Erythropoietin management
Reading File
Finding Sources
Searching PubMed
"erythropoietin" AND "management"
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to write a thorough answer. Let me compile everything.
Erythropoietin (EPO) - Comprehensive Clinical Management
Physiology & Mechanism
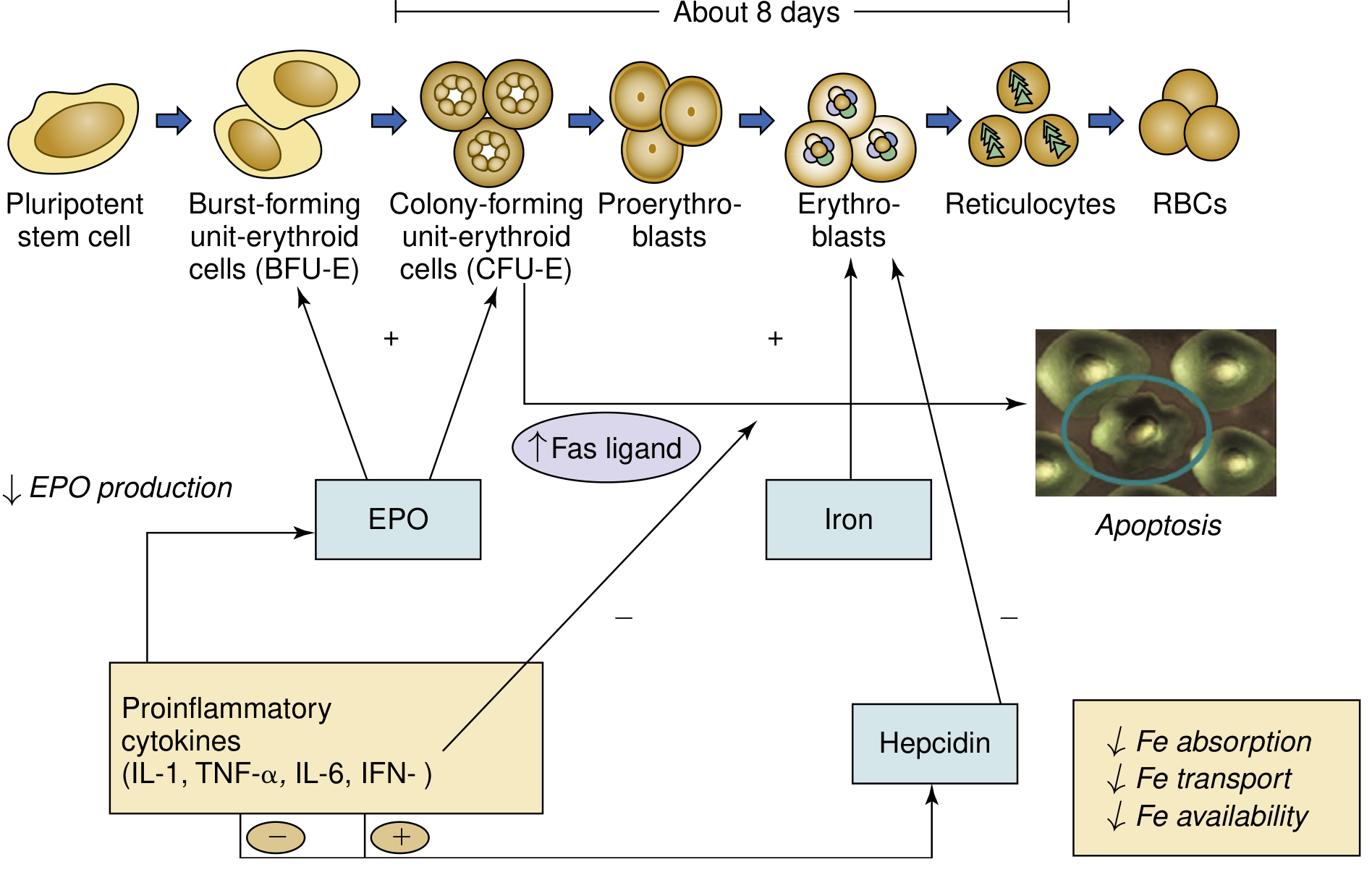
Erythropoietin (EPO) is a 30.4 kDa glycoprotein hormone produced primarily by peritubular interstitial fibroblasts in the renal cortex. It is the master regulator of erythropoiesis.
Oxygen-sensing / HIF pathway:
- Under normoxia, HIF-alpha subunits (1α, 2α, 3α) are constitutively produced but rapidly degraded via prolyl hydroxylases (PHDs) and the ubiquitin-proteasome pathway.
- Under hypoxia, PHD activity falls, HIF-alpha escapes degradation, dimerizes with HIF-beta, and binds hypoxia-responsive elements (HREs) in the EPO gene, dramatically increasing EPO transcription (up to 100-fold increase with severe anemia).
- EPO then binds receptors on committed erythroid progenitors (CFU-E and BFU-E), signaling via the JAK2/STAT5 pathway to promote proliferation, differentiation, and reticulocyte release.
Normal EPO levels: <20 IU/L in nonanemic individuals. With moderate-severe anemia, levels rise to 100-500 IU/L or even thousands IU/L - except in chronic kidney disease where levels are inappropriately low.
Available Erythropoiesis-Stimulating Agents (ESAs)
| Agent | Half-life | Dosing frequency | Route |
|---|---|---|---|
| Epoetin alfa (Epogen, Procrit) | 4-13 h (IV) | 3x/week | IV or SC |
| Darbepoetin alfa (Aranesp) | 2-3x longer than epoetin | Weekly | SC (or IV) |
| Methoxy-PEG-epoetin beta (Mircera) | Very long (pegylated) | Every 2 weeks or monthly | IV or SC |
| Epoetin alfa-ebpx (Retacrit) | Same as epoetin alfa | 3x/week | IV or SC |
- Darbepoetin alfa has additional N-linked oligosaccharide chains (amino acid substitutions) compared to endogenous EPO, extending its half-life.
- Methoxy-PEG-epoetin beta is epoetin covalently attached to a long polyethylene glycol polymer; should NOT be used for chemotherapy-related anemia (increased mortality in one trial).
- Biosimilar ESAs (e.g., Retacrit) are FDA-approved after demonstrating structural/functional similarity to the reference product.
- Katzung's Basic & Clinical Pharmacology, 16e; NKF Primer on Kidney Diseases, 8e
Clinical Indications
- Anemia of chronic kidney disease (CKD) - the primary and best-established use
- HIV infection treated with zidovudine - zidovudine suppresses erythropoiesis; EPO levels <500 IU/L predict response
- Cancer chemotherapy-related anemia - when Hb <10 g/dL; use conservatively, lowest effective dose; only when non-curative intent
- Elective (non-cardiac, non-vascular) surgery - to reduce transfusion requirements in eligible patients
- Low-risk myelodysplastic syndrome - for transfusion-dependent patients with disproportionately low EPO levels
- Porphyria cutanea tarda with renal failure - EPO may be combined with phlebotomy
Key predictor of response: Endogenous EPO levels <100 IU/L respond best; 100-500 IU/L respond occasionally; levels >500 IU/L are unlikely to respond to exogenous ESA.
- Katzung's Basic & Clinical Pharmacology, 16e; Goldman-Cecil Medicine
Management in CKD (Most Common Context)
Screening and Diagnosis
Per the 2012 KDIGO Anemia in CKD Guidelines:
- Screen CKD stage 3 at least annually; more frequently with advancing CKD
- Monthly Hb monitoring in maintenance dialysis patients
- Anemia defined as: Hb <13.0 g/dL in adult men, Hb <12.0 g/dL in adult women
- Evaluation: CBC with indices, reticulocyte count, serum ferritin, transferrin saturation (TSAT) or reticulocyte Hb content (CHr)
The anemia of EPO deficiency is normocytic and normochromic (normal MCV and MCHC).
Iron Assessment Before and During ESA Therapy
Iron deficiency is the most common cause of ESA hyporesponsiveness. Two types:
- Absolute iron deficiency: Low TSAT (<20%) + ferritin <25 ng/mL (men) or <12 ng/mL (women); treat with IV or oral iron first
- Functional iron deficiency: Low TSAT but normal/high ferritin - often due to pharmacologically stimulated erythropoiesis outpacing iron release from reticuloendothelial stores, or hepcidin-mediated blockade in inflammation. Responds to IV iron.
- If low TSAT + normal/high ferritin does NOT respond to IV iron: presume RE blockade (hepcidin-mediated)
Target Hemoglobin
- Current consensus (KDIGO): Individualize targets; generally maintain Hb in the 10-11.5 g/dL range
- Do NOT use ESAs to target Hb >13 g/dL - associated with increased risk of stroke, cardiovascular events, thromboembolism, and mortality
- Do NOT exceed 11 g/dL in patients with prior stroke or active malignancy
Typical Starting Doses
- Epoetin alfa: 50-100 IU/kg SC three times per week; NDD-CKD and peritoneal dialysis patients typically receive SC
- Darbepoetin alfa: 0.45 mcg/kg SC/IV weekly, or 0.75 mcg/kg every 2 weeks
- Mircera: 0.6 mcg/kg IV/SC every 2 weeks initially, then monthly once stable
Expect reticulocyte count increase in ~10 days; Hb rise in 2-6 weeks.
Doses are titrated by ~25% increments. If Hb rises >1 g/dL over 2 weeks, reduce dose by 25%. If no response after 4 weeks, increase by 25%.
- Katzung's Basic & Clinical Pharmacology, 16e; NKF Primer on Kidney Diseases, 8e; Brenner & Rector's The Kidney
Causes of ESA Hyporesponsiveness
When a patient on ESA fails to reach target Hb despite adequate doses, investigate:
- Iron deficiency (most common) - absolute or functional
- Inflammation / infection - cytokines suppress EPO effect and iron availability via hepcidin
- Inadequate dialysis - uremic toxins blunt marrow response
- Hyperparathyroidism - PTH suppresses erythropoiesis
- Aluminum toxicity - in dialysis patients
- Vitamin B12 / folate deficiency
- Pure red cell aplasia (PRCA) - anti-EPO antibodies (see below)
- Occult blood loss
- Hemolysis
- Bone marrow disorders (e.g., myelodysplasia, infiltration)
Adverse Effects
| Effect | Details |
|---|---|
| Hypertension | Most common; monitor BP; may require antihypertensive initiation or dose adjustment |
| Thromboembolism | Increased risk of DVT, PE, arteriovenous access thrombosis; especially with Hb >11 g/dL |
| Cardiovascular events / stroke | Increased in trials targeting higher Hb (>13 g/dL) |
| Pure Red Cell Aplasia (PRCA) | Rare but serious; anti-EPO antibodies; sudden drop in Hb ~1 g/dL/week, reticulocyte count <20,000/µL despite high ESA dose; confirm by anti-EPO antibody testing or bone marrow biopsy (<4% erythroblasts) |
| Allergic reactions | Infrequent |
PRCA Management: Discontinue ESA immediately + immunosuppressive therapy (e.g., cyclophosphamide). Most patients respond over several months. Switching to a different ESA is contraindicated due to cross-reactivity of antibodies.
- Katzung's Basic & Clinical Pharmacology, 16e; NKF Primer on Kidney Diseases, 8e
Emerging Therapy: HIF-PHD Inhibitors
PHD (prolyl hydroxylase domain) inhibitors (e.g., roxadustat, daprodustat, vadadustat) work by blocking PHD enzymes, stabilizing HIF-alpha, and stimulating endogenous EPO production. They also suppress hepcidin, improving iron availability. Roxadustat is approved in several countries (Japan, China, EU) for CKD anemia, but has faced regulatory scrutiny regarding cardiovascular safety in the US. These agents offer oral administration as an advantage over injectable ESAs.
- Katzung's Basic & Clinical Pharmacology, 16e
Blood Doping (Athletic Misuse)
EPO is widely misused by endurance athletes to increase oxygen-carrying capacity. Doping with EPO poses serious health risks (polycythemia, hyperviscosity, thrombosis) and is banned by all major sporting bodies and routinely tested for. Blood doping via autologous transfusion or androgens is used similarly.
Recent Evidence (2024-2025)
- A 2024 systematic review [PMID: 39533400] examined factors contributing to post-kidney transplant anemia and effects of ESAs - confirming that ESA use remains relevant even after transplantation.
- A 2025 systematic review [PMID: 39913688] reviewed drug-induced erythrocytosis, noting that ESA and PHD inhibitor misuse/overuse is an emerging concern.
- Iron management optimization in dialysis patients continues to be refined (systematic review, 2024, PMID: 39664943), with IV iron shown to reduce ESA requirements and improve outcomes.
Key References:
- Katzung's Basic & Clinical Pharmacology, 16th Edition (Hematopoietic Growth Factors chapter)
- Goodman & Gilman's Pharmacological Basis of Therapeutics (Hematopoietic Agents chapter)
- NKF Primer on Kidney Diseases, 8th Edition (Chapter 55 - Anemia in CKD)
- Brenner & Rector's The Kidney (Erythropoietin chapter)
This is a shared conversation. Sign in to Orris to start your own chat.