Colles fracture in short everything for viva
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Here is a complete viva-ready summary of Colles fracture, sourced from Rosen's Emergency Medicine, Tintinalli's, Pye's Surgical Handicraft, Pfenninger & Fowler, and Campbell's Operative Orthopaedics.
Colles Fracture - Complete Viva Notes
Definition
A transverse fracture of the distal radial metaphysis, within 2.5 cm of the articular surface, with:
- Dorsal displacement and angulation of the distal fragment
- Radial deviation / displacement
- Proximal impaction (radial shortening)
"The most common wrist fracture." - Pfenninger & Fowler's
Eponym & History
Named after Abraham Colles (1814) who described it before X-rays existed - purely a clinical description.
Mechanism
Fall on an outstretched hand (FOOSH) - the wrist is in extension/dorsiflexion at impact. Compression forces on the dorsal cortex produce dorsal comminution.
Epidemiology / Who Gets It?
- Most common in post-menopausal women (osteoporosis - considered a pathological fracture in osteoporotic bone)
- Bimodal: elderly women (low-energy falls) and young adults (high-energy trauma)
Classic Deformity: "Dinner Fork" / "Silver Fork"
The wrist profile from the lateral side resembles a dinner fork:
- Dorsal prominence of distal fragment
- Volar concavity proximally
- Associated prominent lower end of ulna (radial deviation)
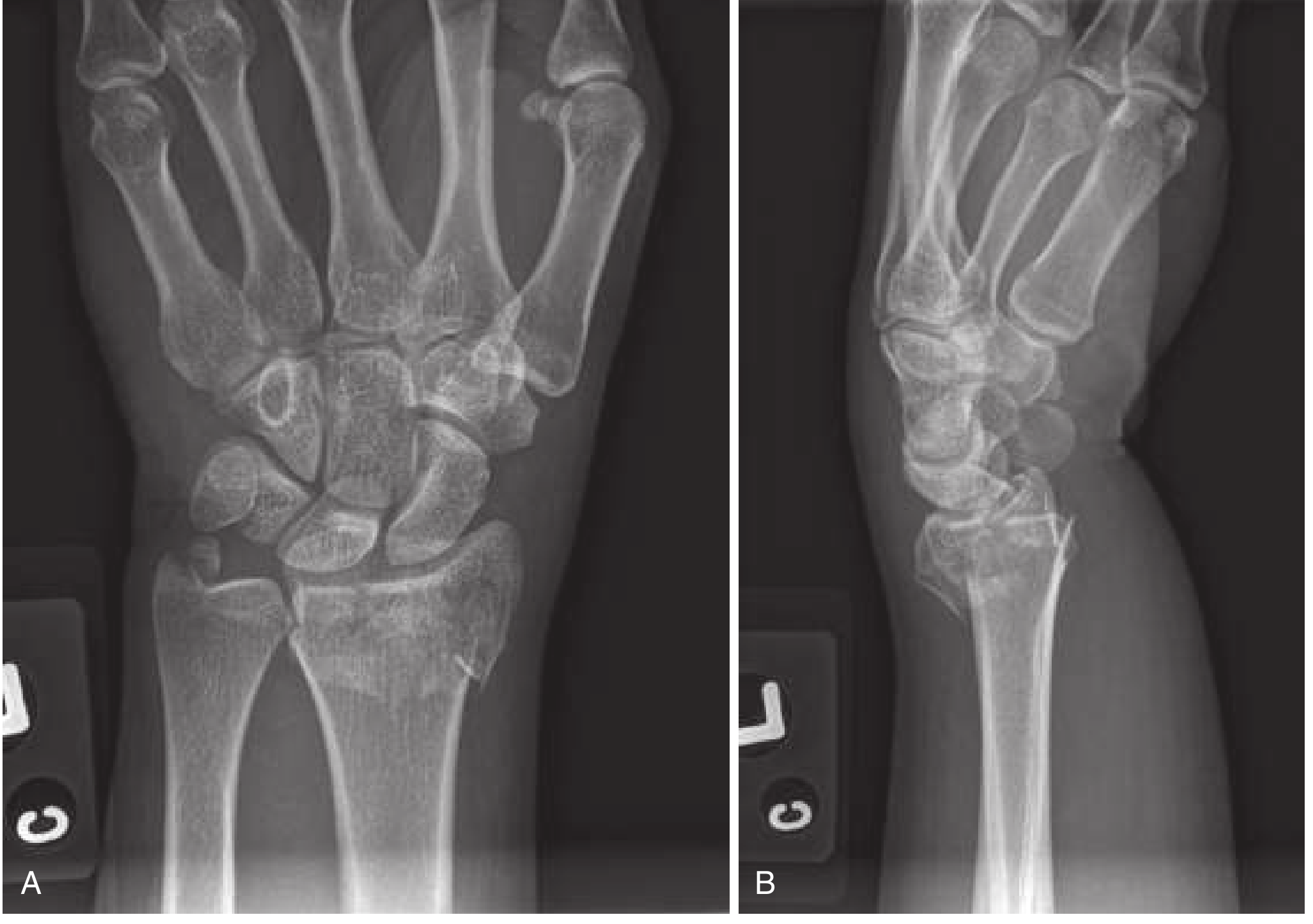
X-ray Findings
PA (AP) view:
- Distal radial metaphyseal fracture with shortening
- Radial deviation of carpus
- Loss of radial inclination (normal ~22-23°)
- Fracture of ulnar styloid (present in ~60% of cases) - indicates disruption of the triangular fibrocartilage complex (TFCC)
- Possible intraarticular extension into radiocarpal or radioulnar joint
Lateral view:
- Dorsal angulation of distal radial articular surface (normally has 11-12° volar tilt - this is lost or reversed)
- Best view to assess degree of displacement
Associated Injuries
- Ulnar styloid fracture (60%) - from TFCC avulsion
- Median nerve injury (most common nerve, ~17%) - from contusion, traction, or swelling
- TFCC injury - source of long-term morbidity
- Scaphoid fracture (occasionally)
- Radioulnar joint disruption
Radiological Parameters - Memorize These
| Parameter | Normal | Acceptable post-reduction |
|---|---|---|
| Volar tilt (lateral) | +11 to +12° | 0° (neutral) minimum |
| Radial inclination (AP) | 22-23° | > 15° |
| Radial length | Radius longer than ulna | ≤ 5 mm shortening |
| Intraarticular step-off | 0 mm | < 2 mm |
Gartland & Werley Classification (1951) - For Viva
| Group | Type |
|---|---|
| Group 1 | Simple Colles fracture |
| Group 2 | Comminuted Colles, undisplaced intraarticular fragment |
| Group 3 | Comminuted Colles, displaced intraarticular fragment |
(From Campbell's Operative Orthopaedics 15th Ed)
Indicators of Instability (require surgical consideration)
- Dorsal angulation ≥ 20 degrees
- Radial shortening > 5 mm (≥1 cm)
- Intraarticular involvement
- Marked comminution
- Age > 60 with osteoporosis
- Dominant hand in high-demand patient
Management
Undisplaced / Stable fractures
- Double sugar-tong splint for 3-5 days → short-arm cast for 4-6 weeks
- Follow-up X-rays at 1, 2, and 6 weeks
Displaced fractures - Closed Reduction
Anesthesia options:
- Hematoma block - 22G needle inserted dorsally into fracture site, aspirate hematoma, inject 5-10 mL of 1-2% lidocaine. Easiest and effective.
- Bier block (IV regional anesthesia)
- Regional nerve blocks (median, radial, ulnar, brachial plexus)
- Procedural sedation (GA for complex/uncooperative)
Reduction technique:
- Apply traction (finger traps or manual) to disimpact the fragment
- Push distal fragment distally, volarly (anteriorly), and ulnarly
- Apply traction via thumb in line with forearm for ulnar deviation
- Minimal palmar flexion - extreme flexion is unnecessary and harmful (damages median nerve)
- Mold into dorsal plaster slab
Goal: Restore volar tilt (minimum neutral/0°), radial inclination, and radial length.
Post-reduction: Double sugar-tong splint (NOT circumferential cast for 24 hrs - edema risk). Orthopedic follow-up in 2-3 days.
Surgical (ORIF / percutaneous K-wires / external fixator)
Indications:
- Failed or unstable closed reduction
- Intraarticular fractures with >2 mm step-off
- Open fractures
- Neurovascular compromise
- Dominant hand in high-demand patient
Comparison with Related Fractures
| Feature | Colles | Smith's | Barton's |
|---|---|---|---|
| Displacement | Dorsal | Volar ("reverse Colles") | Volar articular fragment |
| Deformity | Dinner fork | Garden spade | - |
| Mechanism | FOOSH (extension) | Fall on flexed wrist | Fall on wrist |
| Articular | Usually extra-articular | Usually extra-articular | Intra-articular |
Complications
Early:
- Median nerve injury (most common nerve - carpal tunnel syndrome acutely)
- Vascular injury (rare)
- Tendon damage
Late (6-80% complication rate):
- Malunion (most common late complication) - "dinner fork" persists
- Carpal tunnel syndrome (delayed - most common late complication)
- Sudeck's atrophy / Complex Regional Pain Syndrome (CRPS / RSDS)
- Stiff, weak, painful wrist
- Rupture of extensor pollicis longus (EPL) tendon (at Lister's tubercle)
- Radioulnar joint instability
- Radiocarpal arthritis
- Shoulder-hand syndrome
Iatrogenic:
- Median nerve damage from splinting in extreme flexion
- Conversion to open fracture (thin skin over fracture)
Key memory: factors predicting disability = dorsal angulation ≥20° + radial shortening ≥5 mm
Pediatric Equivalent
In children, the equivalent is displacement of the lower radial epiphysis (Salter-Harris Type I/II physeal injury) - fragment displaces dorsally, similar mechanism. Only severe displacement needs reduction; 3 weeks in dorsal slab is sufficient.
Key Viva Points Summary
| Question | Answer |
|---|---|
| Definition | Transverse fracture distal radius within 2.5 cm of articular surface, dorsal displacement |
| Most common in | Post-menopausal osteoporotic women |
| Mechanism | FOOSH |
| Classic deformity | Dinner fork / Silver fork |
| Most common nerve injured | Median nerve |
| Most common associated fracture | Ulnar styloid (~60%) |
| Indicates TFCC injury | Ulnar styloid fracture |
| Anesthesia for reduction | Hematoma block (commonest), Bier block, regional |
| Position after reduction | Slight palmar flexion + ulnar deviation (NOT extreme flexion) |
| Immobilization | Dorsal slab → short arm cast 4-6 weeks |
| Unstable if... | Angulation >20°, shortening >5 mm, intraarticular, comminuted |
| Most common late complication | Malunion / CTS / CRPS |
| EPL rupture site | Lister's tubercle |
| Pediatric equivalent | Distal radial epiphysis displacement |
| Reverse Colles | Smith's fracture (volar angulation) |
| Classification | Gartland & Werley Groups 1-3 |
Sources: Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Pye's Surgical Handicraft 22nd Ed; Pfenninger & Fowler's Procedures for Primary Care; Campbell's Operative Orthopaedics 15th Ed (2026)
This is a shared conversation. Sign in to Orris to start your own chat.