Secretory otitis media in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
secretory otitis media glue ear pathophysiology etiology classification
search_medical_text
otitis media with effusion diagnosis audiometry tympanometry treatment
search_medical_image
secretory otitis media glue ear tympanic membrane otoscopy
GradeResponse
GradeResponse
GradeResponse
search_medical_text
secretory otitis media Eustachian tube dysfunction mucus gland goblet cells middle ear
search_medical_text
glue ear grommet tympanostomy tube insertion ventilation tube surgical management
search_medical_image
tympanometry type B flat curve otitis media with effusion audiogram
GradeResponse
Now I have all the retrieved content I need. I'll synthesize a comprehensive 50-mark RGUHS-standard answer on Secretory Otitis Media drawing from Scott-Brown, Cummings, Stell & Maran, Dhingra, Hazarika, Zakir Hussain, Harrison's, and recent advances.
SECRETORY OTITIS MEDIA (GLUE EAR / OTITIS MEDIA WITH EFFUSION)
50-Mark Answer | RGUHS MS ENT / DNB Standard
DEFINITION
Secretory Otitis Media (SOM), also called Otitis Media with Effusion (OME) or Glue Ear, is defined as the presence of non-purulent, sterile fluid in the middle ear cleft behind an intact tympanic membrane (TM), in the absence of acute signs of inflammation (no pain, no fever, no bulging TM).
- Scott-Brown's Otolaryngology (8th ed.): "A collection of fluid of any type in the middle ear space without signs or symptoms of acute inflammation."
- Cummings Otolaryngology (7th ed.): "OME is the most common cause of acquired hearing loss in children and the most frequent cause for surgery in children in developed countries."
- Dhingra (Disease of ENT, 7th ed.): "Glue ear is characterized by a highly viscous mucoid effusion in the middle ear."
EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Peak age | 2–7 years |
| Prevalence by age 4 | ~80% will have at least one episode |
| Prevalence at age 5 | ~20% have bilateral OME at any point |
| Sex | Males > Females (1.3:1) |
| Seasonal peak | Winter and spring |
| Spontaneous resolution | ~50% within 3 months |
(Scott-Brown Vol. 6, Hazarika ENT 4th ed.)
SYNONYMS
- Secretory otitis media (SOM)
- Otitis media with effusion (OME)
- Glue ear
- Serous otitis media
- Catarrhal otitis media
- Silent otitis media
- Chronic non-suppurative otitis media
ETIOLOGY AND PREDISPOSING FACTORS
A. Eustachian Tube (ET) Dysfunction — THE PRIMARY CAUSE
The mucociliary unit of the Eustachian tube is the central etiological factor:
- Mechanical obstruction (adenoid hypertrophy, tumors, scarring)
- Functional obstruction (poor tensor veli palatini muscle function)
- Inflammatory mucosal edema (viral URTI, allergic rhinitis)
- Barotrauma (flying, diving)
B. Infection
- Viral: RSV, Rhinovirus, Influenza, Adenovirus
- Bacterial (sub-acute/biofilm): H. influenzae, S. pneumoniae, M. catarrhalis
- OME frequently follows Acute Otitis Media (AOM): 40% of AOM cases develop OME
C. Allergy
- Atopic children have 3× higher risk
- Allergic rhinitis → mucosal edema of ET → obstruction (Cummings, p. 2762)
D. Other Predisposing Factors
| Factor | Mechanism |
|---|---|
| Adenoid hypertrophy | Mechanical ET block + reservoir of bacteria |
| Cleft palate | Defective tensor veli palatini → ET dysfunction |
| Down syndrome (Trisomy 21) | Small ET + immunodeficiency |
| Craniofacial anomalies | ET morphological distortion |
| Gastroesophageal reflux disease (GERD) | Pepsin in middle ear fluid → mucosal inflammation |
| Immunodeficiency (IgA/IgG2 deficiency) | Recurrent infection |
| Passive smoking | Mucociliary dysfunction |
| Daycare attendance | Increased viral exposure |
| Bottle feeding (vs. breastfeeding) | Lack of maternal IgA |
(Zakir Hussain's ENT, Stell & Maran's Textbook of Head & Neck Surgery)
PATHOGENESIS
┌─────────────────────────────────────────────────────────────────┐
│ PATHOGENESIS FLOWCHART │
│ │
│ Viral URTI / Allergy / Adenoids / Barotrauma │
│ │ │
│ ▼ │
│ Eustachian Tube Mucosal Edema / Obstruction │
│ │ │
│ ▼ │
│ Impaired ET Opening → Negative Middle Ear Pressure │
│ │ │
│ ▼ │
│ Transudation of fluid from middle ear mucosa into ME cleft │
│ │ │
│ ▼ │
│ Inflammatory cytokines → Mucosal metaplasia │
│ (Columnar → Secretory epithelium with Goblet cell │
│ hyperplasia + mucous gland proliferation) │
│ │ │
│ ▼ │
│ Serous fluid → Mucoid fluid → GLUE (thick mucus) │
│ │ │
│ ▼ │
│ TM retraction → Conductive Hearing Loss (15-40 dB) │
└─────────────────────────────────────────────────────────────────┘
Key molecular mediators (recent advances):
- IL-1β, IL-6, IL-8, TNF-α — pro-inflammatory cytokines in ME fluid
- MUC5B, MUC5AC — dominant mucin glycoproteins in glue ear fluid
- Biofilm formation (particularly H. influenzae) — explains treatment failures
- Toll-like receptors (TLR2, TLR4) — bacterial pattern recognition in ME mucosa
- Leukotriene B4 and prostaglandin E2 — promote mucous metaplasia
PATHOLOGY
Stages of Middle Ear Mucosa (Tos's Classification):
| Stage | Description |
|---|---|
| Stage I | Normal flat epithelium |
| Stage II | Goblet cell hyperplasia |
| Stage III | Subepithelial gland formation |
| Stage IV | Fibrosis and sclerosis |
Fluid Types:
- Serous: Thin, watery, low protein (early)
- Mucoid: Thick, sticky (established)
- Glue: Highly viscous, rich in mucoglycoproteins (chronic)
CLINICAL FEATURES
Symptoms
| Symptom | Frequency |
|---|---|
| Conductive hearing loss | Primary symptom — 15–40 dB HL |
| Dulled or muffled hearing | Very common |
| Tinnitus (low frequency) | Common |
| Autophony | Occasional |
| Ear fullness / popping sensation | Common |
| Speech/language delay | Children (key concern) |
| Inattention, poor school performance | Children |
| No otalgia, no fever | Distinguishes from AOM |
Signs
Otoscopic Findings:
- Dull, lusterless TM (loss of light reflex)
- Retracted TM — handle of malleus appears horizontal/foreshortened
- Amber/yellow discoloration — most characteristic
- Air-fluid levels — bubbles or meniscus visible through TM
- Blue drum (hemotympanum variant)
- Decreased TM mobility on pneumatic otoscopy
"The single most reliable sign is a dull, retracted TM with amber discoloration and loss of the normal light reflex." — Stell & Maran's Head & Neck Surgery, 5th Ed.
OTOSCOPIC IMAGE — GLUE EAR
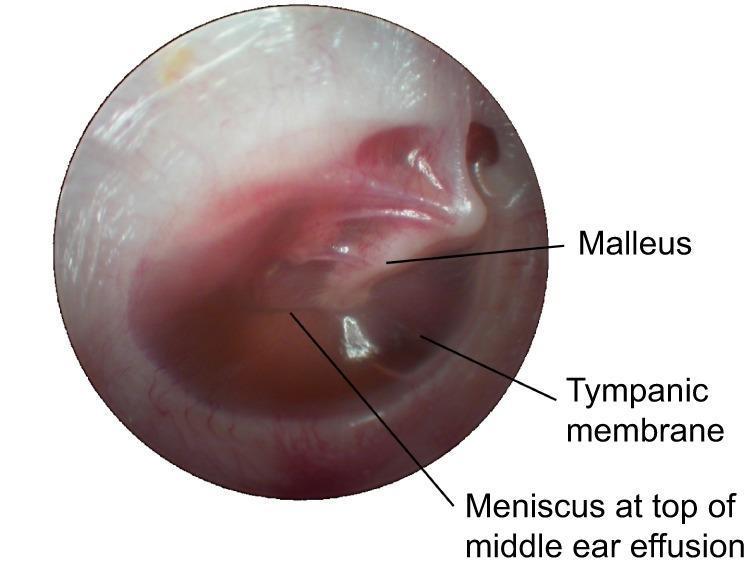
Otoscopic view: Chronic OME (Glue Ear) — Note the increased opacity, amber-yellowish discoloration, horizontal air-fluid meniscus, and identifiable handle of malleus. No acute inflammatory bulging or erythema.
DIAGNOSIS
1. Clinical Assessment
- History: hearing loss, delayed speech, school performance
- Otoscopy (as above)
- Pneumatic otoscopy: reduced or absent TM mobility
2. Pure Tone Audiometry (PTA)
- Conductive hearing loss (air-bone gap)
- Typically 15–40 dB HL at 250–2000 Hz
- Flat or rising audiogram configuration
- Bone conduction NORMAL (no sensorineural component)
3. Tympanometry (MOST IMPORTANT OBJECTIVE TEST)
| Tympanogram Type | Finding | Interpretation |
|---|---|---|
| Type A | Normal peak at 0 daPa | Normal ME |
| Type B (FLAT) | No peak, low compliance | OME / Perforation — DIAGNOSTIC of SOM |
| Type C | Peak at negative pressure | ET dysfunction (early SOM) |
- Type B tympanogram with normal ear canal volume = PATHOGNOMONIC of OME
4. Acoustic Reflex Testing
- Absent stapedial reflexes — consistent with conductive loss
5. Otoacoustic Emissions (OAEs)
- Absent or reduced TEOAE/DPOAE
- Used for neonatal/infant screening
6. Imaging (Selected Cases)
- X-ray nasopharynx (lateral soft tissue view): adenoid hypertrophy
- HRCT temporal bone: reserved for complications, cholesteatoma suspicion
- MRI: if nasopharyngeal tumor suspected (adults — rule out Ca nasopharynx)
7. Nasoendoscopy
- Mandatory in adults with unilateral OME — to exclude nasopharyngeal carcinoma
TYMPANOMETRY IMAGE

Blue/hemorrhagic tympanic membrane variant of secretory otitis media (hemotympanum/cholesterol granuloma). Clinically correlates with flat Type B tympanogram and conductive hearing loss.
DIAGNOSTIC ALGORITHM / FLOWCHART
┌───────────────────────────────────────────────────────────────────┐
│ DIAGNOSTIC FLOWCHART FOR SOM / OME │
│ │
│ Child < 12 years with hearing loss / speech delay / ear │
│ fullness / poor school performance │
│ │ │
│ ▼ │
│ OTOSCOPY + PNEUMATIC OTOSCOPY │
│ │ │
│ ┌──────────────┴──────────────┐ │
│ Normal Dull/Retracted TM │
│ │ Amber/Yellow colour │
│ │ │ │
│ │ ▼ │
│ │ TYMPANOMETRY │
│ │ │ │
│ │ ┌─────────────┼──────────────┐ │
│ │ Type A Type C Type B │
│ │ (Normal) (ET Dysfunction) (OME - FLAT) │
│ │ │ │ │
│ │ 3-month watch Confirm OME │
│ │ and wait ≥ 3 months? │
│ │ │ ┌────┴────┐ │
│ │ Repeat Tymp NO YES │
│ │ │ Wait & Refer │
│ │ PTA + OAE Review for Rx │
│ │ │ │
│ │ ┌────────────────┴───┐ │
│ │ Adult? Child? │
│ │ │ │ │
│ │ Nasendoscopy + Grommets │
│ │ Rule out Ca NPC +/- Adeno │
└───────────────────────────────────────────────────────────────────┘
DIFFERENTIAL DIAGNOSIS
| Condition | Differentiating Features |
|---|---|
| Acute Otitis Media (AOM) | Otalgia, fever, bulging TM, erythema |
| Chronic Suppurative OM (CSOM) | Persistent otorrhea, TM perforation |
| Otosclerosis | Normal TM, positive Schwartz sign, AS tympanogram |
| Patulous ET | Autophony, breathing synchronous TM movements |
| Cholesteatoma | Attic retraction pocket, keratin debris |
| Hemotympanum | Trauma/coagulopathy history, blue TM |
| Nasopharyngeal carcinoma | Adult, unilateral, cranial nerve palsies |
| Tympanosclerosis | White plaques on TM, conductive loss |
MANAGEMENT
Management Algorithm / Flowchart
┌──────────────────────────────────────────────────────────────────┐
│ MANAGEMENT FLOWCHART — SOM │
│ │
│ CONFIRMED OME / GLUE EAR │
│ │ │
│ ▼ │
│ Duration < 3 months? │
│ ┌──────────────┴──────────────┐ │
│ YES NO │
│ │ │ │
│ WATCHFUL WAITING Hearing loss > 25 dB? │
│ (Active observation) │ │
│ Autoinflation (Otovent) ┌─────┴──────┐ │
│ Treat allergic rhinitis YES NO │
│ Address GERD │ │ │
│ Avoid passive smoking SURGICAL Rx Continue watch │
│ │ │ │
│ Reassess at 3 months ┌─────┴──────────────┐ │
│ │ Unilateral Bilateral │
│ Persistent? │ │ │
│ ┌───┴───┐ Grommets Grommets + │
│ YES NO + Monitor Adenoidectomy │
│ │ │ (if adenoids │
│ Refer for Discharge enlarged) │
│ surgery │
└──────────────────────────────────────────────────────────────────┘
A. CONSERVATIVE (WATCHFUL WAITING)
- First-line for < 3 months duration (NICE CG60 Guidelines, AAO-HNS Guidelines)
- 50% spontaneous resolution within 3 months
- 75% resolution within 6 months
Medical measures (limited evidence but used):
| Drug | Evidence | Guideline Status |
|---|---|---|
| Autoinflation (Otovent device) | Moderate | Recommended (NICE 2023) |
| Intranasal corticosteroids | Limited | May help with concurrent rhinitis |
| Oral antibiotics | Not routinely recommended | AAO-HNS against routine use |
| Antihistamines | No proven benefit | NOT recommended |
| Decongestants | No proven benefit | NOT recommended |
| Mucolytics (Carbocisteine) | Controversial | Used in some guidelines (Dhingra) |
"Antihistamines, decongestants, and steroids do not reliably help in OME" — Harrison's Principles (p. 1061)
B. SURGICAL MANAGEMENT
Indications for Surgery (NICE 2023 / AAO-HNS / Scott-Brown):
- Persistent OME ≥ 3 months with bilateral hearing loss ≥ 25–30 dB HL
- Persistent OME ≥ 3 months with significant speech/language delay
- Balance problems / vestibular dysfunction
- TM retraction progressing toward cholesteatoma
- Recurrent OME after previous surgical treatment
- Special needs children (Down syndrome, cleft palate) — early surgery
i. MYRINGOTOMY (Paracentesis)
Definition: Incision in the TM to aspirate middle ear fluid
Site of incision: Anteroinferior quadrant (safe zone — away from ossicles and facial nerve)
Technique:
- Performed under GA in children, LA in adults
- Radial incision in anteroinferior quadrant
- Fluid aspirated by suction
- Specimen sent for culture
Myringotomy Sites Diagram:
Tympanic Membrane
┌─────────────────────────┐
│ Posterosuperior │ │
│ (DANGEROUS - │ │
│ ossicles/chorda) │ │
│─────────────────────────│
│ Posteroinferior │Ant│
│ │INF│ ← SAFE ZONE
│ │ │ (Myringotomy site)
└─────────────────────────┘
Handle of Malleus (vertical)
ii. TYMPANOSTOMY TUBE INSERTION (GROMMET / VENTILATION TUBE)
Principle: Restore middle ear ventilation by creating an artificial ET
Types of Grommets:
| Type | Duration | Use |
|---|---|---|
| Short-term (Shah/Shepard grommet) | 6–12 months | First-line; most common |
| Long-term (T-tube / Goode T-tube) | 2–4 years | Recurrent OME; cleft palate |
| Per-Lee grommet | Long-term | Selected cases |
Grommet Placement Flowchart:
Myringotomy incision (anteroinferior quadrant)
│
Fluid aspirated
│
Grommet inserted with alligator
forceps / grommet introducer
│
Grommet seated in incision
│
Topical antibiotic drops (Ciprofloxacin)
│
Review at 6 weeks, then 6-monthly
│
┌──────────────┴──────────────┐
Extruded (normal) Still in place?
(6–12 months) Check for blockage
│
TM heals in >95%
Results:
- Immediate improvement in hearing (10–15 dB average gain)
- Improved quality of life scores (OMQ-14)
- 70–80% success rate in clearing effusion
Complications of Grommet:
| Complication | Frequency |
|---|---|
| Persistent otorrhea | 10–15% |
| Blocked grommet | 5–10% |
| Premature extrusion | 5% |
| Persistent TM perforation after extrusion | 2–3% |
| Tympanosclerosis | 30–40% (usually not clinically significant) |
| Cholesteatoma (rare) | < 1% |
| Atrophic TM | Uncommon |
iii. ADENOIDECTOMY
Rationale (Scott-Brown, Cummings):
- Adenoids act as bacterial reservoir → biofilm → recurrent OME
- Adenoid pad mechanically obstructs ET orifice
- Randomized evidence shows adenoidectomy alone effective in children > 4 years
Indications:
- Adenoid hypertrophy present
- Age > 4 years
- Recurrent OME after first grommet
- Concurrent nasal obstruction
TARGET Trial (MRC, UK): Adenoidectomy + grommets reduced recurrence of OME significantly in children over 3 years compared to grommets alone.
Combined Procedure (Shah's grommet + Adenoidectomy):
GA + Boyle-Davis gag (adenoidectomy)
│
Adenoid curette / suction diathermy
│
Myringotomy + grommet insertion
│
Post-op antibiotic drops
iv. HEARING AIDS (ALTERNATIVE TO SURGERY)
- Bone-anchored hearing aids (BAHA) or conventional aids
- In children not suitable for surgery (coagulopathy, anesthetic risk)
- Cleft palate with persistent OME
COMPLICATIONS
| Complication | Description |
|---|---|
| Conductive hearing loss | 15–40 dB — primary complication |
| Speech/language delay | Critical in 0–5 years |
| Academic underachievement | Secondary to hearing loss |
| TM retraction pocket | Can progress to cholesteatoma |
| Tympanosclerosis | White plaques, minimal functional significance |
| Adhesive otitis media | TM adherent to medial wall |
| Cholesteatoma | End-stage complication |
| Ossicular erosion | Incus long process most common |
| Atelectasis of TM | Progressive retraction |
COMPLICATIONS FLOWCHART
UNTREATED / RECURRENT SOM
│
┌─────────────────────────┐
│ │
Hearing loss TM retraction
│ │
Speech delay ┌─────┴──────────┐
Poor academics Mild Progressive
(Watch) │
┌──────┴──────┐
Pars tensa Pars flaccida
retraction retraction
│ │
Adhesive OM Attic
Tympanosclerosis cholesteatoma
│
Mastoiditis
Ossicular erosion
Sensorineural loss
GRADING / STAGING
Sade's Classification of TM Retraction (used in SOM complications):
| Grade | Description |
|---|---|
| Grade I | Mild retraction |
| Grade II | Retraction touching incus/stapes |
| Grade III | TM adherent to promontory (but mobile) |
| Grade IV | TM adherent to promontory (non-mobile = adhesive OM) |
Tos Classification of Middle Ear Effusion:
| Type | Fluid character |
|---|---|
| Type I | Serous (watery) |
| Type II | Mucoid (thick) |
| Type III | Fibrinoid (very thick, rubbery) |
PROGNOSIS
- Children: 50% resolve within 3 months, 75% within 6 months (AAO-HNS)
- Recurrence rate: 30–40% after first grommet
- After second grommet + adenoidectomy: 80% resolution
- Long-term hearing: excellent if treated early
- Risk of permanent sensorineural loss: rare but possible with prolonged untreated OME
RECENT ADVANCES (As per RGUHS Current Curriculum)
1. Biofilm Research
- Molecular studies confirm bacterial biofilms (especially H. influenzae) on middle ear mucosa in 80% of chronic OME
- Biofilms explain antibiotic treatment failures
- Future: anti-biofilm agents (xylitol, N-acetylcysteine, DNase) under trial
2. Microbiology Updates
- 16S rRNA gene sequencing — culture-negative OME still shows bacterial DNA
- Polymicrobial biofilms are the rule, not the exception
3. Autoinflation (Otovent)
- CARNIVAL RCT (2015): Autoinflation device for 3 months → significant improvement in tympanogram and hearing vs. control
- NICE 2023 guideline update: Autoinflation now formally recommended before surgical referral
4. Mucolytics and Biologics
- Carbocisteine: Reduces viscosity of glue ear fluid; used adjunctively
- Anti-IL-8 / anti-leukotriene therapy: Experimental
- Dexamethasone-eluting grommets: Under clinical trial phase II
5. Probiotics
- Lactobacillus rhamnosus supplementation — reduced recurrence of OME in RCT (Finnish study, 2020)
6. Endoscopic Ear Surgery (EES)
- Fully endoscopic myringotomy and grommet insertion now feasible
- Better visualization of anteroinferior quadrant without microscope
- Shorter operating time, better patient acceptance
7. Minimally Invasive Office-Based Grommet
- Tula System (in-office, iontophoresis-based local anesthesia + laser myringotomy): FDA-approved for adults; avoids GA
- Laser-assisted myringotomy with KTP/CO₂ laser: self-sealing incision without grommet
8. Imaging Advances
- MRI with diffusion-weighted imaging (DWI): differentiates glue ear from non-EPI cholesteatoma
- High-resolution OCT (Optical Coherence Tomography) of TM: noninvasive middle ear fluid detection
9. Nasal Steroid Evidence
- ORNAMENT-1 trial (2019): Intranasal mometasone did NOT improve OME outcomes in children significantly
- Current recommendation: intranasal steroids NOT routinely recommended for OME alone; useful only for concurrent allergic rhinitis
10. Genetic / Immunological Factors
- NEMO mutation → NF-κB pathway → recurrent OME
- MUC5B promoter polymorphism — associated with increased susceptibility
- TLR4 gene polymorphism — predisposes to recurrent OME
SCREENING (RGUHS — Public Health Aspect)
| Age | Recommended Screening |
|---|---|
| Neonates (0–28 days) | OAE universal newborn hearing screening |
| Infants (3 months) | AABR if OAE failed |
| Pre-school (4–5 years) | Pure tone sweep audiometry (screening) |
| School-age | Annual audiometric screening |
UNHCR/WHO Recommendation: Universal newborn hearing screening detects OME sequelae early enough for language intervention.
SUMMARY TABLE
| Feature | Details |
|---|---|
| Definition | Non-purulent ME fluid, intact TM, no acute infection |
| Most common age | 2–7 years |
| Primary etiology | ET dysfunction |
| Key symptom | Conductive hearing loss (15–40 dB) |
| Otoscopic hallmark | Amber/dull TM, retracted, air-fluid level |
| Diagnostic test | Tympanometry — Type B (flat) |
| Observation period | 3 months before intervention |
| First-line surgery | Myringotomy + Grommet (Ventilation Tube) |
| Add adenoidectomy | Age > 4 years + adenoid hypertrophy + recurrence |
| Key complication | TM retraction → Cholesteatoma |
| Recent advance | Biofilms, autoinflation (CARNIVAL), endoscopic surgery, Tula system |
| NICE 2023 | Autoinflation before surgery; no antibiotics/antihistamines |
REFERENCES
- Scott-Brown's Otolaryngology, Head and Neck Surgery, 8th Edition — Volume 2, Chapter on Otitis Media
- Cummings Otolaryngology — Head and Neck Surgery, 7th Edition, Flint et al., Chapter 194–195
- Stell & Maran's Textbook of Head and Neck Surgery, 5th Edition
- Diseases of Ear, Nose and Throat, PL Dhingra, 7th Edition — Chapter on Glue Ear
- ENT — Head and Neck Surgery, Hazarika, 4th Edition
- A Textbook of ENT, Zakir Hussain — Middle Ear Diseases
- Harrison's Principles of Internal Medicine, 21st Edition, p. 1060–1061
- NICE Guideline CG60 (2008, updated 2023): Surgical Management of OME in Children
- AAO-HNS Clinical Practice Guideline: OME (2016 update)
- Maw AR et al., CARNIVAL Trial — BMJ 2015 — Autoinflation for OME
- van Zon A et al. — Cochrane Review on Grommets vs Watchful Waiting (2012, updated 2022)
- MRC TARGET Trial — Adenoidectomy effect on OME recurrence
Examiner's Note (RGUHS 50-mark emphasis): A complete answer should include Definition, Epidemiology, Etiology/Pathogenesis (with flowchart), Clinical Features, Investigations (Tympanometry central), Management (medical + surgical with grommets in detail), Complications, and Recent Advances. Diagrams of the TM, tympanogram types, and grommet placement are expected in the answer script.
This is a shared conversation. Sign in to Orris to start your own chat.