Tb lymphadentis full details for md exams 15marks
Reading File
search_medical_text
tuberculosis lymphadenitis pathology etiology classification cervical scrofula
search_medical_text
TB lymphadenitis clinical features diagnosis investigations FNAC histopathology treatment
search_medical_image
tuberculosis lymphadenitis histopathology FNAC cervical lymph node
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive, exam-ready answer on Tuberculous Lymphadenitis structured for a 15-mark MD question.
TUBERCULOUS LYMPHADENITIS (TB Lymphadenitis / Scrofula)
1. DEFINITION
Tuberculous lymphadenitis is the most common form of extrapulmonary tuberculosis, characterized by granulomatous infection of lymph nodes caused primarily by Mycobacterium tuberculosis (rarely M. bovis or non-tuberculous mycobacteria). Cervical involvement is called scrofula (Latin: scrofa = brood sow).
2. EPIDEMIOLOGY
| Parameter | Details |
|---|---|
| Incidence | 35% of all extrapulmonary TB worldwide; >40% in the USA |
| Most common site | Cervical & supraclavicular nodes |
| High-risk groups | Children, HIV-infected individuals, non-Caucasian women, immunocompromised |
| Causative organism | M. tuberculosis (predominantly); M. bovis (historical) |
(Harrison's Principles of Internal Medicine, 21st Ed., p. 5132)
3. ETIOLOGY & PATHOGENESIS
Route of infection:
- Primary focus → haematogenous or lymphatic spread from a pulmonary or abdominal TB focus
- Direct extension from a contiguous primary focus (e.g., tonsil → cervical nodes)
- Reactivation of dormant bacilli seeded during primary infection
Pathogenesis sequence:
- Mycobacteria arrive via lymphatics → phagocytosed by macrophages → T-cell mediated delayed hypersensitivity → epithelioid granuloma formation → central caseous necrosis → liquefaction → collar-stud abscess → sinus tract formation (if untreated)
4. STAGES (Pathological / Surgical Staging)
| Stage | Pathology | Clinical Finding |
|---|---|---|
| I | Reactive hyperplasia | Firm, discrete, rubbery node |
| II | Granuloma without necrosis | Discrete, slightly tender node |
| III | Granuloma with caseation | Matted, non-tender nodes |
| IV | Abscess formation (liquefaction) | Fluctuant swelling with erythema |
| V | Collar-stud abscess | Bilobed abscess through deep fascia |
| VI | Sinus tract formation | Discharging sinus on skin |
5. SITES OF INVOLVEMENT
- Cervical (most common) — posterior triangle, anterior triangle
- Supraclavicular
- Axillary
- Mediastinal (paratracheal, hilar)
- Mesenteric — "tabes mesenterica" in children
- Inguinal
- Para-aortic
6. CLINICAL FEATURES
Symptoms
- Painless swelling of lymph nodes (hallmark)
- Constitutional features: low-grade fever, night sweats, weight loss, fatigue (present in ~40%)
- Rarely painful (unless secondary infection)
Signs
- Early: Discrete, firm, rubbery, non-tender nodes
- Late: Matted, fixed, fluctuant mass; collar-stud abscess; discharging sinus
- Overlying skin: erythematous, thinned, or with scar (in sinus stage)
- May have features of primary pulmonary TB
Collar-Stud Abscess (Clinically important!)
- Cold abscess perforates the deep cervical fascia
- Bilobar abscess — upper (deep) and lower (superficial) compartments communicating through a narrow neck
- No signs of acute inflammation → hence "cold" abscess
7. INVESTIGATIONS
A. Laboratory Tests
| Investigation | Finding |
|---|---|
| ESR | Elevated (non-specific) |
| CBC | Lymphocytosis, normocytic anaemia |
| Mantoux/TST | Positive (>10 mm in immunocompetent; >5 mm in HIV) |
| IGRA (Interferon-Gamma Release Assay) | High sensitivity & specificity; useful in BCG-vaccinated individuals |
| Serum ADA | Elevated (>40 U/L) — supportive |
B. Imaging
| Modality | Findings |
|---|---|
| Chest X-ray | Pulmonary TB focus, mediastinal adenopathy, Ghon complex |
| USG Neck | Hypoechoic nodes, matting, central necrosis, calcification |
| CT with contrast | Peripheral ring enhancement + central hypodense necrosis — pathognomonic pattern |
| PET-CT | Useful for systemic disease mapping |
C. Microbiological & Pathological (KEY for diagnosis)
1. FNAC (Fine Needle Aspiration Cytology) — First-line, rapid, minimally invasive
- Smear shows: epithelioid cell granulomas + Langhans' giant cells + caseation necrosis + lymphocytes
- Send material for: AFB smear, culture, TB-PCR
2. Ziehl-Neelsen (ZN) Stain — Detects acid-fast bacilli (AFB)
- Red bacilli on blue background
- Sensitivity ~30–40% (low)
3. FNAC / Biopsy Histopathology Findings:
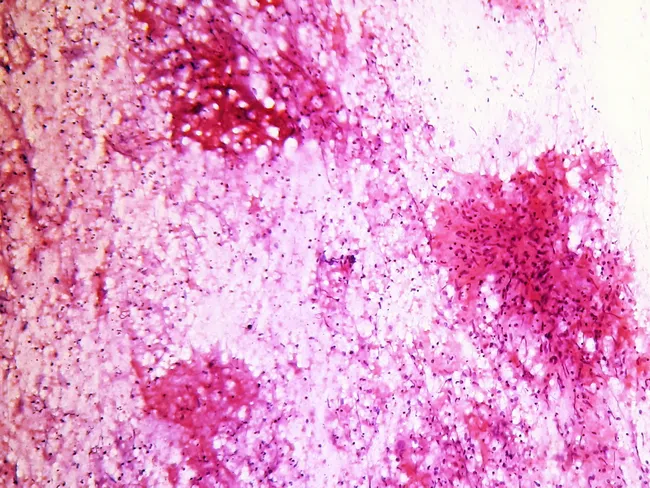
- Epithelioid histiocytes forming cohesive granulomas
- Langhans' giant cells (nuclei arranged in horseshoe/peripheral pattern)
- Caseous necrosis (central, cheese-like)
- Background lymphocytes and plasma cells
4. Culture (Gold Standard)
- Lowenstein-Jensen (LJ) medium — grows in 6–8 weeks (slow)
- MGIT (Mycobacteria Growth Indicator Tube) — automated, faster (1–2 weeks)
5. Molecular Tests
- GeneXpert MTB/RIF (CBNAAT): Rapid (2 hours), detects MTB + rifampicin resistance (RIF)
- Line Probe Assay (LPA): Detects INH & RIF resistance
- TB-PCR: High sensitivity in paucibacillary cases
- Whole Genome Sequencing (WGS): Drug resistance profiling
8. HISTOPATHOLOGICAL TYPES OF GRANULOMA
| Type | Description |
|---|---|
| Epithelioid granuloma without necrosis | Early stage; DDx sarcoidosis |
| Epithelioid granuloma with caseation | Classic TB — highly specific |
| Suppurative granuloma | Neutrophilic; DDx atypical mycobacteria, cat-scratch disease |
| Non-necrotizing granuloma | DDx fungal, sarcoid, foreign body |
9. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Features |
|---|---|
| Non-Hodgkin's/Hodgkin's Lymphoma | Reed-Sternberg cells, B symptoms, no AFB |
| Reactive lymphadenitis | Acute, tender, resolves with antibiotics |
| Non-tuberculous mycobacteria (NTM) | Immunocompromised, culture differentiates |
| Sarcoidosis | Non-caseating granulomas, bilateral hilar nodes, ACE elevated |
| Cat-scratch disease | Bartonella henselae, stellate granuloma, cat exposure |
| Fungal (Histoplasma/Cryptococcus) | Specific culture/serology, immunocompromised |
| Metastatic carcinoma | Atypical cells, no granuloma, primary tumor evident |
10. TREATMENT
Anti-Tubercular Therapy (ATT) — WHO / RNTCP Guidelines
Standard regimen: 2HRZE / 4HR
| Phase | Duration | Drugs |
|---|---|---|
| Intensive Phase | 2 months | Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) |
| Continuation Phase | 4 months | Isoniazid (H) + Rifampicin (R) |
| Total duration | 6 months | (Some guidelines extend to 9 months for extensive disease) |
Drug doses (standard):
| Drug | Dose |
|---|---|
| Isoniazid (H) | 5 mg/kg/day (max 300 mg) |
| Rifampicin (R) | 10 mg/kg/day (max 600 mg) |
| Pyrazinamide (Z) | 25 mg/kg/day |
| Ethambutol (E) | 15 mg/kg/day |
- Add Pyridoxine (Vit B6) with INH to prevent peripheral neuropathy
- Response monitored clinically (node regression); lymph nodes may paradoxically enlarge at 2–3 months (immune reconstitution) — do NOT stop ATT
Surgical Management (indications):
- Diagnostic excision biopsy — when FNAC inconclusive
- Drainage of collar-stud abscess (under ATT cover)
- Excision of persistent or matted nodes not responding to ATT
- Sinus tract debridement and excision
Never incise a cold abscess without ATT cover — risk of sinus formation
11. COMPLICATIONS
- Collar-stud abscess → sinus tract formation
- Sinus formation with chronic discharging wound
- Scarring and cosmetic deformity
- Spread → mediastinal, pericardial, meningeal TB
- Secondary bacterial infection of sinuses
- Paradoxical reaction (nodes enlarge during treatment — especially in HIV patients on ART)
12. PROGNOSIS
- Excellent with complete 6-month ATT — >95% cure rate
- Paradoxical enlargement is self-limiting; short course corticosteroids (Prednisolone 1–2 mg/kg) may be used
- Recurrence suggests drug resistance → send for GeneXpert/culture/DST
13. SPECIAL SITUATIONS
| Situation | Management |
|---|---|
| HIV co-infection | Start ATT first; delay ART by 2–8 weeks; beware paradoxical IRIS |
| MDR-TB | Extended regimen (18–24 months) with fluoroquinolones + injectables |
| Pregnancy | Avoid Streptomycin (ototoxic to fetus); 2HRZ/7HR is safe |
| Children | Same regimen; Ethambutol used cautiously (visual monitoring) |
QUICK RECALL SUMMARY (Exam Mnemonics)
- SCROFULA = Cervical TB lymphadenitis (historic name)
- COLLAR-STUD abscess = pathognomonic surgical sign of TB lymphadenitis
- LANGHANS giant cell = nuclei at periphery (horseshoe arrangement)
- 2HRZE / 4HR = standard ATT regimen
- GeneXpert = fastest diagnostic test (detects MTB + RIF resistance in 2 hours)
- Paradoxical reaction = nodes enlarge during ATT — do not stop treatment
Sources: Harrison's Principles of Internal Medicine, 21st Ed. (p. 5132) | Webpathology (Cytopathology Image) | WHO/RNTCP TB Treatment Guidelines | Bailey & Love's Short Practice of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.