Retraction of nipple pathophysiology
Reading File
Finding Sources
Finding Sources
Searching PubMed
nipple retraction inversion pathophysiology
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I have all the material needed for a comprehensive answer. Here is a synthesized response:
Nipple Retraction — Pathophysiology
Nipple retraction (also called nipple inversion when complete) results from mechanical tethering of the nipple–areolar complex by shortened, fibrotic, or malignant-infiltrated structures within the breast. The underlying mechanism varies by cause, but the final common pathway is inward traction on the nipple by fibrotic or neoplastic tissue.
1. Terminology
| Term | Definition |
|---|---|
| Nipple retraction | Partial inward displacement; a single tethered duct produces a slit-like appearance |
| Nipple inversion | Complete inward displacement of the entire nipple |
| Congenital inversion | ~5% of women; usually bilateral; benign — due to failure of normal nipple eversion during breast development |
| Acquired inversion/retraction | New-onset; requires investigation for underlying pathology |
2. Benign Causes & Mechanisms
A. Duct Ectasia / Periductal Mastitis (Most Common Benign Cause)
This is the predominant benign mechanism, particularly in peri- and postmenopausal women. Two competing (possibly complementary) theories:
Haagensen's theory (ectasia-first):
- Subareolar ducts dilate and stagnate → accumulation of inspissated secretions
- Chemically irritating fatty acids leak through the duct wall into periductal tissue
- Local inflammatory reaction (lymphocytes, macrophages, plasma cells; granulomas may form)
- Chronic inflammation → periductal fibrosis
- Fibrosis foreshortens and tethers the ducts → nipple retraction
Periductal mastitis theory (inflammation-first):
- Primary periductal inflammation (associated with smoking and diabetes) weakens duct walls
- Secondary duct dilation follows
- Repeated infection cycles cause progressive scarring → retraction, subareolar masses, and occasionally chronic periareolar fistulae
Histologically: ectatic ducts filled with inspissated debris and lipid-laden macrophages, surrounded by chronic inflammation and concentric fibrosis — the fibrotic mass mimics invasive carcinoma clinically and radiologically.
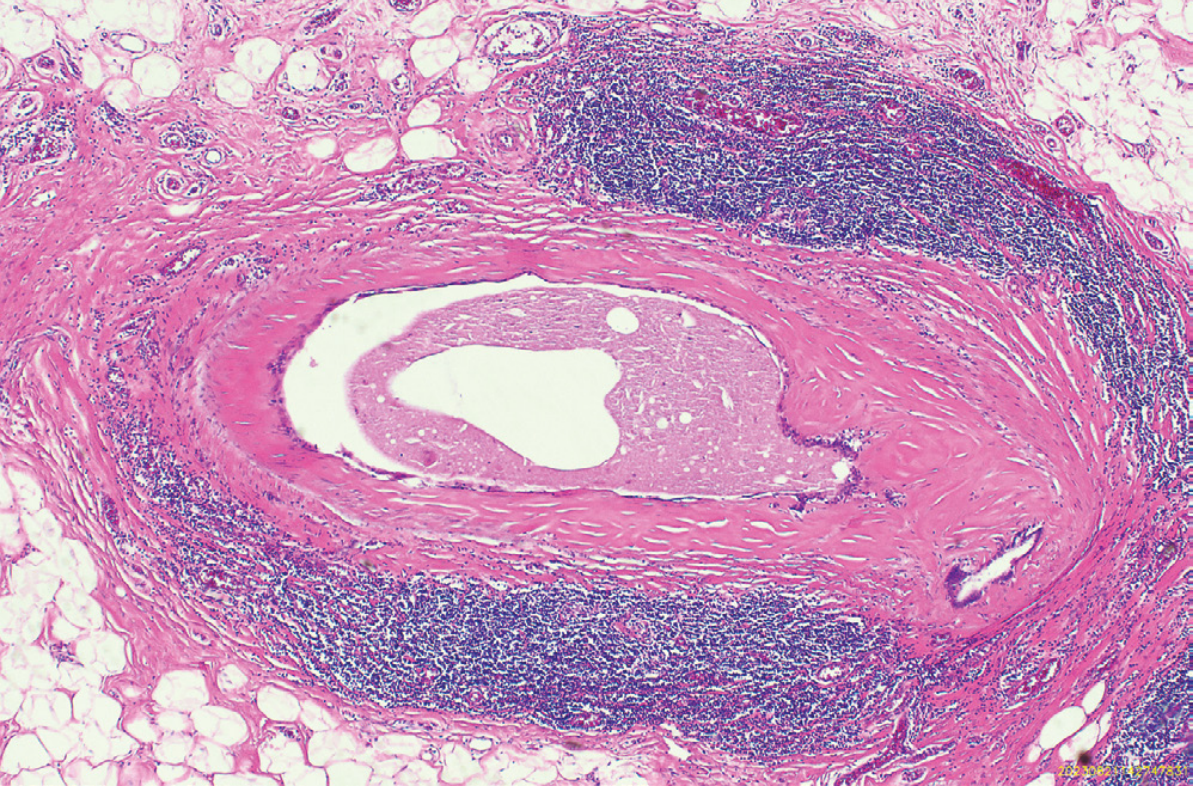
Fig. 23.4 from Robbins, Cotran & Kumar — Pathologic Basis of Disease: Duct ectasia with periductal chronic inflammation and concentric fibrosis.
B. Recurrent Subareolar Infections / Periductal Mastitis
A series of infections with resulting inflammatory changes and scarring can independently lead to retraction or inversion of the nipple, masses in the subareolar area, and occasionally a chronic fistula from the subareolar ducts to the periareolar skin. (Sabiston Textbook of Surgery)
C. Fat Necrosis
Fibrosis following liquefactive fat necrosis (from trauma or surgery) can produce skin thickening and nipple retraction as the reparative scar contracts. (Robbins & Cotran)
D. Involutional Retraction (ANDI Framework)
In the ANDI classification (Aberrations of Normal Development and Involution), nipple retraction during the involution phase (ages 35–55) is classified as a disorder of normal duct involution:
- Duct sclerosis and shortening during breast involution physically pulls the nipple inward
- Periductal fibrosis from prior episodes of periductal mastitis compounds this effect (Schwartz's Principles of Surgery)
3. Malignant Cause & Mechanism
Carcinoma
Breast carcinoma causes nipple retraction via two distinct mechanisms:
a) Direct subareolar invasion:
Carcinomas located in the subareolar area directly infiltrate and shorten the ductal and stromal elements beneath the nipple.
b) Cooper ligament traction (desmoplastic response):
Many breast carcinomas — particularly invasive ductal carcinoma — elicit a desmoplastic (scirrhous) stromal reaction: the tumor stimulates dense collagen deposition. This fibrous tissue contracts, putting Cooper ligaments under tension. Since Cooper ligaments anchor the dermis and nipple–areolar complex to the deep fascia, this traction causes:
- Skin dimpling
- Nipple retraction or flattening
These signs are best seen with indirect (angled) lighting and are accentuated by asking the patient to raise their arms above the head or contract the pectoralis muscles. (Sabiston; Mulholland & Greenfield's Surgery)
Key distinguishing feature from benign retraction: Malignant retraction is characteristically unilateral and develops over weeks to months, whereas benign duct ectasia retraction is usually bilateral and present for years.
4. Other Causes
| Cause | Mechanism |
|---|---|
| Tuberculosis of the breast | Caseating granulomatous destruction → fibrosis and ductal tethering |
| Idiopathic granulomatous mastitis | Non-necrotizing granulomatous inflammation → periductal fibrosis |
| Post-surgical/radiation | Scar contracture shortens ductal or ligamentous structures |
5. Clinical Significance
Acquired nipple retraction accounts for carcinoma in 5–20% of cases; the remainder is predominantly duct ectasia or periductal mastitis. All acquired cases require:
- Full clinical examination
- Breast ultrasound
- Mammography if age ≥35 (Berek & Novak's Gynecology)
Sources:
- Berek & Novak's Gynecology, p. 994
- Robbins, Cotran & Kumar — Pathologic Basis of Disease, Ch. 23
- Schwartz's Principles of Surgery, 11th ed., pp. 579–580
- Sabiston Textbook of Surgery, pp. 1374, 1385
- Mulholland & Greenfield's Surgery, 7th ed., p. 3876
This is a shared conversation. Sign in to Orris to start your own chat.