T inversion in lead v1 and v2
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a structured clinical overview of T-wave inversion in leads V1 and V2.
T-Wave Inversion in V1 and V2
Normal vs. Abnormal
T-wave inversion in V1 alone is a normal variant and has no clinical significance. T-wave inversion extending to V2 may still be normal in women, but in adult men it is considered abnormal and warrants clinical correlation.
Causes / Differential Diagnosis
1. Wellens' Syndrome (Critical — Do Not Miss)
A pre-infarction pattern caused by critical proximal LAD stenosis. The T-wave changes appear when the patient is pain-free (post-ischemic reperfusion pattern).
Two patterns:
| Pattern | Morphology | Prevalence |
|---|---|---|
| Type A (Biphasic) | Biphasic T waves in V2–V3 | ~25% |
| Type B (Deep inversion) | Deep symmetric T-wave inversion in V2–V3, often extending to V1 | ~75% |
Diagnostic criteria (Tintinalli's):
- History of episodic chest pain consistent with unstable angina
- During pain, the ECG may be normal
- When pain-free: abnormal T waves most prominent in V2–V3, often in V1 and V3
- Deep symmetric T-wave inversion (~75%) or biphasic T waves (~25%)
- No pathologic Q waves or loss of R waves
These patients are at high risk of massive anterior MI and require urgent coronary angiography.
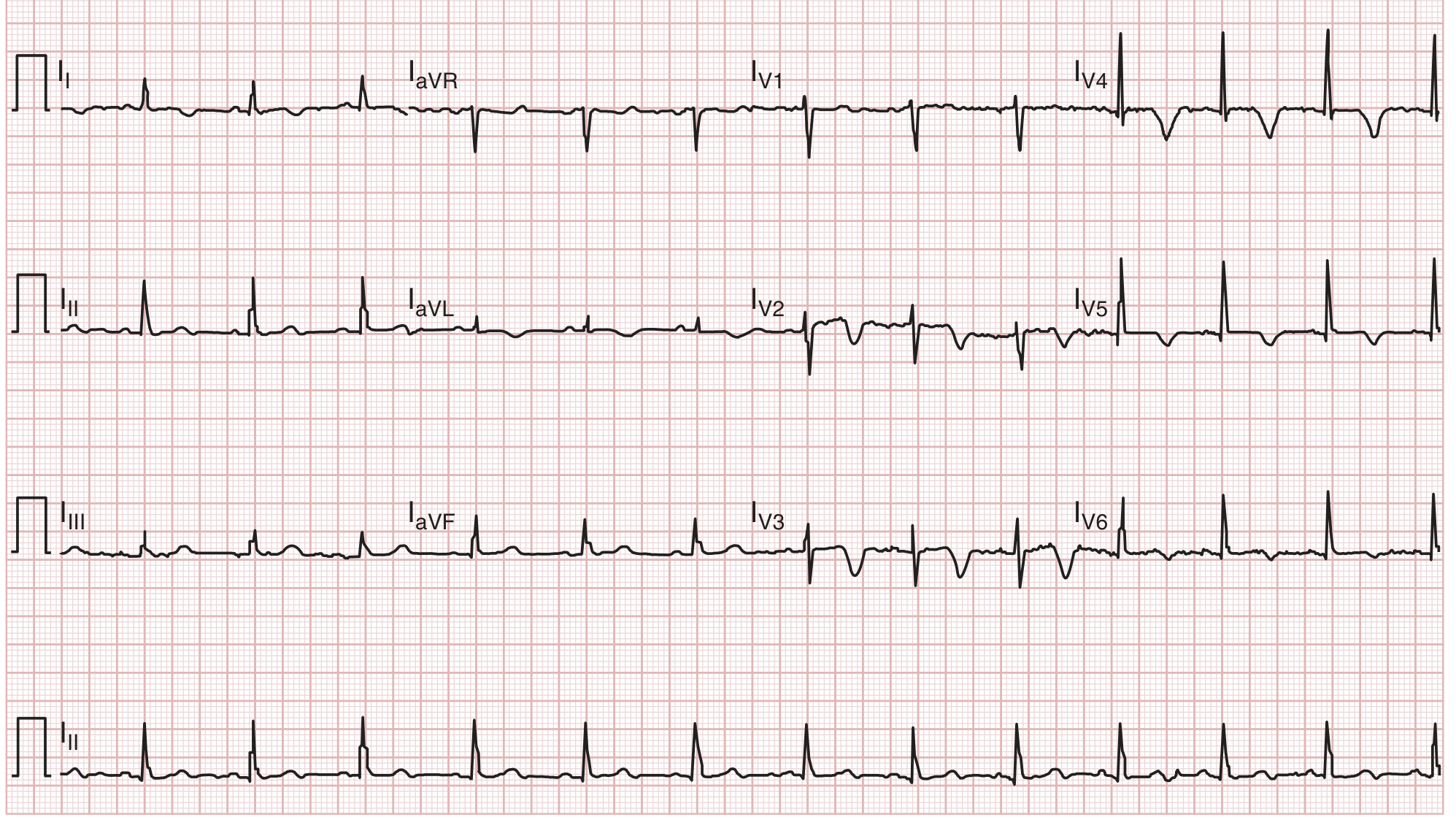
ECG showing Wellens' pattern (deep symmetric T-wave inversion V1–V3):
2. Pulmonary Embolism (PE)
T-wave inversion in V1–V3 (especially V2–V3) is the most frequent ECG sign of high-risk (massive) PE and reflects acute RV strain from right heart dilatation.
- May accompany the S1Q3T3 pattern, right axis deviation, sinus tachycardia, or RBBB
- Both the Qr pattern in V1 and T-wave inversion in V2 are independent predictors of RV dysfunction and adverse outcome
- ~20% of PE patients have no ECG changes; ECG alone cannot rule in or rule out PE
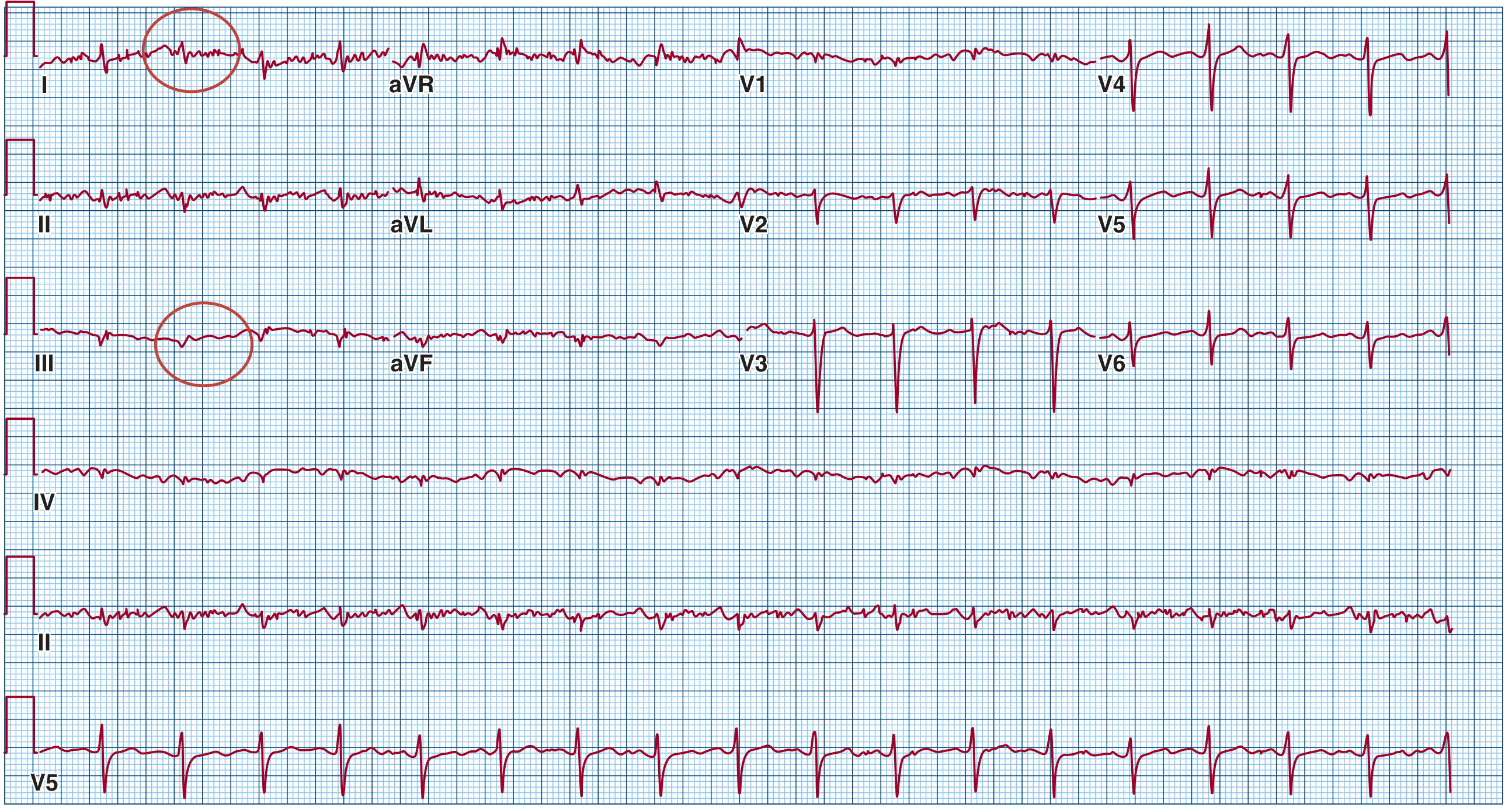
ECG from a 60-year-old with massive PE and cardiogenic shock (note T-wave inversion in right precordial leads + S1Q3T3):
3. ARVC (Arrhythmogenic Right Ventricular Cardiomyopathy)
T-wave inversion in V1–V3 (or more) is a major diagnostic criterion for ARVC, accompanied by:
- Prolonged terminal QRS (>55 ms from S-wave nadir to end of QRS) in V1–V3
- Epsilon waves (small deflections after the QRS in right precordial leads)
- VT with LBBB morphology
4. Brugada Syndrome
Type I Brugada pattern: coved ST elevation (≥2 mm) with T-wave inversion in V1–V2. This is the diagnostic pattern; it may be present spontaneously or only after sodium channel blocker challenge (e.g., procainamide, flecainide, ajmaline).
5. Right Bundle Branch Block (RBBB)
Secondary T-wave inversions in V1–V2 are an expected finding in RBBB and are not independently pathological — they follow the direction opposite to the dominant terminal R' wave (discordant repolarization).
6. Right Ventricular Hypertrophy / Cor Pulmonale
Chronic RV pressure overload (e.g., from pulmonary hypertension) can produce T-wave inversions in V1–V3 as a "strain" pattern.
7. Posterior MI (Isolated)
T-wave inversion in V1–V2 may represent a reciprocal change of posterior STEMI. Applying posterior leads (V7–V9) to confirm ST elevation over the left posterior chest helps confirm this diagnosis.
8. Normal Variant / Juvenile T-wave Pattern
Isolated inversion in V1–V2 (sometimes V3) can persist as a normal variant, especially in young women, and is termed the juvenile T-wave pattern when there are no other findings.
Quick Summary Table
| Cause | Key Features |
|---|---|
| Wellens' syndrome | Pain-free, deep symmetric or biphasic T-wave inversions V2–V3; critical LAD stenosis |
| Pulmonary embolism | RV strain, S1Q3T3, tachycardia; most frequent ECG sign of high-risk PE |
| ARVC | Epsilon waves, prolonged terminal QRS V1–V3, T-wave inversion V1–V5 |
| Brugada syndrome | Coved ST elevation + T-wave inversion V1–V2 |
| RBBB | Secondary discordant T-wave inversion; expected finding |
| RV hypertrophy | Chronic RV strain; tall R in V1 |
| Posterior MI | Reciprocal change; tall R/T in V1–V2; confirm with V7–V9 |
| Normal variant | Isolated V1–V2; young women; no other findings |
Clinical bottom line: T-wave inversion confined to V1 is usually benign. Extension to V2 in an adult male — especially in the context of chest pain — demands urgent evaluation for Wellens' syndrome, ACS, or PE, as these carry high short-term mortality risk.
Sources: Tintinalli's Emergency Medicine, Fuster & Hurst's The Heart 15th Ed., Braunwald's Heart Disease
Female pt
Checking Date & Time
Good clarification. In a female patient, T-wave inversion in V1 and V2 shifts the differential in important ways:
T-Wave Inversion V1–V2 in a Female Patient
Key Difference from Males
T-wave inversion in V1 and V2 is more often a normal variant in women — particularly premenopausal women, where it can extend to V3 and still be considered physiological (persistent juvenile T-wave pattern). This is the most important gender-specific caveat.
However, "normal variant" is a diagnosis of exclusion — all pathological causes must still be considered based on clinical context.
Revised Differential Priority in Females
✅ Normal / Benign (Higher probability in females)
| Finding | Notes |
|---|---|
| Juvenile T-wave pattern | T-wave inversion in V1–V3 is common in young/premenopausal women; a normal variant |
| Athlete's heart | T-wave inversion in V1–V2 in female athletes is classified as a normal training adaptation and does not warrant further investigation (Fuster & Hurst, 15th Ed.) |
Per international athlete ECG criteria, T-wave inversion ≥1 mm in depth in two or more contiguous leads excluding aVR, III, and V1 is abnormal. Because V1 is excluded from this criterion, isolated inversion in V1–V2 in a female athlete requires specific clinical judgment.
⚠️ Still Must Exclude (Pathological — same as males)
| Cause | Distinguishing Features |
|---|---|
| Wellens' syndrome | History of chest pain; pain-free ECG with deep symmetric or biphasic T waves V2–V3; critical LAD stenosis — equally dangerous in women |
| Pulmonary embolism | Dyspnea, hypoxia, tachycardia; particularly relevant in women on OCPs or postpartum |
| ARVC | Less common in women; epsilon waves, terminal QRS prolongation V1–V3 |
| Brugada syndrome | Coved ST elevation V1–V2; less penetrant in women but still occurs — female sex is associated with fewer spontaneous events |
| RBBB | Discordant secondary T-wave changes; benign if isolated |
| RV hypertrophy / pulmonary HTN | Women are disproportionately affected by pulmonary arterial hypertension — screen if dyspnea present |
| Posterior MI | Reciprocal changes; less likely to present classically in women |
Pulmonary Hypertension — Female-Specific Consideration
Pulmonary arterial hypertension (PAH) has a female:male ratio of ~3:1. T-wave inversion in the right precordial leads from chronic RV pressure overload should prompt echocardiography if any exertional dyspnea is present in a female patient.
Practical Approach in a Female Patient
T inversion V1–V2 in a female
│
├─ Asymptomatic + young/premenopausal + no other ECG changes?
│ → Likely normal variant / juvenile pattern — reassure
│
├─ History of chest pain (even if pain-free now)?
│ → Rule out Wellens' syndrome — urgent troponin + cardiology referral
│
├─ Dyspnea, hypoxia, tachycardia?
│ → Rule out PE (especially if on OCP/pregnant/postpartum)
│ → Rule out pulmonary hypertension (echo)
│
├─ Palpitations, syncope, family history of SCD?
│ → Consider ARVC, Brugada, channelopathy — refer to electrophysiology
│
└─ Coved ST elevation in V1–V2?
→ Brugada pattern — refer regardless of symptoms
Bottom line: In a female patient, isolated V1–V2 T-wave inversion is more likely to be a normal variant than in a male, but Wellens' syndrome, PE, and pulmonary hypertension remain clinically significant causes that must be excluded based on symptoms, age, and risk factors.
This is a shared conversation. Sign in to Orris to start your own chat.