgens to estrogens via aromatization
- Central/android obesity amplifies the hormonal dysregulation
D. Hypothalamic-Pituitary Compartment
- Elevated LH levels (in ~2/3 of cases), with relative decrease in FSH
- Elevated LH:FSH ratio (a minor, not major, diagnostic criterion)
- Increased LH pulse frequency and amplitude
Insulin Resistance Mechanism
- Insulin resistance (IR) is commonly present in PCOS
- Hyperinsulinemia stimulates ovarian androgen production
- Insulin also decreases hepatic SHBG production, increasing free androgen levels
- The hyperinsulinemia-PCOS cycle is a key driver, especially in obese women
4. Clinical Features
Reproductive Features
| Feature | Details |
|---|---|
| Hirsutism | ~70% of PCOS patients in the US; only 10-20% in Japan (due to genetic differences in skin 5α-reductase activity) |
| Acne | Common; related to androgen excess |
| Male-pattern alopecia | Androgen-mediated |
| Menstrual irregularity | Ranges from oligomenorrhea to amenorrhea; irregular from menarche |
| Anovulatory infertility | Most common cause of anovulatory infertility in developed countries |
| Primary amenorrhea | Rare; menarche may be delayed in a few cases |
Metabolic Features
- Obesity: >50% of PCOS patients; characteristically central/android distribution; higher waist-to-hip ratio indicates increased CVD and diabetes risk
- Insulin resistance and hyperinsulinemia: Very common
- Impaired glucose tolerance / Type 2 diabetes: Significantly elevated risk
- Dyslipidemia (up to 70% prevalence in US): Decreased HDL, elevated triglycerides, altered LDL
- Metabolic syndrome: Waist >88 cm + triglycerides >150 + HDL <50 + BP >130/85 + fasting glucose 110-126 mg/dL (any 3 of 5)
Ovarian Pathology
- Macroscopic: Ovaries 2-5x normal size; white thickened cortex with multiple cysts <1 cm
- Microscopic: Fibrotic and hypocellular superficial cortex, increase in follicles with luteinized theca interna, luteinized stromal cells
Cardiovascular Risks
- Impaired fibrinolysis (elevated plasminogen activator inhibitor)
- Hypertension - incidence reaches 40% by perimenopause
- Greater prevalence of atherosclerosis and cardiovascular disease
- Estimated 7-fold increased risk for myocardial infarction
Obstetric Risks (in pregnancy)
- Increased risk of: early miscarriage, gestational diabetes, gestational hypertension, preeclampsia, and preterm birth
Psychological Features
- Elevated rates of depression and anxiety
- Reduced quality of life
5. Laboratory Investigations
| Test | Finding in PCOS |
|---|---|
| LH | Elevated in ~2/3 of patients |
| LH:FSH ratio | Elevated (minor criterion) |
| Total/free testosterone | Moderately elevated |
| DHEAS | Elevated in some (adrenal contribution) |
| SHBG | Decreased (due to insulin and androgen excess) |
| 17-OHP (basal follicular phase) | Normal (elevated suggests nonclassic CAH) |
| Fasting glucose/2-hr OGTT | Screen for IGT / T2DM |
| Fasting lipid profile | Dyslipidemia common |
| AMH | Elevated; reliable predictor of antral follicle count |
| Prolactin, TSH | Normal (to exclude mimics) |
2-Hour Glucose Tolerance Test (75g OGTT):
- Normal 2-hr: <140 mg/dL
- Impaired glucose tolerance: 140-199 mg/dL
- Type 2 DM: ≥200 mg/dL
6. Treatment
Treatment goals vary based on the patient's primary concern: menstrual regulation, hirsutism/acne, fertility, or metabolic risk reduction.
A. Lifestyle Modification (all patients)
- First-line for obese women - weight loss of just 5-7% over 6 months can:
- Reduce free testosterone significantly
- Restore ovulation and fertility in >75% of women
- A 10-kg weight loss reduces insulin levels by 40% and testosterone by 35%
- Exercise reduces insulin resistance independent of weight loss
- Recommended in ALL women with PCOS
B. Not Desiring Pregnancy
Menstrual Regulation and Hyperandrogenism
| Treatment | Mechanism | Notes |
|---|---|---|
| Combined oral contraceptives (COCs) | Suppress LH → reduce ovarian androgens; estrogen → ↑ SHBG → ↓ free testosterone; reduce DHT conversion | First-line; reduces hair growth in ~2/3 of patients; use lowest effective estrogen dose |
| Spironolactone | Androgen receptor blocker; inhibits 5α-reductase | Add if inadequate response to COC after 6 months |
| Flutamide | Androgen receptor blocker | Alternative antiandrogen |
| Finasteride | 5α-reductase inhibitor | For hirsutism |
| Medroxyprogesterone acetate (10 mg for 10-14 days every 3 months) | Endometrial protection | For women who can't take estrogen |
| Levonorgestrel IUD | Endometrial protection | Alternative |
| GnRH analogues | Suppress LH and ovarian androgen production | Second-line; costly |
Metabolic Management
- Metformin: Insulin sensitizer; recommended for prevention of cardiometabolic risk in overweight/obese PCOS; reduces androgen levels by reducing hyperinsulinemia; NOT recommended alone for hyperandrogenic symptoms, endometrial protection, or infertility
- Statins: For dyslipidemia management
- GLP-1 agonists: Recent evidence supports their use in PCOS with obesity for weight loss and hormonal regulation (2024 meta-analysis, PMID 39178623)
- Probiotics/synbiotics: Emerging evidence for managing insulin resistance (2024 systematic review, PMID 39599701)
C. Desiring Fertility (Ovulation Induction)
| Agent | Role |
|---|---|
| Letrozole (aromatase inhibitor) | First-line for ovulation induction |
| Clomiphene citrate (SERM) | Second-line (with or without metformin) |
| Injectable gonadotropins | Used judiciously by experienced practitioners; PCOS increases risk of ovarian hyperstimulation syndrome (OHSS) |
| Metformin | Adjunct in obese women; insulin sensitizers may help shift endocrine balance toward ovulation |
Prepregnancy counseling and lifestyle management should be offered before attempting conception.
D. Mechanical Hair Removal
- Temporary: shaving, depilatory creams, waxing
- Permanent: laser epilation, electrolysis
7. Monitoring & Screening Schedule
All women with PCOS should be screened at diagnosis and at regular intervals for:
- Obesity (BMI + waist circumference)
- Hypertension (BP at every visit)
- Glycemic control (2-hr 75g OGTT if BMI >30, age >40, personal/family history of DM)
- Fasting lipid profile (if abnormal - follow AHA guidelines; if normal - reassess every 2 years)
- Endometrial carcinoma risk (biopsy if risk is increased)
- Depression and anxiety (PHQ-2 screening)
- Obstructive sleep apnea
- Vitamin D levels (deficiency is common)
8. Long-Term Complications
| System | Complication |
|---|---|
| Metabolic | Type 2 diabetes, metabolic syndrome |
| Cardiovascular | Hypertension (40% by perimenopause), atherosclerosis, 7x ↑ MI risk |
| Reproductive | Anovulatory infertility, endometrial cancer (from unopposed estrogen) |
| Obstetric | Miscarriage, gestational DM, preeclampsia, preterm birth |
| Psychological | Depression, anxiety, poor quality of life |
| Hepatic | NAFLD/NASH |
Recent Evidence (2024-2025)
- Lifestyle interventions remain central to PCOS management, with a 2025 systematic review (PMID 39861440) confirming their efficacy across all PCOS phenotypes
- GLP-1 receptor agonists (e.g., semaglutide, liraglutide) show promising results in PCOS with obesity, with a 2024 meta-analysis (PMID 39178623) demonstrating significant weight loss and hormonal improvement
- Probiotics and synbiotics are emerging as adjuncts for insulin resistance and hormonal imbalance management per a 2024 systematic review (PMID 39599701)
Sources: Berek & Novak's Gynecology; Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.