Alveolar arterial gradient Full details for md exams 15marks
Reading File
search_medical_text
alveolar arterial gradient A-a gradient calculation formula physiology
search_medical_text
A-a gradient clinical significance causes hypoxemia interpretation
search_medical_image
alveolar arterial gradient oxygen diagram ventilation perfusion
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive, exam-ready answer on the Alveolar-Arterial (A-a) Gradient — structured for a 15-mark MD exam response.
Alveolar-Arterial (A-a) Oxygen Gradient
Definition
The alveolar-arterial (A-a) gradient (also written PA-aO₂ or A-aDO₂) is the difference between the partial pressure of oxygen in the alveoli (PAO₂) and in the systemic arterial blood (PaO₂). It is a fundamental index of pulmonary gas exchange efficiency.
A-a gradient = PAO₂ − PaO₂
Physiological Basis
In a perfect lung, alveolar and arterial oxygen tensions would be equal. In reality, a small gradient always exists due to three physiological causes:
| Cause | Contribution |
|---|---|
| Anatomical (true) shunts | Thebesian veins, bronchial circulation (~2%) |
| Physiological V/Q mismatch | Regional variation in ventilation-perfusion ratios |
| Diffusion limitation | Minimal at rest; relevant during exercise or disease |
The Alveolar Gas Equation
To calculate the A-a gradient, you must first calculate PAO₂ using the alveolar gas equation:
$$\boxed{PAO_2 = (F_iO_2 \times [P_{bar} - P_{H_2O}]) - \frac{PaCO_2}{RQ}}$$
Where:
- FiO₂ = Fraction of inspired oxygen (0.21 on room air)
- P_bar = Barometric pressure (760 mmHg at sea level)
- P_H₂O = Water vapor pressure at 37°C = 47 mmHg
- PaCO₂ = Arterial CO₂ tension (from ABG)
- RQ = Respiratory Quotient = 0.8 (standard assumption)
Simplified formula on room air at sea level:
$$PAO_2 = 150 - \frac{PaCO_2}{0.8}$$
Derivation: FiO₂ × (760 − 47) = 0.21 × 713 ≈ 150 mmHg
Then:
$$\text{A-a gradient} = PAO_2 - PaO_2$$
Example Calculation:
- PaCO₂ = 40 mmHg, PaO₂ = 90 mmHg (from ABG)
- PAO₂ = 150 − (40/0.8) = 150 − 50 = 100 mmHg
- A-a gradient = 100 − 90 = 10 mmHg ✓ (Normal)
Normal Values
| Parameter | Value |
|---|---|
| Normal A-a gradient (young adult) | 5–15 mmHg |
| Age-adjusted normal | (Age/4) + 4 mmHg |
| Upper limit of normal | < 25–30 mmHg |
| On 100% O₂ (FiO₂ = 1.0) | < 100 mmHg |
Age correction is critical: A gradient of 25 mmHg is normal in a 70-year-old but abnormal in a 20-year-old.
Harrison's Principles of Internal Medicine (21st Ed., p. 7863) notes that the alveolar gas equation underscores the interplay of FiO₂, barometric pressure, water vapor pressure, and alveolar ventilation in determining PaO₂.
Pathophysiology: Mechanisms of an Elevated A-a Gradient
An elevated A-a gradient = intrinsic lung/vascular problem. The four mechanisms:
1. V/Q Mismatch (most common cause)
- Some alveoli are ventilated but poorly perfused (high V/Q → dead space)
- Some alveoli are perfused but poorly ventilated (low V/Q → shunt-like effect)
- Corrects with supplemental O₂
- Examples: COPD, pulmonary embolism, asthma, pneumonia
2. Right-to-Left Shunt
- Deoxygenated blood bypasses ventilated alveoli entirely
- Does NOT correct with 100% O₂ (hallmark feature)
- Examples: ASD, VSD with Eisenmenger, intrapulmonary AVM, consolidation, ARDS
3. Diffusion Impairment
- O₂ cannot equilibrate across thickened alveolar-capillary membrane
- Worsens with exercise; corrects partially with O₂
- Examples: Interstitial lung disease, pulmonary fibrosis
4. Low Mixed Venous PO₂ (exacerbates above)
- Severe anemia, low cardiac output — exaggerates V/Q mismatch effect
- Not a primary cause of elevated A-a gradient independently
Clinical Interpretation
A-a Gradient as a Diagnostic Tool in Hypoxemia
The A-a gradient is the single most important tool to categorize hypoxemia:
| A-a Gradient | Mechanism | Diagnosis |
|---|---|---|
| Normal (< 15 mmHg) | Hypoventilation only | CNS depression (opioids, sedatives), neuromuscular disease, obesity hypoventilation |
| Elevated (> 15–20 mmHg) | Intrinsic lung pathology | V/Q mismatch, shunt, diffusion impairment |
Severity Classification (Prevention & Treatment of Opportunistic Infections, HIV Guidelines, p. 542):
| Severity | A-a Gradient |
|---|---|
| Mild hypoxemia | PaO₂ ≥ 70 mmHg or A-a gradient < 35 mmHg |
| Moderate hypoxemia | A-a gradient ≥ 35 to < 45 mmHg |
| Severe hypoxemia | A-a gradient ≥ 45 mmHg |
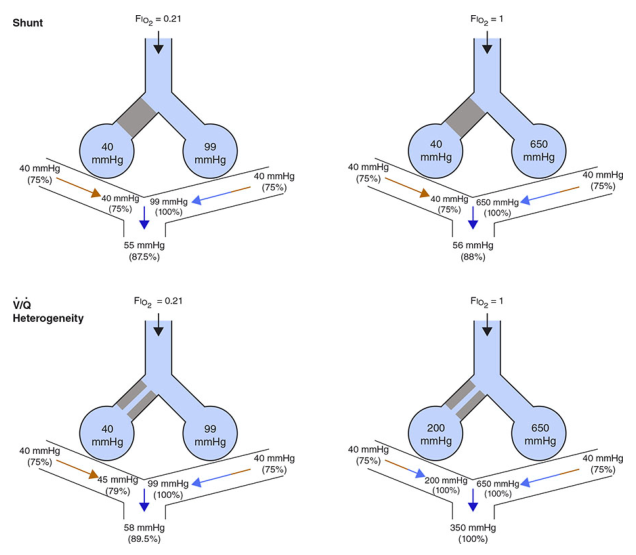
The 100% O₂ Test (Shunt Fraction Estimation)
Administering 100% FiO₂ allows differentiation:
| Response to 100% O₂ | Interpretation |
|---|---|
| PaO₂ rises to > 500 mmHg | V/Q mismatch (not true shunt) |
| PaO₂ fails to rise significantly | True anatomical/intracardiac shunt |
Shunt equation (Qs/Qt):
$$\frac{Q_s}{Q_t} = \frac{C_cO_2 - C_aO_2}{C_cO_2 - C_{\bar v}O_2}$$
Normal shunt fraction: < 5%
V/Q Mismatch vs Shunt — Key Differences
| Feature | V/Q Mismatch | Right-to-Left Shunt |
|---|---|---|
| A-a gradient | Elevated | Elevated |
| Response to 100% O₂ | Corrects | Does NOT correct |
| Example | PE, COPD | ASD, ARDS, lobar collapse |
| Dead space involvement | Yes | No |
Causes of Elevated A-a Gradient — Clinical Summary
Pulmonary Causes (V/Q mismatch):
- Pulmonary embolism (classic — elevated A-a gradient with normal/low PaCO₂)
- COPD/emphysema
- Asthma (acute)
- Pneumonia, atelectasis
- Pulmonary edema (cardiogenic/non-cardiogenic)
- ARDS
- Interstitial lung disease / pulmonary fibrosis
Shunt Causes:
- Intracardiac: ASD, VSD, PDA (with right-to-left shunting)
- Intrapulmonary: Hepatopulmonary syndrome, AVM
- Pulmonary consolidation / collapse (no ventilation, perfusion preserved)
Normal A-a Gradient with Hypoxemia:
- Hypoventilation syndromes — opioid/sedative overdose, CNS lesions, myasthenia gravis, GBS, hypothyroidism
- High altitude (low FiO₂ → low PAO₂, but gas exchange intact)
A-a Gradient in Pulmonary Embolism
PE classically presents with:
- Hypoxemia + hypocapnia (tachypnea-induced)
- Elevated A-a gradient — due to dead space creation (unperfused but ventilated alveoli)
- The A-a gradient is elevated in >80–90% of PE cases
- However, a normal A-a gradient does NOT exclude PE
Factors Affecting A-a Gradient
| Factor | Effect on A-a gradient |
|---|---|
| Increasing age | Increases (normal aging) |
| Increasing FiO₂ | Increases slightly (even in normals) |
| Exercise | Increases in diffusion impairment |
| High altitude | Increases |
| Body position (supine) | Increases slightly |
A-a Gradient vs PaO₂/FiO₂ Ratio
| Index | Formula | Normal | Use |
|---|---|---|---|
| A-a gradient | PAO₂ − PaO₂ | < 15 mmHg | Localizes hypoxemia mechanism |
| P/F ratio | PaO₂ / FiO₂ | > 400 mmHg | Severity of ARDS (Berlin criteria) |
| a/A ratio | PaO₂ / PAO₂ | > 0.75 | Less FiO₂-dependent than A-a gradient |
ARDS Classification by P/F ratio (Berlin Definition):
- Mild: 200–300 mmHg
- Moderate: 100–200 mmHg
- Severe: < 100 mmHg
Summary for Exam — Quick Points
- Definition: Difference between alveolar O₂ (PAO₂) and arterial O₂ (PaO₂)
- Formula: PAO₂ = FiO₂ × (P_bar − 47) − PaCO₂/0.8; A-a = PAO₂ − PaO₂
- Normal: 5–15 mmHg; age-adjusted = age/4 + 4
- Normal gradient + hypoxemia → Hypoventilation (no lung pathology)
- Elevated gradient → Intrinsic lung disease (V/Q mismatch, shunt, diffusion defect)
- O₂ corrects V/Q mismatch; does NOT correct true shunt
- Elevated in PE — due to dead space effect
- Severity: < 35 mild, 35–45 moderate, > 45 severe
- P/F ratio is the clinical counterpart used in ICU/ARDS
- Age matters — always apply age correction before labeling gradient as abnormal
Sources: Harrison's Principles of Internal Medicine, 21st Edition (pp. 7863, 7865); Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV (p. 542)
This is a shared conversation. Sign in to Orris to start your own chat.