angina pectoris essay
Reading File
search_medical_text
angina pectoris pathophysiology types stable unstable vasospastic
search_medical_text
angina pectoris diagnosis ECG stress test management treatment
search_medical_image
angina pectoris ECG ischemia coronary artery disease diagram
GradeResponse
GradeResponse
GradeResponse
search_medical_text
stable ischemic heart disease pathophysiology coronary atherosclerosis demand supply mismatch
search_medical_text
angina nitrates beta blockers calcium channel blockers antiplatelet therapy revascularization PCI CABG
Here is a comprehensive essay on angina pectoris, drawing on retrieved sources and supplemented with established medical knowledge.
Angina Pectoris: A Comprehensive Essay
1. Introduction
Angina pectoris is a clinical syndrome of chest discomfort arising from myocardial ischemia — an imbalance between myocardial oxygen supply and demand — most commonly in the setting of obstructive coronary artery disease (CAD). The term was coined by William Heberden in 1768, who described it as "a sense of strangling and anxiety." It remains one of the most prevalent and clinically significant manifestations of ischemic heart disease (IHD), affecting tens of millions of people worldwide and serving as a key warning signal of underlying cardiovascular pathology.
2. Epidemiology
- Angina is a major public health burden, with an estimated 9 million adults in the United States affected.
- It is more prevalent in older adults and men, though post-menopausal women carry comparable risk.
- Risk is directly tied to cardiovascular risk factors: hypertension, hyperlipidemia, diabetes mellitus, smoking, obesity, physical inactivity, and family history of premature CAD.
3. Pathophysiology
At its core, angina results from myocardial ischemia — insufficient blood flow to meet the metabolic demands of the myocardium. The mechanism varies by subtype:
3.1 Supply-Demand Imbalance
The myocardium extracts ~70–75% of delivered oxygen at rest, leaving little reserve. When demand increases (e.g., exercise, emotional stress, tachycardia) or supply decreases (e.g., coronary stenosis, vasospasm, hypotension), ischemia ensues. Key determinants include:
| Factor | Effect on Oxygen Demand |
|---|---|
| Heart rate ↑ | Demand ↑ |
| Myocardial contractility ↑ | Demand ↑ |
| Wall stress (afterload/preload) ↑ | Demand ↑ |
| Coronary stenosis | Supply ↓ |
| Vasospasm | Supply ↓ |
| Hypotension/anemia | Supply ↓ |
3.2 Coronary Atherosclerosis
In stable angina, a fixed atherosclerotic plaque narrows the coronary lumen, limiting flow reserve. Blood flow is adequate at rest but insufficient during exertion. The plaque is typically stable (fibrous cap intact, no active thrombus).
In unstable angina (UA), a vulnerable plaque ruptures or erodes, triggering platelet aggregation and partial thrombosis — dramatically reducing perfusion, producing ischemia even at rest.
3.3 Vasospastic (Prinzmetal's) Angina
Caused by focal coronary artery spasm in the absence of obstructive plaque (though atherosclerosis may coexist). Mediated by smooth muscle hyperreactivity and endothelial dysfunction. Attacks characteristically occur at rest, often at night or early morning, and are associated with transient ST-segment elevation on ECG.
3.4 Microvascular Angina (Cardiac Syndrome X)
Ischemia originating from dysfunction of small coronary arterioles, not epicardial vessels. Common in women. Coronary angiography is normal, but stress testing reveals ischemia. Pathogenesis involves impaired endothelium-dependent vasodilation and abnormal pain sensitization.
4. Clinical Features
According to Harrison's Principles of Internal Medicine (p. 529), the characteristics of anginal discomfort are consistent across stable IHD, UA, and MI — differing primarily in pattern and duration. Chest discomfort is typically described as:
"Aching, heavy, squeezing, crushing, or constricting."
Classic Presentation
- Location: Substernal, may radiate to left arm, jaw, neck, shoulder, or back
- Character: Pressure, tightness, heaviness — rarely "sharp" or "pleuritic"
- Duration: 2–10 minutes (stable); >10–20 minutes raises concern for UA/NSTEMI
- Precipitants: Exertion, emotional stress, cold weather, heavy meals (stable angina)
- Relief: Rest, sublingual nitroglycerin (within 1–5 minutes)
- Associated symptoms: Dyspnea, diaphoresis, nausea, palpitations
Atypical Presentations
Particularly in women, diabetics, and the elderly, angina may present as:
- Epigastric discomfort or indigestion
- Jaw or arm pain without chest pain
- Exertional dyspnea as the primary "anginal equivalent"
- Fatigue
5. Classification
Canadian Cardiovascular Society (CCS) Grading of Angina
| Class | Description |
|---|---|
| I | Angina only with strenuous/rapid/prolonged exertion; ordinary activity does not cause angina |
| II | Slight limitation of ordinary activity (e.g., walking >2 blocks, climbing >1 flight of stairs) |
| III | Marked limitation of ordinary physical activity |
| IV | Inability to perform any physical activity without discomfort; angina may be present at rest |
Types of Angina
| Type | Mechanism | Precipitant | ECG Change | Relief |
|---|---|---|---|---|
| Stable | Fixed atherosclerotic stenosis | Exertion/stress | ST depression | Rest, nitrates |
| Unstable | Plaque rupture + partial thrombosis | Rest or minimal exertion | ST depression or T-wave changes | Requires urgent treatment |
| Prinzmetal's (Variant) | Coronary vasospasm | Rest, often nocturnal | Transient ST elevation | Nitrates, Ca²⁺ channel blockers |
| Microvascular | Small vessel dysfunction | Exertion | ST depression or normal | Variable |
6. Diagnosis
6.1 Clinical Assessment
A thorough history (character, location, duration, precipitants, relief) combined with cardiovascular risk factor profiling is the cornerstone of diagnosis. Pre-test probability guides the choice of investigations.
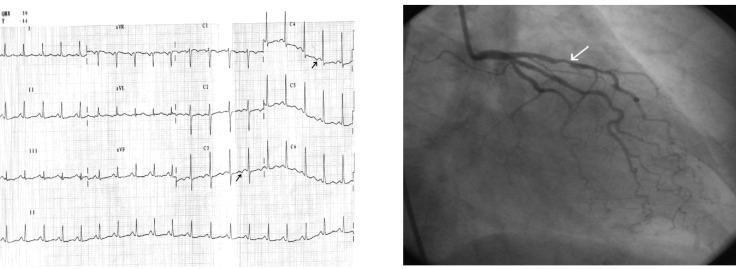
6.2 Resting ECG
- May be normal between episodes
- During ischemia: horizontal or downsloping ST-segment depression, T-wave inversion, or (in Prinzmetal's) ST elevation
- Persistent Q waves suggest prior MI
The image below illustrates the ECG-angiographic correlation in stable angina:
6.3 Stress Testing
- Exercise ECG (Treadmill test): First-line for intermediate-probability angina; positive if ≥1 mm ST depression at ≥0.08 sec past J-point
- Stress echocardiography: Detects wall motion abnormalities; higher sensitivity/specificity than exercise ECG
- Nuclear perfusion imaging (SPECT/PET): Identifies perfusion defects; useful when ECG is non-interpretable (e.g., LBBB, pacemaker)
- Stress cardiac MRI: Excellent for microvascular disease assessment
6.4 Coronary Imaging
- CT coronary angiography (CTCA): Excellent negative predictive value; preferred for low-to-intermediate probability; identifies plaque burden and stenosis non-invasively
- Invasive coronary angiography: Gold standard for anatomic assessment; required before revascularization; FFR (fractional flow reserve) used to assess hemodynamic significance of intermediate stenoses
6.5 Laboratory Tests
- Troponin (I or T): Normal in stable angina; elevated in UA/NSTEMI — critical distinguishing feature
- Lipid panel, fasting glucose, HbA1c: Risk factor assessment
- CBC: Exclude anemia as contributing factor
- TFTs: Exclude thyrotoxicosis as cause of demand ischemia
7. Management
As outlined in Harrison's Principles of Internal Medicine (p. 7508), management of stable angina must be individualized, encompassing:
- Patient education and reassurance
- Identification and treatment of aggravating conditions
- Activity modification
- Risk factor reduction
- Pharmacological therapy
- Consideration of revascularization
7.1 Risk Factor Modification (Secondary Prevention)
- Smoking cessation: Reduces risk of MI and mortality
- Blood pressure control: Target <130/80 mmHg (ACC/AHA 2017)
- Lipid management: High-intensity statins (atorvastatin 40–80 mg, rosuvastatin 20–40 mg); target LDL <70 mg/dL in established CAD
- Diabetes management: HbA1c <7% (individualized)
- Regular aerobic exercise: 150 min/week moderate-intensity
- Diet: Mediterranean-style diet; reduce saturated fats
7.2 Antiplatelet and Antithrombotic Therapy
- Aspirin 75–100 mg/day: Reduces risk of MI and cardiovascular death; cornerstone of stable CAD management
- Clopidogrel: Alternative if aspirin-intolerant; also added after PCI (dual antiplatelet therapy)
7.3 Anti-Anginal Drug Therapy
| Drug Class | Examples | Mechanism | Indication |
|---|---|---|---|
| Nitrates (short-acting) | Sublingual GTN | Venodilation → ↓ preload; coronary vasodilation | Acute angina relief |
| Nitrates (long-acting) | Isosorbide mononitrate | As above (tolerance requires nitrate-free interval) | Prophylaxis |
| Beta-blockers | Metoprolol, Atenolol | ↓ HR, contractility, BP → ↓ O₂ demand | First-line for stable angina, post-MI |
| Calcium channel blockers | Amlodipine (DHP), Diltiazem/Verapamil (non-DHP) | Vasodilation, ↓ HR/contractility | Alternative/adjunct; first-line for vasospastic angina |
| Ranolazine | Ranolazine | Inhibits late Iₙₐ current → ↓ diastolic wall tension | Refractory angina, adjunct |
| Ivabradine | Ivabradine | ↓ HR via If channel inhibition (sinus node) | When beta-blockers contraindicated/intolerant |
| Nicorandil | Nicorandil | ATP-sensitive K⁺ channel opener + nitrate effect | Used in Europe; reduces cardiovascular events |
Beta-blockers are the preferred first-line agents as they both relieve symptoms and improve prognosis (especially post-MI). Calcium channel blockers (especially non-dihydropyridines) are preferred for vasospastic angina.
7.4 Revascularization
Percutaneous Coronary Intervention (PCI)
- Drug-eluting stents (DES) deployed via catheter-based approach
- Indicated for:
- Significant single- or multi-vessel disease (with suitable anatomy) when symptoms persist despite optimal medical therapy
- High-risk anatomy (proximal LAD stenosis)
- COURAGE and ISCHEMIA trials showed PCI does not reduce mortality in stable angina vs. optimal medical therapy alone but does improve anginal symptoms and quality of life
Coronary Artery Bypass Grafting (CABG)
- Superior to PCI for:
- Left main coronary artery disease
- Three-vessel CAD (especially with reduced LV function, EF <35%)
- Diabetic patients with multi-vessel disease (FREEDOM trial)
- Uses internal mammary artery (LIMA to LAD — gold standard graft) and saphenous vein grafts
8. Special Populations
| Population | Key Considerations |
|---|---|
| Women | More frequent atypical symptoms; more microvascular disease; aspirin benefit vs. bleeding risk must be weighed carefully |
| Elderly | Higher comorbidity burden; polypharmacy risk; nitrate hypotension more common |
| Diabetics | Silent ischemia common; autonomic neuropathy blunts pain; CABG preferred over PCI for multi-vessel disease |
| CKD patients | Contrast nephropathy risk; adjust dosing; higher cardiovascular mortality |
9. Complications
If angina is not adequately managed, it may progress to:
- Acute coronary syndrome (ACS): Unstable angina, NSTEMI, STEMI
- Heart failure: Due to ischemic cardiomyopathy from repeated ischemic episodes
- Arrhythmias: Ventricular tachycardia/fibrillation, particularly during acute ischemia
- Sudden cardiac death
- Psychological morbidity: Depression and anxiety are common comorbidities that worsen prognosis
10. Prognosis
Prognosis depends on:
- Extent and severity of CAD: Left main or three-vessel disease carries worse prognosis
- LV systolic function: EF is the strongest predictor of mortality
- CCS class: Higher class = more extensive ischemia
- Comorbidities: Diabetes, CKD, peripheral artery disease worsen outcomes
- Response to therapy: Patients well-controlled on optimal medical therapy have excellent long-term outcomes
Annual mortality in stable angina is approximately 1–2%, rising substantially with reduced EF or multi-vessel disease.
11. Conclusion
Angina pectoris is the symptomatic expression of myocardial ischemia and a pivotal clinical marker of underlying coronary artery disease. Its evaluation requires a structured approach — from clinical history and risk stratification through ECG, stress testing, and coronary imaging. Management is multifaceted: aggressive risk factor modification and antiplatelet therapy form the foundation, anti-anginal drugs (led by beta-blockers and nitrates) control symptoms, and revascularization is reserved for refractory symptoms or high-risk anatomy. Recognizing atypical presentations, especially in women and diabetics, is critical to avoid missed diagnoses. With contemporary medical and interventional therapy, most patients with stable angina enjoy a good quality of life and favorable prognosis.
Key References
- Harrison's Principles of Internal Medicine, 21st Edition, pp. 529, 7508
- ACC/AHA Guideline on the Diagnosis and Management of Stable Ischemic Heart Disease
- ESC Guidelines on Chronic Coronary Syndromes (2019)
- ISCHEMIA Trial (NEJM, 2020)
- COURAGE Trial (NEJM, 2007)
- FREEDOM Trial (NEJM, 2012)
cardiac causes of chest pain
search_medical_text
cardiac causes of chest pain differential diagnosis
search_medical_text
pericarditis myocarditis aortic dissection chest pain clinical features
search_medical_image
cardiac chest pain differential ECG findings ischemia pericarditis
GradeResponse
GradeResponse
GradeResponse
Cardiac Causes of Chest Pain
Chest pain is one of the most common and consequential presenting complaints in medicine. Cardiac causes range from immediately life-threatening (STEMI, aortic dissection) to benign (musculoskeletal overlap), and accurate differentiation is critical. The primary goal of initial evaluation is to exclude the most dangerous conditions: Acute Coronary Syndrome (ACS), Acute Aortic Syndrome (AAS), and Acute Pulmonary Embolism (PE) — before considering other etiologies (Non-Invasive Imaging in Coronary Syndromes, p. 14).
Overview: Cardiac Causes at a Glance
| Condition | Pain Character | Location/Radiation | Precipitant | Relief | Key Finding |
|---|---|---|---|---|---|
| Stable Angina | Pressure, heaviness | Substernal → arm/jaw | Exertion | Rest, nitrates | ST depression on stress |
| Unstable Angina / NSTEMI | Same as above, more severe | Substernal → arm/jaw | Rest or minimal exertion | Nitrates (partial) | Elevated troponin (NSTEMI) |
| STEMI | Severe crushing | Substernal → arm/jaw/back | Spontaneous | Not relieved by nitrates | ST elevation, elevated troponin |
| Aortic Dissection | Tearing/ripping, maximal at onset | Anterior chest → back (interscapular) | Hypertension, Marfan | None | Widened mediastinum on CXR |
| Pericarditis | Sharp, pleuritic | Substernal → trapezius ridge | Viral illness | Sitting forward, NSAIDs | Diffuse ST elevation, PR depression |
| Myocarditis | Sharp/dull, variable | Precordial | Viral illness, post-vaccine | Variable | Elevated troponin, MRI LGE |
| Hypertensive Emergency | Dull pressure | Substernal | Severe BP elevation | Antihypertensives | Severely elevated BP |
| Arrhythmias | Palpitations ± chest tightness | Precordial | Variable | Rate control | Abnormal rhythm on ECG |
| Cardiac Tamponade | Dull pressure, dyspnea | Precordial | Trauma, cancer, pericarditis | Pericardiocentesis | Beck's triad, electrical alternans |
1. Acute Coronary Syndrome (ACS)
ACS encompasses Unstable Angina (UA), NSTEMI, and STEMI — a spectrum of plaque rupture with varying degrees of coronary occlusion.
Pathophysiology
Atherosclerotic plaque rupture or erosion triggers platelet aggregation and thrombus formation. In STEMI, complete occlusion causes transmural ischemia. In NSTEMI/UA, partial occlusion causes subendocardial ischemia.
Clinical Features
- Character: Crushing, pressure, heaviness — "like an elephant sitting on my chest"
- Location: Substernal, radiating to left arm, jaw, neck, shoulder, or epigastrium
- Duration: UA/NSTEMI — prolonged (>20 min); STEMI — continuous
- Associated: Diaphoresis, nausea, vomiting, dyspnea, syncope
- Atypical: Women, diabetics, and the elderly may present with jaw pain, fatigue, dyspnea, or epigastric discomfort alone
Diagnosis
- ECG: ST depression / T-wave inversion (UA/NSTEMI); ST elevation ≥1 mm in ≥2 contiguous leads (STEMI); new LBBB
- Troponin: Normal in UA; elevated in NSTEMI/STEMI (high-sensitivity troponin rises within 1–3 hours)
- Imaging: Echocardiography shows regional wall motion abnormalities; coronary angiography is definitive
Management
- Aspirin + P2Y12 inhibitor (clopidogrel, ticagrelor, prasugrel)
- Anticoagulation (heparin, enoxaparin)
- Beta-blockers, nitrates, statins
- Primary PCI within 90 minutes for STEMI (door-to-balloon time)
- Thrombolysis if PCI unavailable within 120 minutes
2. Stable Angina Pectoris
(Discussed in detail separately)
- Fixed coronary stenosis limits flow during exertion
- Predictable, reproducible chest pressure with exertion, relieved by rest or sublingual nitroglycerin within 1–5 minutes
- Managed with anti-anginal therapy, risk factor modification, and revascularization if refractory
3. Acute Aortic Syndrome (Aortic Dissection)
Pathophysiology
A tear in the aortic intima allows blood to track within the media, creating a false lumen. Stanford Type A involves the ascending aorta (surgical emergency); Type B involves the descending aorta only (managed medically unless complicated).
Clinical Features
- Character: Sudden-onset, tearing or ripping pain — maximal intensity at onset (unlike MI, which builds)
- Location: Anterior chest (Type A) or interscapular back (Type B)
- Associated: Pulse differentials between arms (>20 mmHg), new aortic regurgitation murmur, neurological deficits (if carotid involvement), limb ischemia
- Risk factors: Uncontrolled hypertension, Marfan syndrome, bicuspid aortic valve, pregnancy, cocaine use
Diagnosis
- CXR: Widened mediastinum (>8 cm), loss of aortic knuckle — present in ~60%
- CT Aortography: Gold standard; shows intimal flap and true/false lumen
- TEE: Excellent sensitivity; useful intraoperatively
- D-dimer: Negative D-dimer has high NPV to exclude dissection in low-probability cases
Management
- Type A: Emergency surgical repair (mortality ~1–2%/hour if untreated)
- Type B: IV beta-blockade (target HR <60, SBP 100–120 mmHg); endovascular repair (TEVAR) for complications
⚠️ Critical pitfall: Thrombolytics given for a misdiagnosed "STEMI" in aortic dissection can be fatal.
4. Pericarditis
According to the Management of Myocarditis and Pericarditis guidelines (p. 15), pericarditis is an inflammatory pericardial syndrome, with chest pain present in 85–90% of cases.
Clinical Features
- Character: Sharp, pleuritic (worsens with inspiration and swallowing)
- Positional: Worsens lying flat; improves sitting forward (reduces friction between inflamed layers)
- Radiation: To trapezius ridge (pathognomonic — from phrenic nerve irritation)
- Associated: Fever, recent viral illness (Coxsackievirus, Echovirus most common), dyspnea
- Sign: Pericardial friction rub — superficial, scratchy, three-component sound; present in ≤33% of cases
Diagnosis
Requires ≥2 of the following criteria:
- Typical chest pain (pleuritic, positional)
- Pericardial friction rub
- ECG changes (diffuse ST elevation, PR depression)
- New/worsening pericardial effusion on imaging
ECG in Acute Pericarditis:
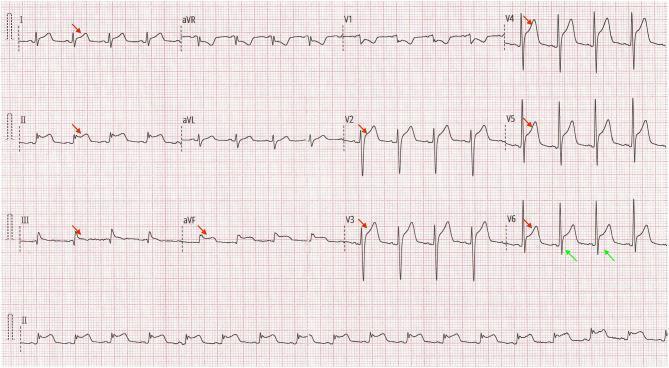
ECG Features (distinguishing pericarditis from STEMI):
| Feature | Pericarditis | STEMI |
|---|---|---|
| ST morphology | Concave (saddle-shaped) upward | Convex (domed) upward |
| Distribution | Diffuse (multiple territories) | Focal (one coronary territory) |
| Reciprocal ST depression | Absent | Present |
| PR depression | Present (especially lead II) | Absent |
| Q waves | Absent | May develop |
| aVR | ST depression + PR elevation | Reciprocal changes |
Lab: Elevated CRP (79–90%), ESR, leukocytosis; troponin may be mildly elevated if myopericarditis
Imaging: Echocardiography for effusion; Cardiac MRI is superior — shows pericardial edema and late gadolinium enhancement (LGE)
Management
- NSAIDs (ibuprofen 600 mg TID or aspirin 750–1000 mg TID) for 1–2 weeks
- Colchicine 0.5 mg BD for 3 months — reduces recurrence by ~50% (COPE and ICAP trials)
- Corticosteroids only for refractory cases, autoimmune etiology, or contraindications to NSAIDs (associated with higher recurrence rates if used empirically)
- Activity restriction until symptom-free and CRP normalized
5. Myocarditis
Pathophysiology
Inflammation of the myocardium, most commonly due to viral infection (Coxsackievirus B, adenovirus, COVID-19, SARS-CoV-2 mRNA vaccine-associated). Immune-mediated myocardial injury leads to necrosis, dysfunction, and arrhythmias.
Clinical Features
- Chest pain (precordial, sharp or dull), often following a viral prodrome (fever, myalgia, upper respiratory symptoms 1–4 weeks prior)
- Dyspnea, palpitations, fatigue
- May present as acute heart failure, cardiogenic shock, or sudden cardiac death in fulminant cases
- Young athletes: myocarditis is a leading cause of sudden cardiac death
Diagnosis
- Troponin: Elevated (degree correlates with extent of necrosis)
- ECG: Sinus tachycardia, non-specific ST-T changes, arrhythmias
- Echocardiography: Reduced EF, wall motion abnormalities, pericardial effusion
- Cardiac MRI (Lake Louise Criteria): Gold standard non-invasive test — myocardial edema (T2 signal), hyperemia, LGE in non-ischemic (mid-wall/epicardial) distribution
- Endomyocardial biopsy: Definitive (Dallas criteria); reserved for hemodynamically unstable or unclear cases
Management
- Supportive: Rest, heart failure therapy (ACE inhibitors, beta-blockers, diuretics)
- Avoid NSAIDs in acute phase (may worsen myocardial injury)
- Immunosuppression for giant cell myocarditis, autoimmune myocarditis
- Mechanical circulatory support (IABP, LVAD, ECMO) for cardiogenic shock
- Activity restriction for 3–6 months; return to sport requires clinical and imaging clearance
6. Cardiac Tamponade
Pathophysiology
Accumulation of fluid in the pericardial space compresses the heart, impairing diastolic filling and reducing cardiac output. As pericardial pressure exceeds diastolic pressure, stroke volume falls precipitously.
Clinical Features — Beck's Triad
- Hypotension
- Elevated JVP (distended neck veins)
- Muffled heart sounds
Additional: Dyspnea, tachycardia, pulsus paradoxus (>10 mmHg drop in SBP during inspiration — classic sign)
Causes: Malignancy (most common in developed countries), post-cardiac surgery, trauma, pericarditis, renal failure, aortic dissection
Diagnosis
- ECG: Sinus tachycardia + electrical alternans (alternating QRS axis — pathognomonic)
- Echocardiography: Diagnostic — pericardial effusion with right atrial/ventricular diastolic collapse, IVC plethora, respiratory variation in valve flows
- CXR: Globular "water bottle" cardiac silhouette
Management
- Pericardiocentesis: Urgent drainage — even 50–100 mL removal can dramatically improve hemodynamics
- Surgical drainage for loculated effusions or recurrence
7. Hypertensive Emergency with Cardiac Involvement
Severely elevated BP (>180/120 mmHg) with target organ damage can cause:
- Hypertensive heart disease: LV hypertrophy → subendocardial ischemia → chest pain
- Acute heart failure/pulmonary edema: Flash pulmonary edema
- Type 2 MI: Demand ischemia from severe pressure overload
Management: IV labetalol, nicardipine, or nitroprusside; target 20–25% BP reduction in the first hour.
8. Arrhythmias
Tachyarrhythmias (SVT, AF with rapid ventricular response, ventricular tachycardia) and severe bradyarrhythmias can cause chest tightness or palpitations by:
- Increasing myocardial oxygen demand (tachycardia)
- Reducing diastolic filling time → decreased coronary perfusion
- Causing demand ischemia in the presence of underlying CAD
Presentation: Palpitations with chest tightness, dyspnea, presyncope
Diagnosis: ECG, Holter monitor, event recorder
Management: Rate/rhythm control per specific arrhythmia
9. Valvular Heart Disease
| Condition | Chest Pain Mechanism | Key Features |
|---|---|---|
| Severe Aortic Stenosis | Angina from subendocardial ischemia (LVH + high demand) | Crescendo-decrescendo murmur, syncope, exertional dyspnea; triad: angina, syncope, heart failure |
| Hypertrophic Cardiomyopathy (HCM) | LV outflow obstruction + microvascular ischemia | Young athlete, family history, dynamic murmur, sudden death risk |
| Mitral Valve Prolapse | Atypical chest pain (mechanism debated — papillary muscle tension) | Mid-systolic click + late systolic murmur |
10. Approach to the Patient with Cardiac Chest Pain
CHEST PAIN
|
├── Hemodynamically unstable? → Immediate resuscitation (IV access, O2, ECG, echo)
|
├── STEMI on ECG? → Activate cath lab → Primary PCI
|
├── Tearing pain + pulse differential → CT Aortography for Aortic Dissection
|
├── Pleuritic + positional + friction rub → Pericarditis workup
|
├── Post-viral + elevated troponin + young patient → Myocarditis (Cardiac MRI)
|
├── Elevated troponin + ST/T changes (no ST elevation) → NSTEMI → Coronary angiography
|
├── Exertional + relieved by nitrates → Stable Angina → Stress testing
|
└── Beck's triad + electrical alternans → Tamponade → Urgent pericardiocentesis
Key Investigations Summary
| Test | Key Finding | Condition |
|---|---|---|
| ECG | ST elevation (convex, focal) | STEMI |
| ECG | ST elevation (concave, diffuse) + PR depression | Pericarditis |
| ECG | Electrical alternans | Tamponade |
| Troponin ↑ | Myocardial necrosis | ACS, myocarditis |
| CXR | Widened mediastinum | Aortic dissection |
| CXR | "Water bottle" heart | Tamponade |
| Echo | Wall motion abnormality | ACS |
| Echo | Pericardial effusion + RV collapse | Tamponade |
| CT Aortography | Intimal flap | Aortic dissection |
| Cardiac MRI | LGE (non-ischemic pattern) | Myocarditis |
Key References
- Non-Invasive Imaging in Coronary Syndromes, p. 14
- Management of Myocarditis and Pericarditis (ESC Guidelines), p. 15
- Harrison's Principles of Internal Medicine, 21st Edition
- ESC Guidelines on Acute Coronary Syndromes (2023)
- ESC Guidelines on Aortic Diseases (2014/2024 update)
This is a shared conversation. Sign in to Orris to start your own chat.