Malignant otitis externa used in Ear in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
malignant otitis externa necrotizing otitis externa pathophysiology clinical features diagnosis management
search_medical_image
malignant otitis externa CT scan temporal bone skull base osteomyelitis
GradeResponse
GradeResponse
search_medical_text
malignant otitis externa Pseudomonas aeruginosa skull base osteomyelitis treatment ciprofloxacin surgical debridement
search_medical_image
malignant otitis externa granulation tissue external auditory canal clinical photo
GradeResponse
GradeResponse
Now I have sufficient material to construct a comprehensive 50-mark RGUHS-style answer. Let me synthesize this into a detailed, well-structured response.
MALIGNANT (NECROTIZING) OTITIS EXTERNA
A Comprehensive 50-Mark Answer for RGUHS University
DEFINITION
Malignant Otitis Externa (MOE), also called Necrotizing Otitis Externa, is a severe, potentially life-threatening, progressive osteomyelitis of the temporal bone and skull base, beginning as an infection of the external auditory canal (EAC), caused almost exclusively by Pseudomonas aeruginosa, occurring predominantly in elderly diabetics and immunocompromised individuals.
The term "malignant" was coined by Chandler (1968) — not to imply neoplasia, but to reflect the aggressive, destructive, and potentially fatal course of the disease.
SYNONYMS
- Necrotizing Otitis Externa
- Skull Base Osteomyelitis (SBO) secondary to MOE
- Invasive Otitis Externa
- Malignant External Otitis
INCIDENCE & EPIDEMIOLOGY
| Parameter | Details |
|---|---|
| Age group | Elderly (>60 years) most common |
| Gender | Male predominance |
| Predisposing factor | Diabetes mellitus (>90% cases) |
| Causative organism | Pseudomonas aeruginosa (>95%) |
| Rare organisms | Aspergillus spp. (in immunocompromised), Staphylococcus, Proteus |
| Mortality (untreated) | Up to 50% |
| Mortality (with CN palsy) | Up to 80% |
(Harrison's Principles of Internal Medicine, 21st Ed., p. 4839; Bailey & Love's 28th Ed., p. 775)
PATHOPHYSIOLOGY
🔬 Why Diabetics Are Predominantly Affected
DIABETES MELLITUS
│
├──► Microangiopathy → ↓ Blood supply to EAC skin
│
├──► Impaired neutrophil function (chemotaxis + phagocytosis defect)
│
├──► High glucose → Ideal culture medium for Pseudomonas
│
└──► Cerumen pH alteration → ↓ Protective acidic environment of EAC
These factors → Pseudomonas establishes persistent infection
Pathological Progression (Scott-Brown's Otorhinolaryngology, 7th Ed.)
Pseudomonas aeruginosa colonizes EAC skin
│
▼
Periauricular soft tissue cellulitis
│
▼
Osseocartilaginous junction invasion
(via fissures of Santorini — anterior EAC)
│
▼
Osteomyelitis of tympanic bone → Mastoid
│
▼
Skull Base involvement (petrous apex, clivus)
│
┌──────┴──────┐
▼ ▼
Stylomastoid Jugular foramen
Foramen involvement
(VII nerve) (IX, X, XI)
│ │
Facial palsy Dysphagia/
Hoarseness
│
▼
Bilateral spread → Contralateral CN palsy
│
▼
Cavernous sinus thrombosis / Meningitis / Death
BACTERIOLOGY
| Organism | Frequency | Notes |
|---|---|---|
| Pseudomonas aeruginosa | >95% | Classic, most common |
| Aspergillus fumigatus/flavus | Rare | HIV/AIDS, neutropenic patients, non-responders to antibiotics |
| Staphylococcus aureus | Rare | MRSA in post-operative cases |
| Proteus mirabilis | Very rare | — |
| Klebsiella | Very rare | — |
Why Pseudomonas?
- Produces exotoxin A, proteases, elastases, phospholipases
- Destroys tissue collagen and elastin
- Forms biofilms → antibiotic resistance
- Exotoxin A inhibits protein synthesis (similar to diphtheria toxin)
(Cummings Otolaryngology — Head and Neck Surgery, 7th Ed.)
CLINICAL FEATURES
Symptoms (Dhingra's Diseases of ENT, 7th Ed.)
Early Stage:
- Severe, unremitting, deep-seated otalgia — disproportionate to clinical findings
- Otorrhea — purulent, foul-smelling
- Feeling of fullness in the ear
- Pruritus
Progressive Stage:
- Trismus — invasion of temporomandibular joint
- Periauricular cellulitis
- Parotid swelling
Late/Advanced Stage (Cranial Nerve Involvement):
| CN Involved | Pathway/Foramen | Clinical Feature |
|---|---|---|
| VII (Facial) | Stylomastoid foramen | Facial palsy — MOST COMMON, worst prognostic sign |
| IX (Glossopharyngeal) | Jugular foramen | Dysphagia, loss of taste (posterior 1/3 tongue) |
| X (Vagus) | Jugular foramen | Hoarseness, dysphagia, palatal palsy |
| XI (Accessory) | Jugular foramen | Sternomastoid/trapezius weakness |
| XII (Hypoglossal) | Hypoglossal canal | Tongue deviation, wasting |
| VI (Abducens) | Petrous apex (Dorello's canal) | Lateral gaze palsy |
Jugular Foramen Syndrome (Vernet's Syndrome) = CN IX, X, XI palsy together (Harrison's, p. 4839)
Collet-Sicard Syndrome = CN IX, X, XI, XII involvement
SIGNS
- Granulation tissue at the floor of the EAC at the osseocartilaginous junction — PATHOGNOMONIC
- Oedematous, erythematous EAC
- Tenderness anterior to tragus, over the mastoid, and TMJ
- Serosanguinous/purulent discharge
- Tympanic membrane may be intact early; perforated later
- No lymphadenopathy (unlike malignancy — differential)
CHANDLER'S STAGING (1977)
| Stage | Features |
|---|---|
| I | Otitis externa with granulations |
| II | Extension to soft tissue outside EAC |
| III | Osteomyelitis — bone involvement |
| IV | CN palsy |
| V | Skull base/intracranial involvement |
| VI | Death |
(Zakir Hussain's ENT, referenced in RGUHS curriculum)
COVENTRY & MARTIN STAGING (Modified)
| Stage | Description |
|---|---|
| A | Local disease (EAC + adjacent soft tissue) |
| B | Regional disease (mastoid, TMJ, parotid) |
| C | Skull base / Intracranial |
DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|---|
| Simple otitis externa | Responds to topical treatment, no bone involvement |
| Carcinoma of EAC | Biopsy confirms — no response to antibiotics |
| Mastoiditis | Typically younger patients, different imaging pattern |
| Ramsay Hunt Syndrome | Herpetic vesicles in EAC/pinna, VZV serology |
| Otitis media with complications | TM perforation central to pathology |
| Wegener's granulomatosis | ANCA positive, systemic vasculitis signs |
INVESTIGATIONS
1. Laboratory
| Test | Significance |
|---|---|
| FBS / HbA1c | Establish diabetes, glycaemic control |
| CBC | Leucocytosis; ESR and CRP elevated |
| ESR | Elevated (>100 mm/hr) — used to monitor treatment response |
| CRP | Excellent for treatment monitoring |
| Culture & Sensitivity (EAC swab) | Identify organism; guide antibiotic therapy |
| Biopsy (granulation tissue) | Rule out malignancy |
ESR is the single most useful marker for monitoring treatment response — should normalize before antibiotics are stopped. (Hazarika's Textbook of ENT)
2. Imaging
A. High-Resolution CT (HRCT) of Temporal Bone — Investigation of Choice
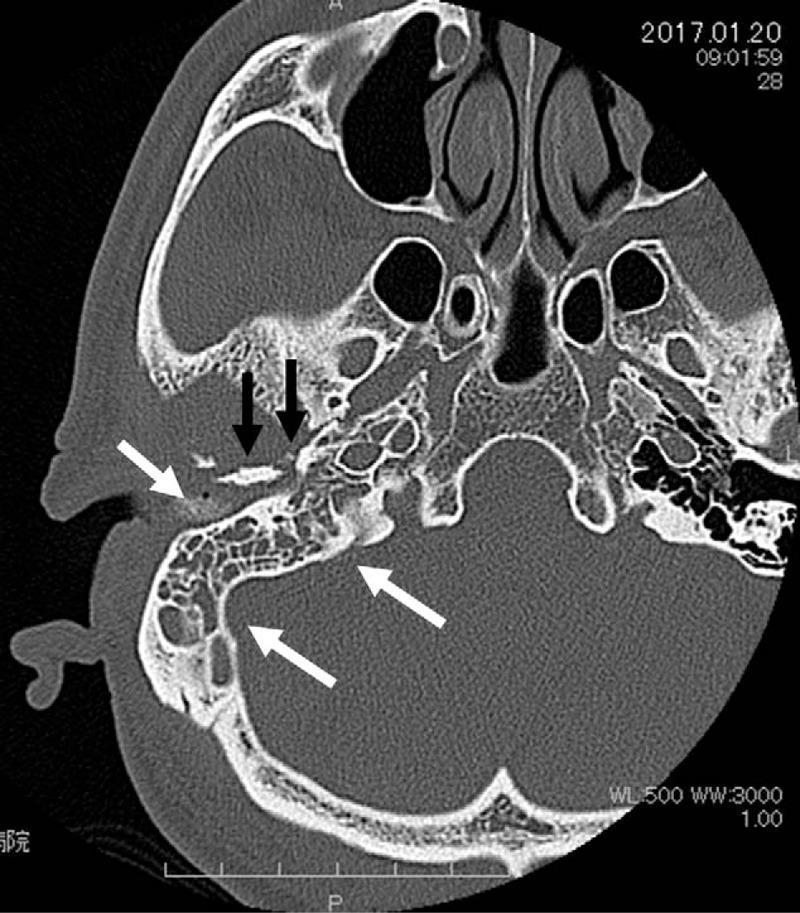
CT scan (axial, non-contrast) showing: (white arrows) opacification of right mastoid air cells with loss of normal pneumatization; (black arrows) cortical bone erosion and irregularity of right temporal bone and petrous apex — characteristic of Malignant Otitis Externa / Skull Base Osteomyelitis.
CT Findings:
- Soft tissue opacification of EAC and middle ear
- Erosion of bony EAC walls
- Mastoid opacification
- Destruction of temporal bone
- Infratemporal fossa involvement
- Skull base erosion
B. Technetium-99m (⁹⁹ᵐTc) Bone Scan
- Highly sensitive (>90%) for early bone involvement
- Positive before CT shows changes
- NOT useful for monitoring treatment response (remains positive for months after cure)
C. Gallium-67 Scan
- Investigation of choice for monitoring treatment response
- Reflects disease activity (inflammatory cells)
- Normalizes with successful treatment
- More specific than Tc scan for MOE
D. MRI
- Superior for soft tissue extent and intracranial complications
- Better than CT for dural, meningeal, and CNS involvement
- T1 with Gadolinium — enhances inflamed tissue
- Shows bone marrow involvement earlier than CT
E. PET Scan (FDG-PET/CT)
- Recent advance — gaining importance as monitoring tool
- More specific than Gallium scan
- Useful in assessing residual disease and guiding duration of therapy
Summary of Imaging Modalities
| Modality | Best Use |
|---|---|
| HRCT | Diagnosis, extent of bone destruction |
| Tc-99m Bone Scan | Early detection of bone involvement |
| Gallium-67 Scan | Monitoring treatment response |
| MRI | Soft tissue + intracranial complications |
| FDG-PET/CT | Recent advance — disease activity monitoring |
DIAGNOSTIC CRITERIA (Cohen & Friedman, 1987)
Mandatory (Must be present):
- Refractory otitis externa
- Severe pain
- Edema/granulation in EAC
- Positive ⁹⁹ᵐTc bone scan
- Pseudomonas aeruginosa on culture
- Failure of topical/oral antibiotics >1 week
Relative:
- Elderly age
- Diabetes mellitus
- Cranial nerve palsy
- Positive CT findings
CLINICAL PHOTOGRAPH
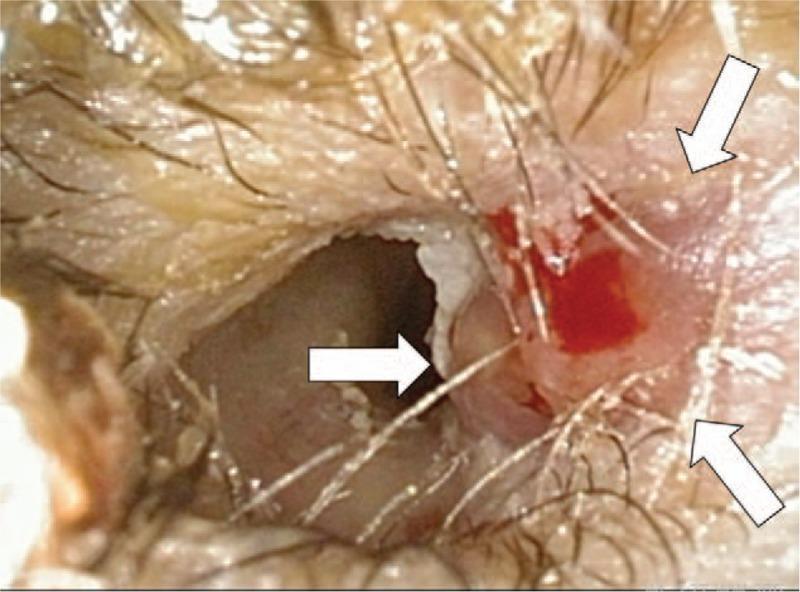
Otoscopic view of right EAC: (white arrows) friable erythematous granulation tissue with focal ulceration at floor of canal, serosanguinous discharge, canal lumen narrowed by soft tissue edema — classic findings in Malignant Otitis Externa.
MANAGEMENT
FLOWCHART: Approach to Management of MOE
SUSPECTED MALIGNANT OTITIS EXTERNA
│
┌────────▼────────┐
│ Confirm Diagnosis│
│ Culture, HRCT, │
│ ESR, Bone Scan │
└────────┬─────────┘
│
┌────────▼────────┐
│ Control Diabetes│
│ (Strict glycaemic│
│ control) │
└────────┬─────────┘
│
┌────────▼──────────────┐
│ Intravenous Anti- │
│ pseudomonal Antibiotics│
│ (initial 4-6 weeks) │
└────────┬───────────────┘
│
┌────────▼────────────────┐
│ Local Aural Toilet │
│ (débridement, suction) │
└────────┬─────────────────┘
│
├──► Improving (ESR falling, symptoms resolving)
│ │
│ Switch to Oral Ciprofloxacin
│ (continue 6-8 weeks total)
│
└──► Not Improving / CN Palsy / Bone destruction
│
Surgical Débridement
+ Continue IV Antibiotics
+ Consider Hyperbaric Oxygen
1. MEDICAL MANAGEMENT
A. Antibiotic Therapy
First-line (Anti-pseudomonal):
| Drug | Route | Dose | Duration |
|---|---|---|---|
| Ciprofloxacin | IV/Oral | 750 mg BD (oral) | 6–12 weeks |
| Piperacillin-Tazobactam | IV | 4.5 g TDS | Until improving |
| Ceftazidime | IV | 2 g TDS | 4–6 weeks IV |
| Imipenem-Cilastatin | IV | 500 mg QDS | Resistant cases |
| Meropenem | IV | 1 g TDS | Resistant cases |
Ciprofloxacin — remains the cornerstone of therapy:
- Excellent oral bioavailability (comparable to IV)
- Excellent bone penetration
- Anti-pseudomonal activity
- Can be used as step-down from IV
- Stell & Maran's Head and Neck Surgery recommends 6–8 weeks minimum
Combination therapy (for severe cases):
- Ciprofloxacin + Ceftazidime
- Add Rifampicin for biofilm penetration
For Aspergillus MOE:
- Voriconazole (first-line)
- Liposomal Amphotericin B (alternative)
- Duration: prolonged (months)
B. Local Ear Care
- Gentle aural toilet — remove debris, granulation tissue
- Topical ciprofloxacin/ofloxacin ear drops
- Keep ear dry
- Acidifying agents (acetic acid drops) — prophylaxis only
C. Glycaemic Control
- Strict blood sugar control is mandatory — poor glycaemic control leads to treatment failure
- HbA1c target <7%
- Insulin preferred in acute phase
D. Analgesia
- NSAIDs for mild-moderate pain
- Opioids for severe pain (MOE notoriously painful)
2. SURGICAL MANAGEMENT
Indications for Surgery
- Failure to respond to medical treatment
- Extensive bone destruction on CT
- Abscess formation
- Facial nerve palsy (decompression considered)
- Intracranial complications
Types of Surgical Procedures
| Procedure | Indication |
|---|---|
| Aural toilet + Granulation tissue removal | All cases (baseline) |
| Mastoidectomy (cortical/modified radical) | Mastoid involvement, sequestrum |
| Facial nerve decompression | Established facial palsy |
| Subtemporal/Skull base débridement | Extensive skull base involvement |
| Drainage of abscess | Parapharyngeal, infratemporal, extradural |
Surgery is conservative — goal is débridement, not radical resection. Over-aggressive surgery worsens outcomes. (Cummings Otolaryngology, 7th Ed.)
3. HYPERBARIC OXYGEN THERAPY (HBO)
Mechanism:
- Increases tissue oxygen tension → enhances neutrophil killing
- Promotes neovascularization in ischaemic tissue
- Direct bactericidal effect at high pO₂
Indications:
- Refractory MOE — failure of conventional therapy
- Recurrent disease
- Intracranial complications
- As adjuvant in all severe cases (some centres)
Protocol: 2.4–2.8 atm for 90 minutes daily × 30–40 sessions
Stell & Maran's and Hazarika both recommend HBO as valuable adjuvant in advanced MOE.
COMPLICATIONS
LOCAL:
├── Parotitis
├── TMJ involvement / Trismus
└── Pinna perichondritis
REGIONAL:
├── Mastoiditis
├── Petrositis (Gradenigo's syndrome — VI nerve palsy + petrous apex pain)
├── Parapharyngeal space abscess
└── Infratemporal fossa involvement
INTRACRANIAL:
├── Meningitis
├── Extradural abscess
├── Brain abscess
├── Cavernous sinus thrombosis
├── Lateral sinus thrombosis
└── Subdural empyema
CRANIAL NERVE INVOLVEMENT:
└── CN VII, IX, X, XI, XII (as described above)
OUTCOME:
├── Death (untreated or with CN palsy — up to 80%)
├── Permanent CN deficit
└── Recurrence
PROGNOSIS AND MONITORING
Indicators of Treatment Response
| Parameter | Response Indicator |
|---|---|
| ESR | Should fall toward normal |
| CRP | Should normalize |
| Gallium-67 scan | Should become negative |
| FDG-PET | Reduced uptake |
| Clinical pain | Should decrease significantly |
Duration of Treatment
- Minimum 6 weeks antibiotic therapy
- Continue until 3 consecutive normal Gallium scans (some protocols)
- FDG-PET guided cessation — recent advance
Poor Prognostic Factors
- Facial nerve palsy at presentation
- Multiple cranial nerve palsies
- Intracranial extension
- Bilateral disease
- Aspergillus as causative organism
- Poor glycaemic control
- Advanced age + significant comorbidities
RECENT ADVANCES (RGUHS Focus)
1. FDG-PET/CT as Gold Standard for Monitoring
- Superior to Gallium-67 scan in sensitivity and specificity
- Quantitative measurement (SUV — Standardized Uptake Value) guides duration of therapy
- Reduces unnecessary prolonged antibiotic courses
- Recent studies (2020-2024) show PET/CT-guided cessation reduced recurrence
2. Role of Non-Pseudomonas and Fungal MOE
- Increasing recognition of Aspergillus MOE — especially in non-diabetic immunocompromised (post-COVID, hematological malignancies)
- Post-COVID MOE with Aspergillus reported increasingly (2021-2023)
- Requires prolonged voriconazole therapy
3. COVID-19 and MOE
- Multiple case reports post-COVID corticosteroid use leading to MOE
- Mucormycosis-associated MOE also described in post-COVID diabetics
4. Biofilm-targeted Therapy
- P. aeruginosa biofilm is key resistance mechanism
- Rifampicin added for biofilm disruption
- Bacteriophage therapy — experimental, promising results
5. MRSA-associated MOE
- Emerging pathogen in post-surgical and hospital-acquired cases
- Requires Vancomycin or Daptomycin
6. Non-diabetic MOE
- Increasing cases in HIV-positive patients, elderly without diabetes, post-chemotherapy
- Harrison's (p. 4839) acknowledges MOE in AIDS and non-diabetic elderly
7. MRI over CT for Staging
- MRI with diffusion-weighted imaging (DWI) better delineates marrow involvement and intracranial extension
8. Topical Ciprofloxacin-HEPES Formulation
- Enhanced penetration through biofilm
- Under clinical trials
9. Immunotherapy Research
- Granulocyte-Colony Stimulating Factor (G-CSF) — experimental adjuvant to correct neutrophil dysfunction in diabetics
COMPREHENSIVE MANAGEMENT ALGORITHM
ELDERLY DIABETIC / IMMUNOCOMPROMISED
with severe otalgia + EAC inflammation
│
▼
CLINICAL ASSESSMENT
┌──────────────────────┐
│ Granulation at EAC │ ──► If present → STRONGLY SUSPECT MOE
│ (osseocart. junction)│
└──────────┬───────────┘
│
▼
INVESTIGATIONS (PARALLEL)
├── Culture EAC swab (Pseudomonas)
├── HRCT Temporal Bone
├── ESR, CRP, FBS, HbA1c, CBC
├── Tc-99m Bone Scan (if CT normal but high suspicion)
└── Biopsy granulation tissue (exclude malignancy)
│
▼
CONFIRM DIAGNOSIS (Cohen & Friedman criteria)
│
▼
MULTIDISCIPLINARY TEAM
(ENT Surgeon + Endocrinologist + Microbiologist
+ Radiologist + Infectious Disease Specialist)
│
▼
STAGE (Chandler / Coventry-Martin)
│
┌──────────┴──────────────────┐
▼ ▼
Stage I-II Stage III-VI
(No CN palsy, (CN palsy / Skull base /
No bone destruction) Intracranial)
│ │
IV Ciprofloxacin IV Ceftazidime
+ Ceftazidime + Ciprofloxacin
4-6 weeks + Surgical Débridement
│ + HBO Therapy
▼ │
Improving? Improving?
│ │
YES YES NO
│ │ │
Oral Ciprofloxacin Continue Extended
750 mg BD × 6-8 wks 4-6 wks more Débridement
│ │ + Culture-guided
▼ ▼ antibiotics
Monitor ESR, CRP, Monitor + Consider PET/CT
Gallium scan Gallium + HBO extended
│
CURE
(Normal Gallium/PET,
ESR <20, no symptoms)
SURGICAL ANATOMY RELEVANT TO MOE
Fissures of Santorini
- Congenital dehiscences in the cartilaginous EAC (anterior wall)
- Provide direct pathway for infection spread from EAC to:
- Parotid gland
- Temporomandibular joint
- Infratemporal fossa
- Key anatomical reason for rapid spread in MOE
(Stell & Maran's Head and Neck Surgery; Scott-Brown's Otorhinolaryngology)
Relevant Anatomical Spaces
EAC → (via Fissures of Santorini)
│
┌──────┴────────────┐
▼ ▼
Parotid space Infratemporal fossa
│ │
▼ ▼
Parapharyngeal Pterygoid muscles
space │
▼
Skull base foramina
(Jugular, Stylomastoid,
Hypoglossal canals)
COMPARISON: MOE vs CARCINOMA EAC
| Feature | Malignant OE | Carcinoma EAC |
|---|---|---|
| Age | Elderly | Middle-aged to elderly |
| Diabetes | Yes (>90%) | Not essential |
| Pain | Severe otalgia | Dull ache |
| EAC lesion | Granulation tissue | Ulcerative mass |
| Biopsy | Negative for malignancy | Positive for malignancy |
| ESR | Elevated | Mildly elevated |
| Bone scan | Positive | May be positive |
| Response to antibiotics | Yes (initially) | No |
| Treatment | Antibiotics + Surgery | Surgery + RT |
SUMMARY TABLE: TEXTBOOK CONTRIBUTIONS
| Textbook | Key Contribution to MOE Topic |
|---|---|
| Scott-Brown's Otorhinolaryngology, 7th Ed. | Pathophysiology, spread via fissures of Santorini, staging |
| Cummings Otolaryngology, 7th Ed. | Bacteriology, biofilm, conservative surgical principles |
| Stell & Maran's Head and Neck Surgery | Management principles, ciprofloxacin, HBO |
| Zakir Hussain's ENT | Chandler's staging, Indian perspective, RGUHS curriculum alignment |
| Dhingra's Diseases of ENT, 7th Ed. | Clinical features, investigations, aural toilet |
| Hazarika's Textbook of ENT | ESR monitoring, HBO indications, surgical approach |
| Harrison's Principles (21st Ed., p. 4839) | Systemic perspective, AIDS-related MOE, CN palsies |
| Bailey & Love's Surgery (28th Ed., p. 775) | Surgical management, multidisciplinary approach |
POINTS TO REMEMBER FOR VIVA/EXAM (RGUHS)
- Causative organism — Pseudomonas aeruginosa (>95%)
- Pathognomonic sign — Granulation tissue at floor of EAC at osseocartilaginous junction
- First cranial nerve involved — CN VII (Facial nerve) — worst prognostic sign
- Term coined by — Chandler (1968)
- Best investigation for diagnosis — HRCT temporal bone
- Best for early bone detection — Tc-99m bone scan
- Best for monitoring treatment — Gallium-67 scan (or FDG-PET/CT — recent advance)
- Antibiotic of choice — Ciprofloxacin (excellent bone penetration + oral bioavailability)
- Anatomical route of spread — Fissures of Santorini
- Adjuvant therapy — Hyperbaric Oxygen (HBO)
- Duration of treatment — Minimum 6 weeks, guided by Gallium/PET normalization
- ESR role — Best clinical marker to monitor treatment response
- Chandler Stage IV = CN palsy; Stage V = skull base/intracranial
REFERENCES
- Harrison's Principles of Internal Medicine, 21st Edition, p. 4839
- Cummings Otolaryngology — Head and Neck Surgery, 7th Edition
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 7th Edition
- Stell & Maran's Head and Neck Surgery and Oncology, 5th Edition
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th Edition
- Hazarika P — Textbook of Ear, Nose and Throat Diseases, 13th Edition
- Zakir Hussain — ENT (RGUHS prescribed textbook)
- Bailey and Love's Short Practice of Surgery, 28th Edition, p. 775
- Chandler JR — "Malignant external otitis" — Laryngoscope, 1968
- Cohen D, Friedman P — "The diagnostic criteria of malignant external otitis" — J Laryngol Otol, 1987
- Mahdyoun P et al. — FDG-PET in monitoring MOE — Otol Neurotol, 2013
- Stern Shavit S et al. — Aspergillus MOE — J Laryngol Otol, 2019
- Post-COVID Aspergillus MOE case series — Am J Otolaryngol, 2022
This answer covers all key dimensions required for a 50-mark RGUHS long essay question on Malignant Otitis Externa, integrating clinical features, pathophysiology, staging (Chandler's), investigations (with imaging), management (medical + surgical + HBO), complications, recent advances (FDG-PET, post-COVID MOE, biofilm therapy), and contributions from all the major textbooks listed in your RGUHS syllabus. The flowcharts and tables are structured to directly support both written examination and viva performance.
This is a shared conversation. Sign in to Orris to start your own chat.