what is happening in parts wave which muscles contracts and what events occur there
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a thorough, well-sourced answer. Here is the complete breakdown:
The P Wave - What Is Happening, Which Muscles Contract, and What Events Occur
What Is the P Wave?
The P wave is the first deflection on the ECG and represents atrial depolarization - the electrical activation that sweeps across the atria just before they contract. It is a small, rounded, upright wave (0.1-0.3 mV in amplitude) and lasts roughly 0.08-0.10 seconds.
"The P wave is caused by electrical potentials generated when the atria depolarize before atrial contraction begins."
- Guyton and Hall Textbook of Medical Physiology
Which Muscles Contract During the P Wave?
The right and left atrial myocardium (atrial muscle) contracts during and immediately after the P wave. Specifically:
- Right atrium is activated first (early part of the P wave), because the SA node sits at the junction of the right atrium and the superior vena cava
- Left atrium is activated slightly later (latter part of the P wave), as the impulse spreads across both atria via internodal pathways and Bachmann's bundle
- The ventricular muscle does NOT contract during the P wave - this is the key distinction. Ventricular contraction is triggered by the QRS complex, which follows later
Sequence of Events During the P Wave
Here is the full sequence in order:
1. SA Node Fires (Pacemaker Discharge)
The sinoatrial (SA) node - located near the entry of the superior vena cava into the right atrium - spontaneously reaches threshold and fires an action potential. This is the "spark" that starts the cardiac cycle.
2. Electrical Impulse Spreads Across Both Atria
- Depolarization begins at the SA node and spreads in all directions across the atria through gap junctions and specialized internodal pathways
- The direction of spread is generally from the upper right atrium (SA node region) downward and to the left, toward the AV node
- Because this direction aligns with the positive axes of standard limb leads I, II, and III, the P wave is normally upright (positive) in leads I, II, and III
3. Atrial Muscle Depolarizes (= P Wave on ECG)
As the wave of depolarization spreads from cell to cell across the atrial walls:
- The normal resting negative membrane potential inside the atrial cells reverses (inside becomes positive, outside becomes negative)
- This electrical event is what the ECG records as the P wave
"Depolarization of the atria begins in the sinus node and spreads in all directions over the atria. This record of atrial depolarization is known as the atrial P wave."
- Guyton and Hall Textbook of Medical Physiology, p. 155
4. Atrial Systole (Atrial Contraction) - "Atrial Kick"
- Immediately after depolarization sweeps through the atrial muscle, atrial contraction (systole) follows
- Both atria contract, squeezing blood through the open AV valves (mitral and tricuspid) into the ventricles
- This final push of blood into the ventricles accounts for roughly 20-25% of the total ventricular filling (the "atrial kick")
- Left atrial contraction causes a rise in left atrial pressure, which appears as the "a wave" on the jugular venous pulse (JVP) trace
"Atrial systole is atrial contraction. It is preceded by the P wave on the ECG, which marks depolarization of the atria. Contraction of the left atrium causes an increase in left atrial pressure."
- Costanzo Physiology, 7th Edition
5. The PR Interval (Delay at AV Node)
- After the P wave ends, there is the PR interval - a brief pause (~0.12-0.20 sec)
- The electrical impulse arrives at the AV node and is deliberately delayed there, giving the atria time to finish contracting and fill the ventricles before ventricular contraction begins
- This delay is NOT reflected in the P wave itself, but in the flat PR segment that follows it
Summary Table
| Event | ECG Marker | What Contracts |
|---|---|---|
| SA node fires | Start of P wave | Nothing yet |
| Atrial depolarization spreads | P wave | Atrial muscle (R then L atrium) |
| Atrial contraction (systole) | During/after P wave | Both atria |
| AV node delay | PR segment | Nothing |
| Ventricular depolarization | QRS complex | Ventricular muscle |
Diagram: Atrial Depolarization and the P Wave
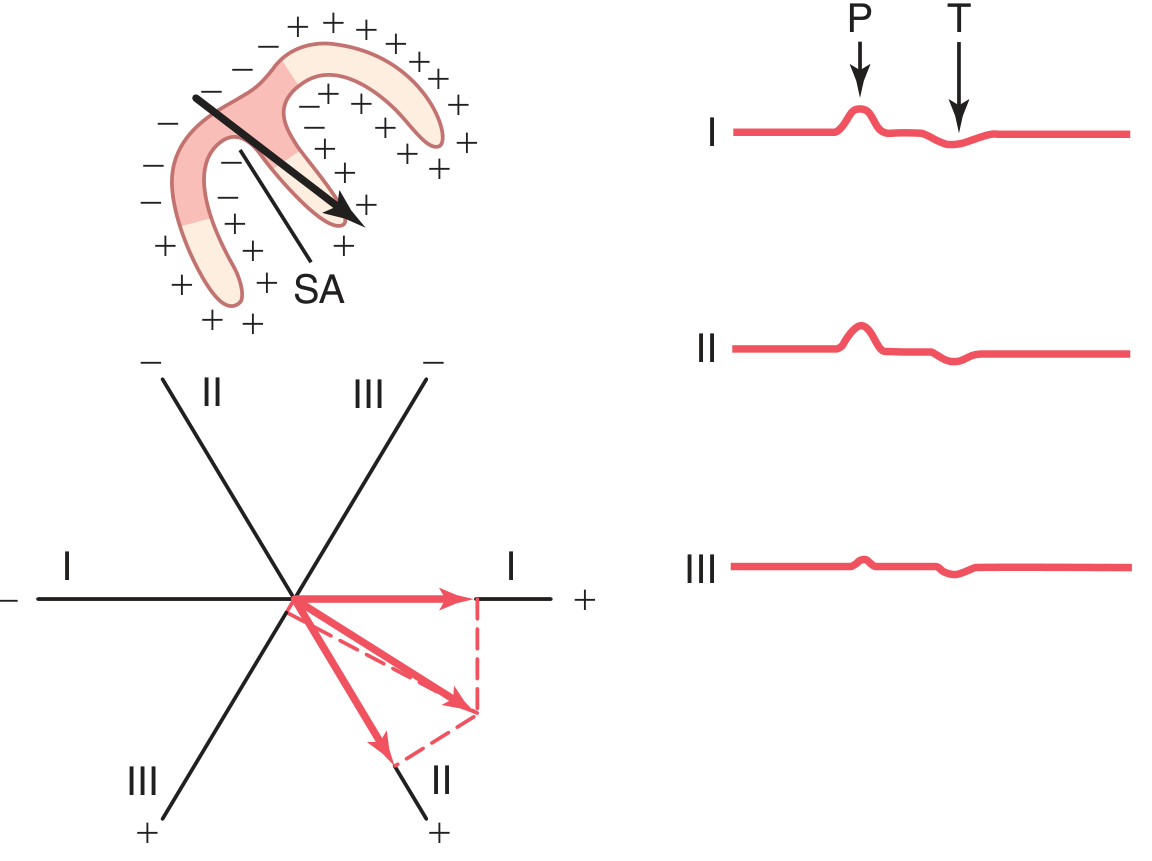
The above diagram (from Guyton & Hall) shows: (top left) the atria with the SA node initiating depolarization spreading in all directions; (bottom left) the mean vector direction; (right) the resulting P wave shape in leads I, II, and III - all upright and positive.
Key Points to Remember
| Feature | Detail |
|---|---|
| Origin | SA node (right atrium, near SVC) |
| Muscle contracting | Both atria (right first, then left) |
| Duration of P wave | 0.08-0.10 seconds (<0.12 sec is normal) |
| Voltage | 0.1-0.3 mV |
| Direction | Positive (upright) in leads I, II, III; inverted in aVR |
| What follows | PR interval (AV nodal delay) then QRS (ventricular depolarization) |
| Atrial repolarization | Occurs during the QRS complex - the "atrial T wave" is hidden/buried within it |
| S4 heart sound | Occurs during atrial contraction (P wave) - audible in stiff ventricles |
Sources: Guyton and Hall Textbook of Medical Physiology (p. 144, 155) | Costanzo Physiology, 7th Edition (p. 161) | Tietz Textbook of Laboratory Medicine, 7th Edition
What happens in parts wave
Asking for Preferences
Pqrst
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete breakdown of all PQRST waves on the ECG:
PQRST Waves of the ECG - Complete Guide

P Wave
What it represents: Atrial depolarization
| Feature | Detail |
|---|---|
| Origin | SA node fires spontaneously |
| Electrical event | Depolarization spreads across both atria (right first, then left) |
| Mechanical event | Atrial contraction (atrial systole) follows immediately after |
| Which muscle contracts | Right and left atrial myocardium |
| Normal duration | < 0.12 sec (120 ms) |
| Normal amplitude | 0.1 - 0.3 mV |
| Direction | Upright (positive) in leads I, II, III; inverted in aVR |
"The P wave is caused by electrical potentials generated when the atria depolarize before atrial contraction begins."
- Guyton and Hall Textbook of Medical Physiology
PR Interval (not a wave, but important)
What it represents: Time from start of atrial depolarization to start of ventricular depolarization
- Includes the delay at the AV node - this pause allows atria to finish contracting before ventricles begin
- Normal: 120-200 ms (0.12 - 0.20 sec)
- Prolonged PR = heart block; short PR = pre-excitation (e.g., WPW syndrome)
Q Wave
What it represents: First downward (negative) deflection of the QRS complex
| Feature | Detail |
|---|---|
| Electrical event | Initial ventricular septal depolarization (left to right) |
| Normal | Small and narrow (< 0.04 sec, < 25% of R wave height) |
| Abnormal deep Q | Indicates old myocardial infarction (dead tissue = no depolarization) |
R Wave
What it represents: First upward (positive) deflection of the QRS complex
| Feature | Detail |
|---|---|
| Electrical event | Main ventricular depolarization - the large muscle mass of both ventricles depolarizing |
| Which muscle | Left and right ventricular myocardium (left ventricle dominates) |
| Normal | Tallest peak of the QRS complex |
| R wave progression | Gets taller from V1 to V5 across chest leads (normal) |
S Wave
What it represents: Downward deflection after the R wave
| Feature | Detail |
|---|---|
| Electrical event | Terminal ventricular depolarization (basal portions of ventricles) |
| Direction | Negative (downward) deflection |
"The QRS complex is caused by potentials generated when the ventricles depolarize before contraction - that is, as the depolarization wave spreads through the ventricles."
- Guyton and Hall Textbook of Medical Physiology
Key fact: The QRS complex looks narrow (similar duration to P wave) despite the ventricles being much larger than atria - because the His-Purkinje system conducts the impulse extremely fast, allowing near-simultaneous activation of the entire ventricular mass. - Costanzo Physiology, 7th Edition
ST Segment (between S and T)
What it represents: The period when all ventricular muscle is fully depolarized
| Feature | Detail |
|---|---|
| Electrical event | Corresponds to Phase 2 (plateau) of the ventricular action potential - all cells are equally depolarized |
| Mechanical event | Ventricular ejection (systole) is occurring - blood being pumped into aorta and pulmonary trunk |
| Normal | Isoelectric (flat, on the baseline) |
| ST elevation | Acute MI (STEMI), pericarditis |
| ST depression | Ischemia, subendocardial infarction |
T Wave
What it represents: Ventricular repolarization
| Feature | Detail |
|---|---|
| Electrical event | Ventricles recovering from depolarization (Phase 3 of action potential) |
| Mechanical event | Ventricles beginning to relax |
| Which muscle | Ventricular myocardium repolarizing (epicardium first) |
| Normal duration | 0.25 - 0.35 sec after depolarization |
| Direction | Normally upright (same direction as QRS) |
| Tall peaked T | Hyperkalemia |
| Inverted T | Ischemia, ventricular hypertrophy, bundle branch block |
"The T wave is caused by potentials generated as the ventricles recover from depolarization... The T wave is known as a repolarization wave."
- Guyton and Hall Textbook of Medical Physiology
Important: The ventricular T wave repolarizes from epicardium inward (opposite to depolarization direction) - this is why the T wave is normally in the SAME direction as the QRS, not opposite.
U Wave (bonus - sometimes seen)
What it represents: Late ventricular repolarization
- Follows the T wave; small and not always visible
- Prominent U waves are seen in hypokalemia
- May represent repolarization of the Purkinje fibers or mid-myocardial (M) cells
Master Summary Table
| Wave/Segment | Electrical Event | Mechanical Event | Muscle Involved |
|---|---|---|---|
| P wave | Atrial depolarization | Atrial contraction | Both atria |
| PR interval | AV node delay | Atria finishing contraction | AV node (no muscle) |
| Q wave | Septal depolarization (L→R) | Ventricular contraction begins | Interventricular septum |
| R wave | Main ventricular depolarization | Isovolumetric contraction → ejection | Both ventricles |
| S wave | Terminal ventricular depolarization | Ventricular ejection | Basal ventricles |
| ST segment | All ventricles fully depolarized (plateau) | Ventricular ejection (systole) | All ventricular muscle |
| T wave | Ventricular repolarization | Ventricular relaxation begins | Both ventricles |
| U wave | Late repolarization | Late ventricular relaxation | Purkinje/M cells |
What Happens to Atrial Repolarization?
Atrial repolarization (the "atrial T wave") does occur but is hidden inside the QRS complex - it happens at the same time and is buried by the much larger ventricular signal. It is only visible in certain conditions like acute pericarditis or AV block.
Sources: Guyton and Hall Textbook of Medical Physiology (p. 143-144) | Harrison's Principles of Internal Medicine 22E (p. 1912) | Costanzo Physiology, 7th Edition (p. 149)
Anatomy of digestion
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I have everything needed for a thorough answer. Here is the complete anatomy of digestion:
Anatomy of Digestion
Overview
The digestive system has four main components:
- GI tract - esophagus, stomach, small intestine, large intestine
- Liver and gallbladder - reside within the peritoneum
- Pancreas - primarily retroperitoneal (except its tail)
- Accessory structures - salivary glands, teeth, tongue
"The digestive system consists of four components: the GI tract, the liver and gallbladder that reside within the peritoneum, as well as the pancreas, that primarily resides in the retroperitoneal space."
- Miller's Anesthesia, 10th Edition
The Wall of the GI Tract - 4 Layers (Inside to Outside)
Every part of the GI tract shares the same fundamental 4-layer structure:
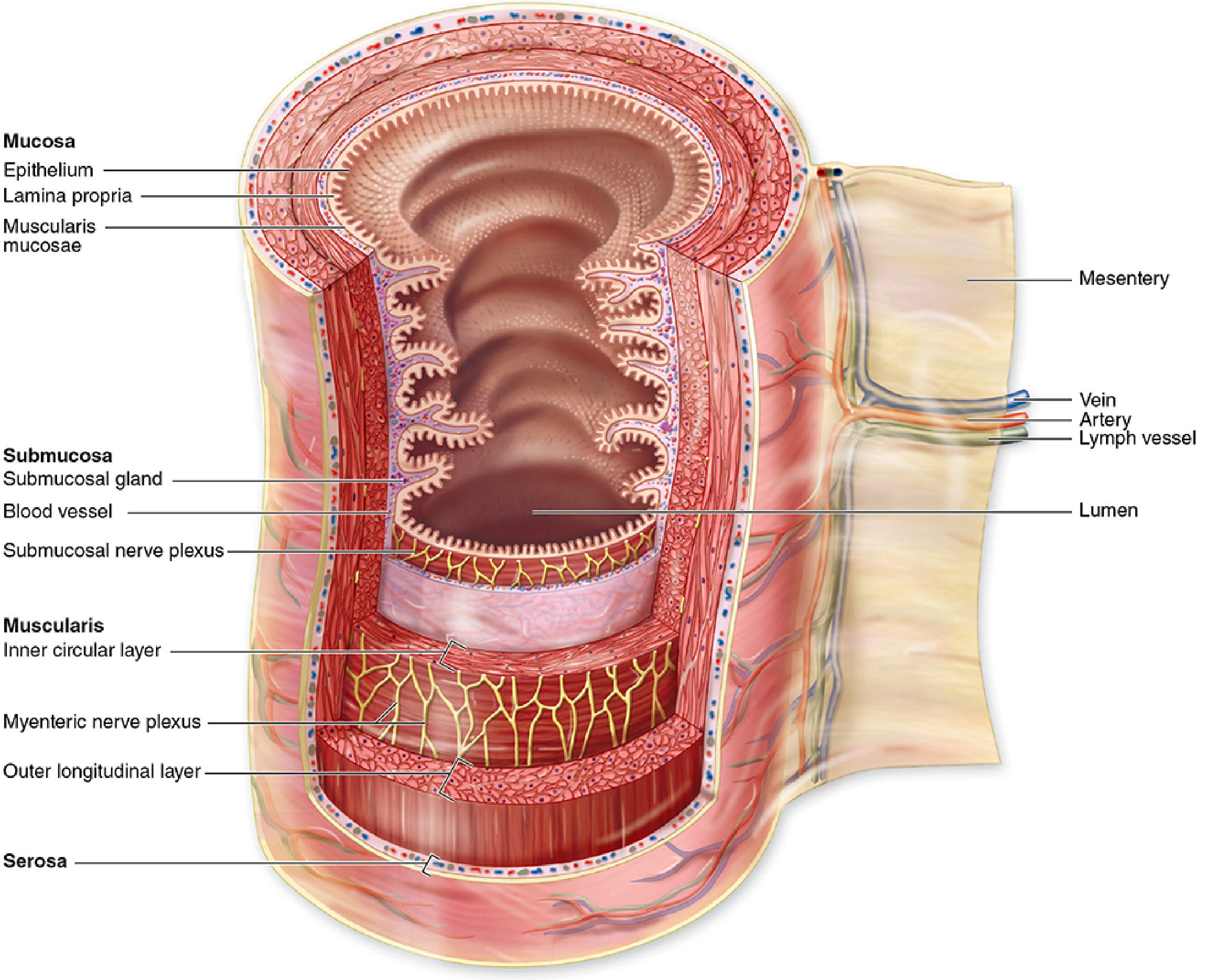
1. Mucosa (innermost layer)
- Epithelium - lines the lumen directly; absorbs nutrients, secrets enzymes, senses contents
- Lamina propria - loose connective tissue containing blood vessels, lymphatics, nerve endings, immune cells
- Muscularis mucosae - thin smooth muscle layer; moves villi and folds the mucosa
2. Submucosa
- Dense connective tissue with larger blood vessels and lymphatics
- Contains Meissner's plexus (submucosal plexus) - transmits sensory information from the epithelium to the enteric and central nervous systems
- May contain glands (e.g., Brunner's glands in the duodenum) and lymphoid tissue
3. Muscularis (Muscularis Externa)
- Two smooth muscle sublayers:
- Inner circular layer - contracts to narrow the lumen
- Outer longitudinal layer - contracts to shorten the segment
- Auerbach's myenteric plexus sits between these two layers - it generates and coordinates peristalsis and mixing contractions
4. Serosa (outermost layer)
- Thin smooth membrane of connective tissue covered by mesothelium (simple squamous epithelium)
- Secretes serous fluid to reduce friction
- Continuous with the mesentery (suspends the intestines in the abdomen and carries blood vessels, nerves, and lymphatics)
- Regions not suspended in the abdomen (e.g., esophagus) have an adventitia instead of serosa
"All regions of the GI tract have certain structural features in common. A hollow tube with a variable diameter lumen, the tract's wall has four main layers: the mucosa, submucosa, muscularis, and serosa."
- Junqueira's Basic Histology, 17th Edition
Organs of the Digestive Tract - Structure & Function
1. Mouth (Oral Cavity)
- Teeth - mechanical breakdown of food (mastication)
- Tongue - manipulates food, contains taste buds
- Salivary glands (parotid, submandibular, sublingual) - produce saliva containing:
- Salivary amylase - begins starch digestion
- Mucus - lubricates the food bolus
- Food is formed into a bolus and swallowed
2. Pharynx & Esophagus
- Esophagus - muscular tube ~18-25 cm long, connecting pharynx to stomach
- Extends from C6 (hypopharynx) to T11 (gastroesophageal junction)
- Three regions:
- Cervical esophagus (~4-5 cm) - surrounded by trachea anteriorly, vertebrae posteriorly
- Thoracic esophagus - runs posterior to trachea, deviates right at aortic arch
- Abdominal esophagus - from diaphragmatic hiatus to stomach cardia
- Upper 1/3 = striated muscle, lower 2/3 = smooth muscle
- Lower esophageal sphincter (LES) - relaxes to allow food into the stomach
- Function: propels food to the stomach via peristalsis - no digestion occurs here
3. Stomach
- J-shaped muscular organ with four regions:
- Cardia - where esophagus connects
- Fundus - upper dome-shaped region (stores gas)
- Body (corpus) - main secretory region
- Pylorus/Antrum - lower region; mixes food and controls gastric emptying via pyloric sphincter
- Rugae - large mucosal folds that allow expansion
- Gastric wall has an extra oblique muscle layer (3 layers total) for churning
- Key secretions:
- Parietal cells → HCl (acid; denatures proteins, kills bacteria) + Intrinsic factor (needed for Vitamin B12 absorption)
- Chief cells → Pepsinogen (converted to pepsin by acid; digests proteins)
- Mucous cells → Mucus (protects stomach lining from acid)
- G cells → Gastrin (hormone that stimulates acid secretion)
- Function: mechanical churning + chemical digestion of proteins; produces chyme
4. Small Intestine (~6-7 meters long)
The primary site of digestion and absorption. Divided into three parts:
| Part | Length | Key Features |
|---|---|---|
| Duodenum | ~25 cm (C-shaped) | Receives bile + pancreatic juice; most digestion begins here |
| Jejunum | ~2.5 m | Primary site of nutrient absorption; tall villi, many circular folds (plicae circulares) |
| Ileum | ~3.5 m | Absorbs bile salts and Vitamin B12; ends at ileocecal valve |
Surface area adaptations - small intestine has three anatomical features that increase absorptive surface area ~600-fold:
- Plicae circulares (circular folds) - permanent folds of mucosa and submucosa
- Villi - finger-like projections of mucosa (~0.5-1.5 mm tall); contain a central lacteal (lymphatic) and capillary network
- Microvilli (brush border) - tiny projections on each enterocyte; contain digestive enzymes (lactase, sucrase, maltase, peptidases)
Blood supply: Celiac artery (duodenum) and superior mesenteric artery (rest of small intestine)
5. Large Intestine (~1.5 meters long)
Parts (in order):
- Cecum + Appendix - blind pouch at the junction with ileum
- Ascending colon - right side, travels upward
- Transverse colon - crosses the abdomen
- Descending colon - left side, travels downward
- Sigmoid colon - S-shaped, leads to rectum
- Rectum - stores feces before defecation
- Anal canal - internal sphincter (smooth, involuntary) + external sphincter (skeletal, voluntary)
Key features:
- Haustra - sac-like pouches caused by the teniae coli (3 longitudinal muscle bands)
- Teniae coli - three bands of outer longitudinal muscle (instead of a complete layer)
- No villi (no major absorption of nutrients)
- Absorbs water, sodium, and potassium; forms and stores feces
- Houses gut microbiome
Blood supply: Superior mesenteric artery (cecum to mid-transverse colon) and inferior mesenteric artery (distal colon to rectum)
6. Liver
- Largest solid organ; adult weight 600-1800 g (2-2.5% of body weight)
- Divided into 8 functional segments (Couinaud system) based on portal vein and hepatic vein distribution
- Right and left hemi-livers divided at the middle hepatic vein
- Dual blood supply:
- Portal vein (75%) - nutrient-rich blood from GI tract
- Hepatic artery (25%) - oxygenated blood
- Key digestive function: produces bile (stored in gallbladder)
- Bile contains bile salts that emulsify fats in the small intestine, enabling lipid absorption
7. Gallbladder
- Small pear-shaped sac on the undersurface of the liver
- Stores and concentrates bile (concentrates ~5-fold) between meals
- Releases bile into the duodenum via the common bile duct when stimulated by CCK (cholecystokinin) after a fatty meal
8. Pancreas
- Primarily retroperitoneal (except the tail which touches the spleen)
- Parts: head (in C-curve of duodenum), neck, body, tail
- Exocrine function (95% of tissue): acinar cells secrete pancreatic juice into the duodenum via the pancreatic duct:
- Proteases (trypsinogen, chymotrypsinogen) - protein digestion
- Lipase - fat digestion
- Amylase - carbohydrate digestion
- Bicarbonate - neutralizes stomach acid in duodenum
- Endocrine function (islets of Langerhans): insulin, glucagon, somatostatin
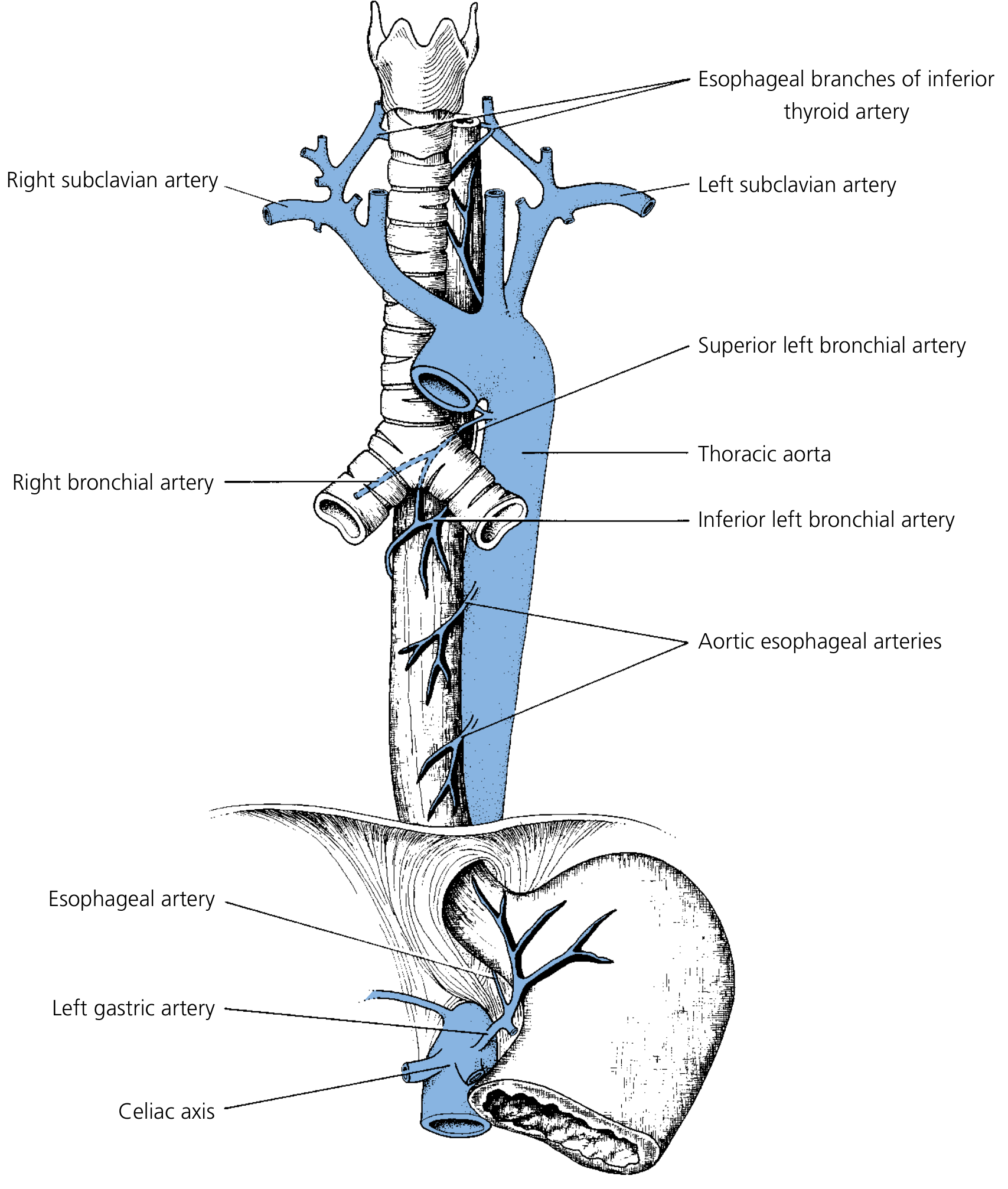
Blood Supply Summary
| Organ | Arterial Supply | Venous Drainage |
|---|---|---|
| Cervical esophagus | Inferior thyroid artery | Superior vena cava |
| Thoracic esophagus | Aortic esophageal arteries | Azygos vein |
| Stomach | Celiac artery | Portal vein |
| Small intestine | Superior mesenteric artery | Portal vein |
| Proximal colon | Superior mesenteric artery | Portal vein |
| Distal colon/rectum | Inferior mesenteric artery | Portal vein |
Key principle: Venous drainage of the entire gut goes to the portal vein → liver, allowing the liver to process all absorbed nutrients before they reach systemic circulation. This is called the hepatic portal circulation.
Digestion and Absorption Summary
| Nutrient | Digestion Starts | Main Absorption Site | Mechanism |
|---|---|---|---|
| Carbohydrates | Mouth (amylase) | Small intestine | Na⁺-glucose cotransport |
| Proteins | Stomach (pepsin) | Small intestine | Na⁺-amino acid cotransport |
| Fats | Small intestine (lipase) | Small intestine | Micelle formation + diffusion; chylomicrons → lymph |
| Vitamin B12 | - | Ileum | Intrinsic factor required |
| Water/Electrolytes | - | Small + large intestine | Active transport / osmosis |
| Iron | - | Duodenum/jejunum | Binds apoferritin → transferrin |
"Digestion is the chemical breakdown of ingested foods into absorbable molecules... Absorption is the movement of nutrients, water, and electrolytes from the lumen of the intestine into the blood."
- Costanzo Physiology, 7th Edition
Sources: Miller's Anesthesia, 10th Edition | Junqueira's Basic Histology, 17th Edition | Costanzo Physiology, 7th Edition | Guyton and Hall Textbook of Medical Physiology
Pharynzx
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information for a thorough answer. Let me compile everything:
Anatomy of the Pharynx
Overview
The pharynx is a 12-14 cm long inverted cone-shaped musculofascial tube that hangs from the pharyngeal tubercle at the base of the skull and fuses with the esophagus below at the level of the lower border of the cricoid cartilage (C6 vertebral level).
It is the common aerodigestive pathway shared by both the respiratory and digestive systems. Its mucosal lining is continuous with the:
- Auditory (Eustachian) tubes
- Nasal cavity
- Oral cavity
- Larynx
Functions:
- Directs air into the laryngeal inlet (respiration)
- Directs food into the esophagus (deglutition/swallowing)
- Assists in pressure equalization in the middle ear (via auditory tube)
- Aids in vocalization and speech
Subdivisions of the Pharynx
The pharynx is divided into three parts based on their anterior communications:
1. Nasopharynx
Boundaries:
- Superior/Roof: Body of sphenoid + basilar occipital bone (basisphenoid)
- Anterior: Choanae (posterior nasal apertures), separated by the vomer
- Lateral walls: Superior constrictor muscle + pharyngotympanic (Eustachian) tube orifice
- Floor: Soft palate
- Inferior: Communicates with oropharynx via the pharyngeal isthmus (behind the soft palate)
Key features:
- Walls are rigid and bony (except the soft palate floor) - always patent for unhindered airflow
- Contains the pharyngotympanic (Eustachian) tube opening - ~1-1.5 cm from the posterior end of the inferior turbinate; connects the middle ear to the nasopharynx to equalize pressure
- Fossa of Rosenmüller (pharyngeal recess) - posterior to the Eustachian tube opening; common site of nasopharyngeal carcinoma
- Nasopharyngeal tonsil (adenoids) - lymphoid tissue in the roof/posterior wall; largest in childhood, involutes after puberty
- Lined by pseudostratified ciliated (respiratory) epithelium
2. Oropharynx
Boundaries:
- Superior: Junction of hard and soft palate
- Inferior: Valleculae (plane of the hyoid bone)
- Anterior: Communicates with oral cavity through the oropharyngeal isthmus (between the palatoglossal arches)
- Lateral: Faucial pillars (palatoglossal arch anteriorly, palatopharyngeal arch posteriorly)
Key structures:
- Palatine tonsils - sit in the tonsillar fossae between the two faucial pillars (anterior = palatoglossus, posterior = palatopharyngeus); part of Waldeyer's ring
- Base of tongue (posterior 1/3) - slopes down from the sulcus terminalis; contains lingual tonsils (completing Waldeyer's ring)
- Valleculae - shallow depressions between the tongue base and epiglottis, divided by the median glossoepiglottic fold
- Soft palate and uvula - acts as a "flutter valve" to separate nasopharynx from oropharynx during swallowing
- Lined by non-keratinized stratified squamous epithelium
Waldeyer's Ring (Lymphoid Ring of the Pharynx)
A ring of lymphoid tissue forming the first line of immune defense:
| Component | Location |
|---|---|
| Adenoids (nasopharyngeal tonsil) | Roof/posterior nasopharynx |
| Palatine tonsils | Tonsillar fossae, oropharynx |
| Lingual tonsils | Posterior 1/3 of tongue |
| Tubal tonsils (Gerlach's) | Around Eustachian tube opening |
| Lateral pharyngeal bands | Behind posterior pillars |
3. Hypopharynx (Laryngopharynx)
Boundaries:
- Superior: Level of hyoid bone (pharyngoepiglottic folds)
- Inferior: Lower border of cricoid cartilage (continues as esophagus)
- Shaped like a funnel with its anterior segment missing
Key structures:
- Pyriform sinuses (piriform fossae) - paired recesses on either side of the laryngeal inlet; bordered medially by aryepiglottic folds and laterally by thyroid cartilage; common site of food trapping and foreign bodies; also common site of hypopharyngeal carcinoma
- Posterior pharyngeal wall - flat muscular wall behind the larynx
- Postcricoid region - immediately behind the arytenoids/cricoid; connects to the esophagus
- Cricopharyngeus muscle - the sphincter of the pharynx; normally closed, opens only during swallowing; weak point above it (Killian's dehiscence) is where a Zenker's diverticulum can form
Wall of the Pharynx - Layers (Outside to Inside)
| Layer | Description |
|---|---|
| Buccopharyngeal fascia | Thin areolar outer covering; contains the pharyngeal nerve and venous plexus |
| Muscular layer | Three constrictor muscles + three longitudinal muscles (see below) |
| Pharyngobasilar fascia | Fibrous submucosal layer; suspends the pharynx from the skull base; fills the gap above the superior constrictor |
| Mucosa | Lines the lumen; varies by region (respiratory vs squamous epithelium) |
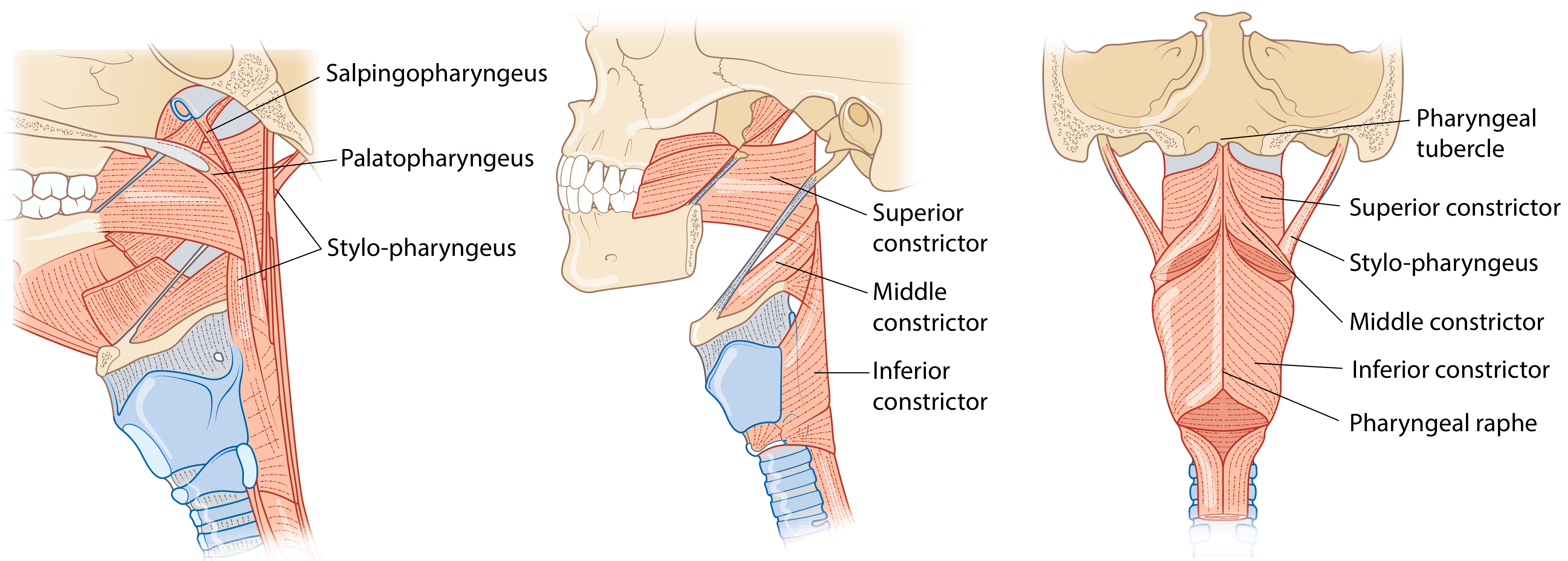
Muscles of the Pharynx
Constrictor Muscles (Circular - compress the lumen for swallowing)
Three muscles interlock like stacked cones, overlapping posteriorly at the pharyngeal raphe:
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Superior constrictor | Pterygoid hamulus, pterygomandibular raphe, mandible, tongue | Pharyngeal raphe | Pharyngeal plexus (CN X + IX) | Constricts nasopharynx/oropharynx |
| Middle constrictor | Greater and lesser horns of hyoid bone, stylohyoid ligament | Pharyngeal raphe | Pharyngeal plexus | Constricts oropharynx |
| Inferior constrictor | Oblique line of thyroid cartilage (thyropharyngeus) + cricoid cartilage (cricopharyngeus) | Pharyngeal raphe | Pharyngeal plexus + recurrent laryngeal nerve | Constricts hypopharynx; cricopharyngeus = upper esophageal sphincter |
Clinical note: The weak area between thyropharyngeus and cricopharyngeus (Killian's dehiscence) is where a Zenker's diverticulum forms as a mucosal herniation.
Longitudinal Muscles (Elevators/Dilators - shorten and widen the pharynx)
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Stylopharyngeus | Medial base of styloid process | Posterior border of thyroid cartilage + lateral glossoepiglottic folds | Glossopharyngeal nerve (CN IX) - only pharyngeal muscle NOT via pharyngeal plexus | Elevates pharynx and larynx; assists peristalsis |
| Palatopharyngeus | Posterior border of hard palate + palatine aponeurosis | Posterior border of thyroid cartilage | Pharyngeal plexus (CN X) | Elevates larynx/pharynx; closes oropharyngeal isthmus during swallowing; forms posterior faucial pillar |
| Salpingopharyngeus | Inferior part of Eustachian tube cartilage | Blends with palatopharyngeus | Pharyngeal plexus (CN X) | Elevates pharynx; opens Eustachian tube |
Nerve Supply
| Structure | Nerve |
|---|---|
| Motor to all pharyngeal muscles (except stylopharyngeus) | Pharyngeal plexus = CN X (vagus) + CN IX (glossopharyngeal) |
| Motor to stylopharyngeus | CN IX (glossopharyngeal) directly |
| Motor to cricopharyngeus | Also recurrent laryngeal nerve (CN X) |
| Sensory - nasopharynx | CN V2 (maxillary branch of trigeminal) |
| Sensory - oropharynx | CN IX (glossopharyngeal) predominantly |
| Sensory - valleculae/base of tongue | Internal laryngeal nerve (branch of CN X) |
| Sensory - palatine tonsils | CN IX + lesser palatine nerve (CN V2) |
Blood Supply
| Region | Artery | Vein |
|---|---|---|
| Nasopharynx | Ascending pharyngeal artery (branch of external carotid) | Pharyngeal venous plexus → internal jugular vein |
| Oropharynx/tonsils | Tonsillar branch of facial artery (main); also lingual, ascending palatine arteries | Paratonsillar vein → external palatine vein → facial vein |
| Hypopharynx | Ascending pharyngeal + inferior thyroid arteries | Pharyngeal plexus |
Clinical note: The internal carotid artery lies only 2.5 cm posterolateral to the palatine tonsils - an important surgical danger zone during tonsillectomy.
Lymphatic Drainage
| Region | Drains to |
|---|---|
| Nasopharynx | Retropharyngeal nodes → upper deep cervical (jugulo-digastric) nodes |
| Oropharynx/tonsils | Jugulodigastric (tonsillar) nodes → deep cervical chain |
| Hypopharynx | Deep cervical nodes (levels II-IV) |
Summary Table
| Feature | Nasopharynx | Oropharynx | Hypopharynx |
|---|---|---|---|
| Extent | Skull base to soft palate | Soft palate to hyoid | Hyoid to cricoid |
| Epithelium | Pseudostratified ciliated | Stratified squamous | Stratified squamous |
| Key structure | Adenoids, Eustachian tube | Palatine tonsils, tongue base | Pyriform sinus, cricopharyngeus |
| Always patent? | Yes (rigid walls) | No (opens/closes) | No (opens/closes) |
| Function | Air passage | Air + food | Food passage only |
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery | K.J. Lee's Essential Otolaryngology | Roberts and Hedges' Clinical Procedures in Emergency Medicine
After pharynx
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Excellent - I now have everything needed for a comprehensive answer on the esophagus.
The Esophagus - Anatomy
Overview
The esophagus is a muscular tube that begins immediately after the pharynx (at the pharyngoesophageal junction / lower border of the cricoid cartilage, C5-C6 level) and ends at the gastroesophageal junction (T10 level). It is the conduit that propels swallowed food into the stomach.
- Length: 18-26 cm (resting); shortens significantly during swallowing
- Diameter: Can distend up to 2 cm anteroposteriorly and 3 cm laterally
- No serosa - unlike the rest of the GI tract, the esophagus has an adventitia (loose connective tissue) instead of serosa. This allows easier spread of esophageal cancers and perforations.
Three Regions
1. Cervical Esophagus (~4-5 cm)
- From the pharyngoesophageal junction (C5-C6) to the suprasternal notch
- Relations:
- Anterior: Trachea
- Posterior: Vertebral column (C5-T1)
- Lateral: Carotid sheaths and thyroid gland
2. Thoracic Esophagus (~16 cm)
- From the suprasternal notch to the diaphragmatic hiatus (T10)
- Runs just posterior to the trachea in the posterior mediastinum
- At T4 (aortic arch level) - deviates right to accommodate the aortic arch
- Posterior to the tracheal bifurcation (carina) and left main bronchus
- At T8 - turns left and crosses anterior to the aorta
- At T10 - passes through the diaphragmatic hiatus
3. Abdominal Esophagus (0.5-2.5 cm)
- From the diaphragmatic hiatus to the cardia of the stomach
- Relations:
- Anterior: Left lobe of liver
- Right: Caudate lobe of liver
- Left: Fundus of stomach
- Posterior: Right crus of diaphragm and aorta
- Compressed by increased intraabdominal pressure (acts as anti-reflux mechanism)
- Enters the stomach at an acute angle - the angle of His - which helps prevent gastric reflux
Narrowings of the Esophagus (4 physiological constrictions)
These are clinically important sites where food, foreign bodies, and strictures tend to get lodged:
| # | Location | Level | Cause |
|---|---|---|---|
| 1 | Pharyngoesophageal junction (Killian's mouth) | C5-C6 | Cricopharyngeus muscle (UES) |
| 2 | Aortic arch impression | T4 | Aorta crosses |
| 3 | Left main bronchus impression | T5 | Bronchus crosses |
| 4 | Diaphragmatic hiatus | T10 | Diaphragm |
Sphincters
Upper Esophageal Sphincter (UES)
- A 2-3 cm zone of elevated resting pressure at the pharyngoesophageal junction
- Primarily formed by cricopharyngeus muscle (C-shaped, attaches to cricoid cartilage at C5-6), plus contributions from the inferior constrictor and thyropharyngeus
- Normally closed - opens during swallowing, belching, and vomiting
- Prevents air entering the esophagus during breathing
Lower Esophageal Sphincter (LES)
- Located at the esophagogastric junction (T10)
- Has two components:
- Intrinsic: Smooth muscle of the LES itself (generates myogenic tone)
- Extrinsic: Crural diaphragm contractions
- Marked externally by the Z-line (squamocolumnar junction) - the abrupt color change from white-tan squamous epithelium to reddish gastric mucosa
- Normally closed - relaxes to allow food into the stomach
- Dysfunction → Gastroesophageal reflux disease (GERD) or achalasia
Wall Layers (Inside → Outside)
| Layer | Details |
|---|---|
| Mucosa | Non-keratinized stratified squamous epithelium + lamina propria + muscularis mucosae |
| Submucosa | Dense connective tissue; contains esophageal glands (mucous secreting); Meissner's plexus |
| Muscularis propria | Inner circular + outer longitudinal layers; upper 1/3 = striated (skeletal) muscle; lower 2/3 = smooth muscle; Auerbach's myenteric plexus between layers |
| Adventitia | Loose connective tissue (NO serosa) |
"The esophagus does not have a serosa but only a loose connective tissue that makes up the adventitia. The absence of a serosal layer allows esophageal perforations and malignancies to disseminate more readily."
- Yamada's Textbook of Gastroenterology, 7th Edition
Muscle Composition by Region
| Region | Muscle Type | Significance |
|---|---|---|
| Upper 1/3 | Striated (skeletal) | Voluntary control of swallowing initiation |
| Middle 1/3 | Mixed striated + smooth | Transition zone |
| Lower 2/3 | Smooth muscle | Involuntary peristalsis |
The striated muscle of the upper esophagus is derived from branchial arches 4, 5, and 6, innervated by corresponding branches of the vagus nerve.
Blood Supply
The arterial supply is segmental with limited overlap (important surgically):
| Segment | Artery |
|---|---|
| Cervical | Branches of inferior thyroid artery (main); also common carotid, subclavian |
| Upper thoracic | Branches of bronchial arteries + vagus nerves |
| Mid-thoracic | Aortic esophageal arteries (direct branches from thoracic aorta) |
| Abdominal | Left gastric artery (branch of celiac axis) + left inferior phrenic artery |
Venous drainage:
- Cervical: → Inferior thyroid vein → brachiocephalic vein → superior vena cava
- Thoracic: → Azygos vein (right), hemiazygos vein (left) → superior vena cava
- Abdominal/lower: → Left gastric vein → portal vein
Clinical note - Esophageal varices: The lower esophagus is a portal-systemic anastomosis site. In portal hypertension (e.g., liver cirrhosis), blood backs up through the left gastric vein into the esophageal veins, dilating them into varices which can rupture and cause life-threatening hemorrhage.
Nerve Supply
Parasympathetic (motor) - via Vagus nerve (CN X):
- Upper esophagus/UES: cell bodies in nucleus ambiguus
- Lower esophagus/LES: from dorsal motor nucleus
- Vagal fibers form the esophageal plexus around the thoracic esophagus
- Below the diaphragm: form anterior vagal trunk (left vagus → anterior gastric + hepatic branches) and posterior vagal trunk (right vagus → posterior gastric + celiac plexus)
- Cervical esophagus: recurrent laryngeal nerves (branches of vagus)
Sympathetic:
- Superior cervical ganglion, sympathetic chain, major splanchnic nerve, celiac ganglion
- Mediates pain (nociception) from the esophagus
Enteric nervous system:
- Auerbach's (myenteric) plexus - coordinates peristalsis of the smooth muscle portion
Lymphatic Drainage
Lymphatic drainage of the esophagus is non-segmental (unlike arterial supply) with extensive interconnections - a key reason why esophageal cancer spreads widely:
| Segment | Drains to |
|---|---|
| Cervical | Cervical lymph nodes |
| Upper thoracic | Paraesophageal, tracheobronchial nodes |
| Mid thoracic | Posterior mediastinal, pericardial nodes |
| Lower thoracic/abdominal | Left gastric and celiac nodes |
"This arrangement accounts for the frequent wide intramural and mediastinal lymphatic spread of esophageal carcinoma."
- Yamada's Textbook of Gastroenterology, 7th Edition
Summary: The Esophagus at a Glance
| Feature | Detail |
|---|---|
| Start | C5-C6 (pharyngoesophageal junction / cricopharyngeus) |
| End | T10 (gastroesophageal junction) |
| Length | 18-26 cm |
| Upper sphincter | Cricopharyngeus (UES) - normally closed |
| Lower sphincter | LES at gastroesophageal junction - prevents reflux |
| Muscle type | Upper 1/3 striated → lower 2/3 smooth |
| Unique feature | No serosa (adventitia only) |
| Key anastomosis | Portal-systemic at lower esophagus (site of varices) |
| Function | Peristalsis propels food bolus to stomach in ~8-10 seconds |
Sources: Yamada's Textbook of Gastroenterology, 7th Edition | K.J. Lee's Essential Otolaryngology | Cummings Otolaryngology Head and Neck Surgery
Whyfood is not going to larynx
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I have everything needed for a thorough, well-illustrated answer.
Why Food Does NOT Enter the Larynx During Swallowing
Food is kept out of the larynx by a series of coordinated protective mechanisms that all fire simultaneously during swallowing - a reflex so precisely timed that the entire pharyngeal phase takes less than 2 seconds.
The 5 Protective Mechanisms - All Happen Simultaneously
1. Soft Palate Rises - Blocks the Nose
- The soft palate is pulled upward to seal off the posterior nares (choanae)
- This prevents food from refluxing into the nasal cavity
- Muscles responsible: levator veli palatini, tensor veli palatini
2. Palatopharyngeal Folds Narrow - Size Filter
- The palatopharyngeal folds on each side are pulled medially, forming a narrow sagittal slit
- This acts as a size filter - only well-chewed food can pass through
- Prevents large, unchewed pieces from proceeding further
3. Larynx Elevates and Moves Forward - Most Important Step
- The larynx is pulled upward and anteriorly by the suprahyoid and thyrohyoid neck muscles
- The hyoid bone is also displaced anteriorly
- This upward movement does two things simultaneously:
- Causes the epiglottis to flip backward (like a trap door) over the laryngeal inlet
- Pulls open the upper esophageal sphincter to receive the food bolus
4. Epiglottis Covers the Laryngeal Opening - Physical Lid
- As the larynx moves up and forward, ligaments prevent the epiglottis from moving upward
- So it is forced to swing backward and downward, covering the laryngeal inlet like a lid
- The epiglottis directs food sideways into the pyriform sinuses (on either side of the larynx) and then into the esophagus
"The backward tilt of the epiglottis covers the opening of the larynx to prevent aspiration."
- Schwartz's Principles of Surgery, 11th Edition
5. Vocal Cords Clamp Shut - The Last Line of Defense
- The vocal cords (true vocal folds) are strongly approximated (adducted) by:
- Adduction of the arytenoid cartilages
- Contraction of the lateral cricoarytenoid muscles
- Contraction of the false vocal folds (ventricular folds) above
- The glottis is completely closed for about 2.3 seconds during swallowing
- This is the most essential mechanism - if the vocal cords fail to close, food can get past the epiglottis and into the airway
"Most essential is the tight approximation of the vocal cords, but the epiglottis helps to prevent food from ever getting as far as the vocal cords. Destruction of the vocal cords or of the muscles that approximate them increases the risk of airway obstruction and choking while swallowing food or drink."
- Guyton and Hall Textbook of Medical Physiology
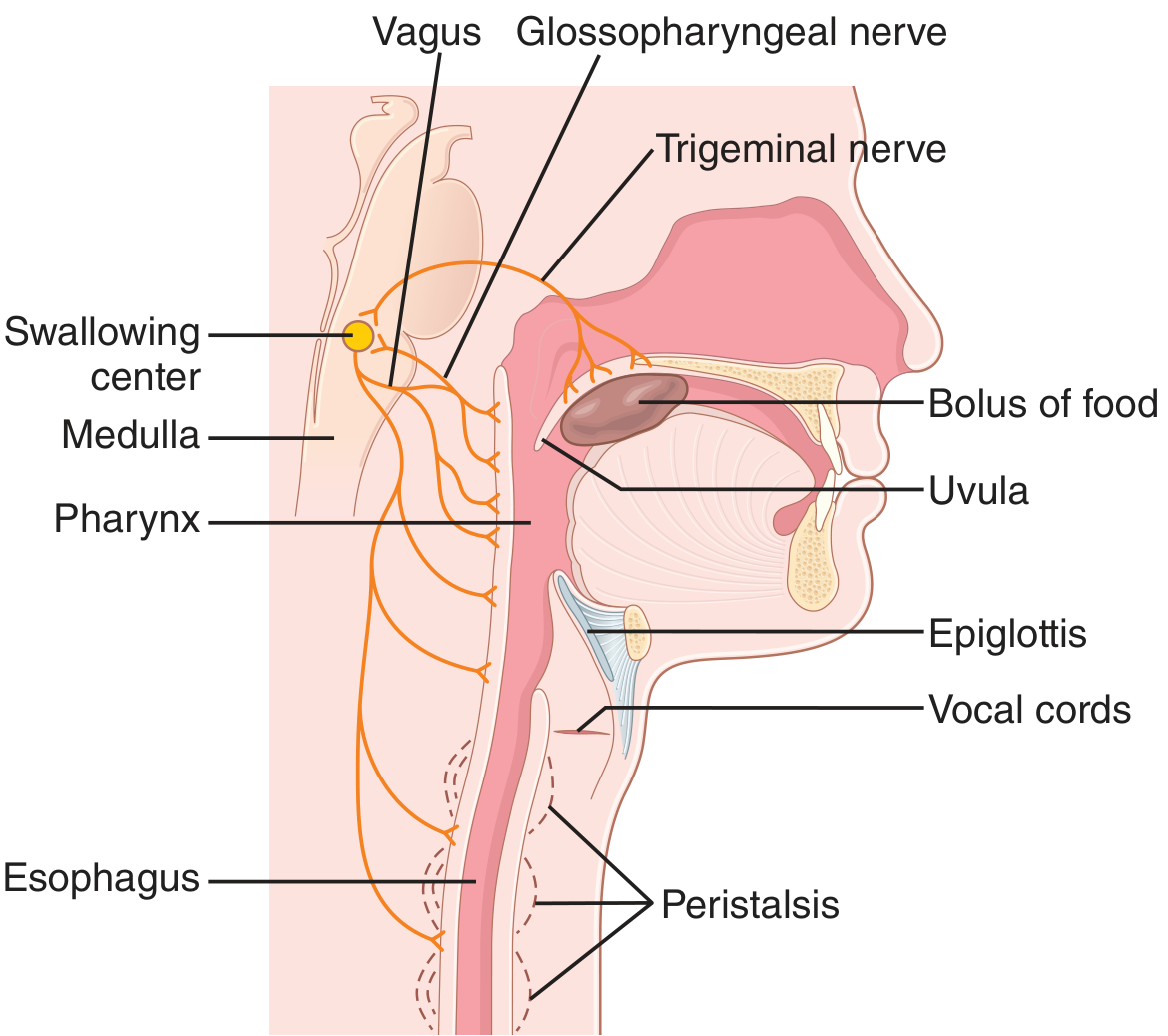
Summary Diagram of Events
Food reaches back of mouth/pharynx
↓
Swallowing receptors (tonsillar pillars, pharyngeal wall) stimulated
↓
Signals sent via CN V (trigeminal) + CN IX (glossopharyngeal) → Medulla
↓
SWALLOWING CENTER (medulla + lower pons) activated
↓ (all 5 events fire simultaneously)
1. Soft palate → UP (blocks nose)
2. Palatopharyngeal folds → IN (size filter)
3. Larynx → UP + FORWARD (opens esophagus, pulls epiglottis down)
4. Epiglottis → BACKWARD (covers larynx opening)
5. Vocal cords → CLOSE (seals the airway completely)
↓
Pharyngeal constrictors contract top to bottom
↓
Food forced into upper esophageal sphincter (which relaxes to receive it)
↓
Peristalsis carries food to stomach in 8-10 seconds
Breathing is Also Paused
The swallowing center in the medulla actively inhibits the respiratory center during swallowing. Breathing is paused for the entire duration of the pharyngeal phase (< 6 seconds). This is why you cannot breathe and swallow at the exact same moment.
"The swallowing center specifically inhibits the respiratory center of the medulla during this time, halting respiration at any point in its cycle to allow swallowing to proceed."
- Guyton and Hall Textbook of Medical Physiology
What Happens If These Mechanisms Fail?
| Mechanism Failed | Result |
|---|---|
| Vocal cords don't close | Food enters the trachea (aspiration) |
| Epiglottis doesn't flip | Food falls toward larynx |
| Larynx doesn't elevate | Upper esophageal sphincter doesn't open properly + aspiration risk increases |
| Swallowing reflex weakened (stroke, elderly) | Aspiration pneumonia - food/liquid enters the lungs |
| Loss of cough reflex | Silent aspiration - food enters lungs without protective cough |
Aspiration pneumonia is a major complication in stroke patients, the elderly, and those with neurological disease, precisely because these protective mechanisms become impaired.
The Nerve Control
Motor signals for the entire coordinated swallowing reflex travel via CN V, IX, X (vagus), XII and upper cervical nerves from the swallowing center in the medulla to the pharyngeal and laryngeal muscles. It is an almost entirely involuntary reflex once food reaches the back of the mouth - you cannot stop it.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
- Guyton and Hall Textbook of Medical Physiology (p. 788-789)
- Schwartz's Principles of Surgery, 11th Edition
This is a shared conversation. Sign in to Orris to start your own chat.