Diagnosis of tb Full details for md exams 15marks
Reading File
search_medical_text
tuberculosis diagnosis clinical features investigations sputum smear culture NAAT
search_medical_text
tuberculosis chest X-ray Mantoux TST IGRA diagnosis criteria
search_medical_image
tuberculosis chest X-ray findings cavitation upper lobe
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive, exam-oriented answer on the Diagnosis of Tuberculosis suitable for a 15-mark MD/postgraduate examination.
Diagnosis of Tuberculosis (TB)
Comprehensive Answer — MD Examination (15 Marks)
1. DEFINITION
Tuberculosis is an infectious disease caused by Mycobacterium tuberculosis, primarily affecting the lungs (pulmonary TB), but capable of involving any organ (extrapulmonary TB). Diagnosis requires integration of clinical, radiological, and microbiological/immunological evidence.
2. CLINICAL DIAGNOSIS
A. Symptoms (Cardinal Features)
| Symptom | Details |
|---|---|
| Cough | > 2–3 weeks duration, initially dry, then productive |
| Hemoptysis | Blood-streaked or frank hemoptysis |
| Fever | Low-grade, typically evening rise |
| Night sweats | Drenching, characteristic |
| Weight loss | Gradual, significant (>10% body weight) |
| Anorexia | Loss of appetite |
| Fatigue/Malaise | Constitutional symptom |
| Chest pain / Dyspnea | In pleural involvement or extensive disease |
B. Signs on Examination
- Pallor, cachexia, clubbing (rare, in fibrocystic disease)
- Chest: Dullness on percussion over apex, crackles (post-tussive crepitations), bronchial breathing, amphoric breath sounds (cavity)
- Cervical lymphadenopathy (scrofula) — extrapulmonary TB
- Signs of pleural effusion: Stony dull percussion, absent breath sounds
3. RADIOLOGICAL DIAGNOSIS
A. Chest X-Ray (CXR) — First-line Investigation
Classic PA CXR Findings:
| Type | Radiological Feature |
|---|---|
| Primary TB | Ghon's focus (lower/mid zone), hilar lymphadenopathy, Ranke complex |
| Post-primary (Reactivation) | Apical/posterior upper lobe infiltrates, fibrosis, cavitation |
| Miliary TB | Diffuse bilateral 1–3 mm nodules ("millet seed" pattern) |
| Pleural TB | Unilateral pleural effusion |
| Progressive primary | Consolidation, lobar collapse (bronchial compression) |
Classic Cavitary TB on Chest X-Ray:
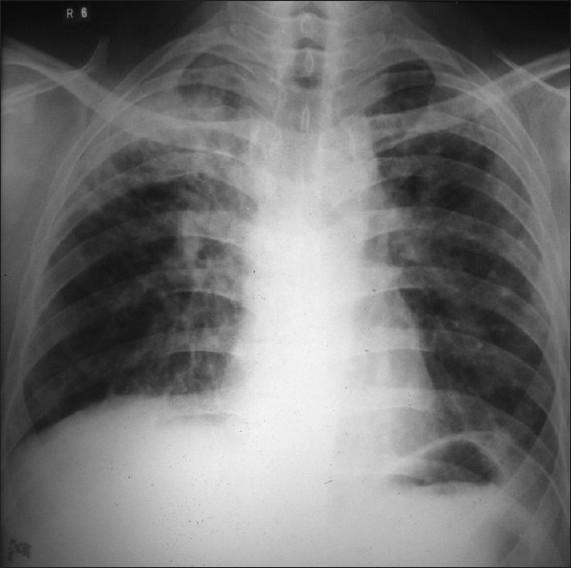
PA Chest X-ray showing right upper lobe dense heterogeneous opacities with a prominent thick-walled radiolucent cavity — classic radiographic appearance of secondary (reactivation) pulmonary tuberculosis.
B. CT Chest (High-Resolution CT)
- More sensitive than CXR
- Shows tree-in-bud pattern, centrilobular nodules, cavities, bronchiectasis
- Useful when CXR is inconclusive, or in immunocompromised patients
- Detects mediastinal lymphadenopathy
4. MICROBIOLOGICAL DIAGNOSIS
A. Sputum Specimen Collection
- 3 specimens recommended: spot → early morning → spot (or 3 consecutive early morning)
- Volume: at least 3 mL (optimal 5–10 mL)
- For smear-negative or unable to expectorate: induced sputum, bronchoscopy (BAL), gastric lavage (children)
B. AFB Smear Microscopy
- Ziehl–Neelsen (ZN) stain — detects acid-fast bacilli (appears red on blue background)
- Auramine-rhodamine fluorescence stain — more sensitive, preferred
- Grading (WHO):
| Grade | AFB/HPF |
|---|---|
| Negative | No AFB seen in 100 HPF |
| Scanty | 1–9 AFB/100 HPF |
| 1+ | 10–99 AFB/100 HPF |
| 2+ | 1–10 AFB/HPF |
| 3+ | >10 AFB/HPF |
Limitations: Sensitivity 40–60%; requires ~10,000 organisms/mL; cannot distinguish M. tuberculosis from NTM. False negatives common — a negative smear does NOT exclude TB. (ATS/IDSA Guidelines, Diagnosis of TB in Adults and Children, p. 2)
C. Mycobacterial Culture — Gold Standard
- Liquid culture (MGIT — Mycobacteria Growth Indicator Tube): results in 2–3 weeks; more sensitive
- Solid culture (Lowenstein-Jensen medium): results in 4–8 weeks; allows colony morphology
- Recommendation: Both liquid AND solid culture on all specimens (ATS/IDSA Guidelines, p. 2)
- Confirmatory identification per CLSI guidelines
- Enables DST (Drug Susceptibility Testing)
D. Nucleic Acid Amplification Tests (NAAT)
- Xpert MTB/RIF (GeneXpert) — WHO-endorsed rapid molecular test
- Detects M. tuberculosis DNA AND rifampicin resistance (surrogate for MDR-TB) simultaneously
- Result in <2 hours
- Sensitivity: ~89% in smear-positive; ~67% in smear-negative
- Specificity: >99%
- Xpert MTB/RIF Ultra — more sensitive, especially for paucibacillary disease
- Line Probe Assay (LPA / Hain GenoType MTBDRplus): Detects resistance to INH and RIF rapidly
- Recommended on initial respiratory specimen in suspected pulmonary TB (ATS/IDSA Guidelines, p. 2)
- A positive NAAT with negative smear = probable TB, confirmed by culture
- A negative NAAT with positive smear = unlikely M. tuberculosis (consider NTM)
5. IMMUNOLOGICAL TESTS
A. Tuberculin Skin Test (TST / Mantoux Test)
- Method: 5 TU (tuberculin units) of PPD (Purified Protein Derivative) intradermally into volar forearm; read at 48–72 hours
- Interpretation (induration in mm):
| Cut-off | Population |
|---|---|
| ≥ 5 mm | HIV-positive, recent TB contacts, organ transplants, immunosuppressed, fibrotic CXR changes |
| ≥ 10 mm | Recent immigrants (<5 yrs) from high-prevalence countries, injection drug users, residents/employees of high-risk facilities, mycobacteriology lab workers, children <4 years |
| ≥ 15 mm | All other persons with no risk factors |
- Limitations:
- False positive: BCG vaccination, NTM infection
- False negative: Anergy (HIV, malnutrition, steroids, miliary TB), recent viral illness, improper technique
- Cannot distinguish latent TB infection (LTBI) from active TB
- Booster phenomenon (two-step testing in elderly)
B. Interferon-Gamma Release Assays (IGRAs)
- Types: QuantiFERON-TB Gold Plus (QFT-Plus), T-SPOT.TB
- Principle: Blood test measuring IFN-γ released by sensitized T-cells after stimulation with M. tuberculosis-specific antigens (ESAT-6, CFP-10)
- Advantages over TST:
- Not affected by BCG vaccination
- Single-visit test (no 48–72 hr return needed)
- More specific
- Indications: Same as TST; preferred in BCG-vaccinated individuals
- Interpretation: Positive IGRA = evidence of M. tuberculosis infection (latent or active)
- Cannot distinguish LTBI from active TB (same as TST)
6. ADDITIONAL / SUPPORTIVE INVESTIGATIONS
A. Routine Blood Tests
| Test | Finding in TB |
|---|---|
| CBC | Normocytic normochromic anemia, lymphocytosis (early), monocytosis |
| ESR | Elevated (non-specific, monitors response) |
| CRP | Elevated |
| LFTs | Baseline before starting anti-TB drugs (hepatotoxicity risk) |
| Serum Na⁺ | Hyponatremia (SIADH in miliary/CNS TB) |
| Blood glucose | Assess for co-existing diabetes (major risk factor) |
| HIV ELISA | Mandatory in all TB patients (co-infection) |
B. Pleural Fluid Analysis (Pleural TB)
| Parameter | Typical Finding |
|---|---|
| Appearance | Straw-colored exudate |
| Protein | >3 g/dL (exudate) |
| LDH | Elevated |
| Cells | Predominantly lymphocytes |
| Glucose | Low |
| ADA (Adenosine Deaminase) | >40 U/L — highly suggestive |
| AFB smear/culture | Low sensitivity (25–30%) |
| Pleural biopsy | Caseating granulomas — most diagnostic |
C. Adenosine Deaminase (ADA)
- Produced by activated T-lymphocytes
- ADA >40 U/L in pleural fluid strongly suggests TB pleuritis
- Also used in CSF (TB meningitis) and ascitic fluid (TB peritonitis)
D. Bronchoscopy
- BAL for AFB smear + culture in smear-negative cases
- Transbronchial biopsy for endobronchial TB
- Bronchoscopic findings: mucosal hyperemia, ulceration, granulomas
E. Histopathology / Tissue Biopsy
- Caseating granuloma with Langhans' giant cells = pathognomonic of TB
- Specimens: Pleural biopsy, lymph node biopsy (FNAC/excision), liver biopsy, bone marrow biopsy (miliary TB), transbronchial biopsy
7. DIAGNOSIS OF SPECIAL FORMS
A. Smear-Negative Pulmonary TB
Diagnosis requires 3 of the following:
- Symptoms compatible with TB
- CXR consistent with TB
- No response to broad-spectrum antibiotics
- Clinical decision to treat for TB
- Positive NAAT or culture on at least one specimen
B. Latent TB Infection (LTBI)
- Positive TST or IGRA
- No clinical symptoms of active TB
- Normal CXR (or stable, old healed lesion)
- Culture negative
C. Extrapulmonary TB
| Site | Key Diagnostic Test |
|---|---|
| TB Meningitis | CSF: lymphocytosis, high protein, low glucose, ADA; CT/MRI brain (basal exudate, hydrocephalus) |
| TB Lymphadenitis | FNAC: caseating granuloma; culture |
| TB Spine (Pott's) | MRI spine: anterior wedging, paravertebral abscess, disc involvement |
| TB Peritonitis | Ascitic ADA >32 U/L; laparoscopic biopsy |
| Renal TB | Urine AFB; IVP ("putty kidney", autonephrectomy) |
| TB Pericarditis | Pericardial fluid ADA; echo-guided biopsy |
D. Miliary TB
- CXR: Bilateral diffuse 1–2 mm nodules (miliary pattern)
- HRCT chest more sensitive
- Fundoscopy: Choroidal tubercles (pathognomonic)
- Bone marrow biopsy: Granulomas with AFB
8. DIAGNOSTIC ALGORITHM (SUMMARY)
Suspected Pulmonary TB
↓
Clinical Evaluation (symptoms + signs)
↓
Chest X-Ray
↓
Sputum: AFB Smear (×3) + Xpert MTB/RIF (NAAT) + Culture (liquid + solid)
↓
┌─────────────────────────────────────────────────────────────┐
│ Smear Positive + NAAT Positive → CONFIRMED TB — Start ATT │
│ Smear Positive + NAAT Negative → Likely NTM or inhibitor │
│ Smear Negative + NAAT Positive → Probable TB — Treat │
│ Smear Negative + NAAT Negative → Culture (wait) + TST/IGRA │
│ Clinical TB (if culture negative) → Treat empirically │
└─────────────────────────────────────────────────────────────┘
↓
HIV testing (all patients)
DST (all culture-positive patients)
9. RNTCP / NTEP CLASSIFICATION (India-specific)
| Category | Definition |
|---|---|
| Bacteriologically Confirmed TB | Smear, culture, or NAAT positive |
| Clinically Diagnosed TB | Clinical + radiological evidence, no bacteriological confirmation |
| Pulmonary TB | Involves lung parenchyma |
| Extrapulmonary TB | Site other than lungs |
| New case | Never treated or <1 month ATT |
| Retreatment | Previously treated >1 month |
10. KEY EXAM POINTS
| Point | Answer |
|---|---|
| Gold standard for TB diagnosis | Culture on Lowenstein-Jensen medium |
| Rapid molecular test (WHO-endorsed) | Xpert MTB/RIF (GeneXpert) |
| Pathognomonic histological lesion | Caseating granuloma with Langhans' giant cells |
| Best stain for AFB | Auramine-rhodamine (fluorescence) |
| CXR finding pathognomonic of primary TB | Ghon's complex / Ranke complex |
| ADA cutoff for TB pleuritis | >40 U/L |
| IGRA advantage over TST | Not affected by BCG vaccination |
| Tuberculin reading time | 48–72 hours |
| Fundoscopic finding of miliary TB | Choroidal tubercles |
| Cannot distinguish LTBI from active TB | Both TST and IGRA |
References
- Diagnosis of Tuberculosis in Adults and Children — ATS/IDSA Clinical Practice Guidelines, p. 2
- Treatment of Drug-Susceptible Tuberculosis — ATS/CDC/IDSA, p. 18
- Harrison's Principles of Internal Medicine, 21st Edition
- WHO Consolidated Guidelines on Tuberculosis (2022)
- NTEP (National TB Elimination Programme) India Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.