Clinical assessment of a drowsy patient
Reading File
Finding Sources
Finding Sources
Searching PubMed
"altered consciousness" OR "drowsy patient" clinical assessment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a thorough, well-structured answer. Let me compile the comprehensive response.
Clinical Assessment of the Drowsy Patient
Why This Is an Emergency
Any alteration of consciousness - even drowsiness - is a medical emergency. The brain tolerates only limited physical or metabolic injury, and impaired consciousness signals brain failure just as uremia signals renal failure. The window for effective action is narrow. Examination and treatment must begin simultaneously. - Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Step 1: Stabilise First (ABC)
Before any formal neurological assessment, ensure the brain is receiving adequate blood and oxygen:
| Priority | Action |
|---|---|
| Airway | Open and protect; consider intubation if GCS ≤ 8 or absent gag reflex |
| Breathing | Assess rate, pattern (see respiratory patterns below), SpO2, ABG |
| Circulation | Blood pressure, heart rate, glucose (finger-stick immediately) |
| Disability | Rapid AVPU/GCS, pupils |
| Dextrose | Give 50% dextrose empirically if hypoglycaemia not excluded |
| Thiamine | 100 mg IV before glucose in any alcoholic or malnourished patient |
| Naloxone | If opioid toxidrome suspected |
Key rule: Persistent hypotension below a mean arterial pressure of ~60 mmHg is almost never caused by a primary neurological event. Search for a systemic cause. - Plum & Posner, p. 112
Step 2: Define the Level of Consciousness
Use standardised terminology and scales to communicate severity.
Spectrum of Altered Consciousness
| Term | Definition |
|---|---|
| Alert | Fully awake, aware of environment, interacts appropriately |
| Vigilant/Hyperalert | Excessively aroused; seen in delirium tremens, agitation |
| Lethargic | Drowsy but easily aroused; becomes fully aware with minimal prodding |
| Obtunded | Drowsy; requires moderate stimulation; slow responses |
| Stupor | Difficult to arouse; incomplete awareness even with strong stimulation |
| Coma | Unarousable; no spontaneous interaction; eyes closed |
From Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Rapid Bedside Scales
AVPU (quickest triage tool):
- A - Alert and oriented
- V - responds to Verbal cues
- P - responds to Pain only
- U - Unresponsive
ACDU (slightly more granular):
- Alert / Confused / Drowsy / Unresponsive
Glasgow Coma Scale (GCS)
The standard scale for trauma and most clinical settings:
| Domain | Score | Response |
|---|---|---|
| Eye | 4 | Opens spontaneously |
| 3 | Opens to voice | |
| 2 | Opens to pain | |
| 1 | No opening | |
| Motor | 6 | Obeys commands |
| 5 | Localises pain | |
| 4 | Withdraws from pain | |
| 3 | Abnormal flexion (decorticate) | |
| 2 | Extension (decerebrate) | |
| 1 | No response | |
| Verbal | 5 | Oriented |
| 4 | Confused | |
| 3 | Inappropriate words | |
| 2 | Incomprehensible sounds | |
| 1 | None |
- GCS 13-15: Mild brain injury
- GCS 9-12: Moderate brain injury
- GCS ≤ 8: Severe brain injury; secure the airway
FOUR Score (Full Outline of Unresponsiveness): More neurologically detailed than GCS, captures brainstem reflexes and can detect locked-in syndrome.
| Domain | 4 (best) | 0 (worst) |
|---|---|---|
| Eye | Open, tracking, blinking to command | Closed despite pain |
| Motor | Thumbs-up/fist/peace sign | No motor response |
| Brainstem | Pupil + corneal reflexes intact | Absent pupil, corneal, cough reflexes |
| Respiration | Not intubated, regular pattern | Breathes at ventilator rate or apnoeic |
Step 3: History (from Witnesses/Relatives/EMS)
The patient cannot give a history - this information must come from others:
- Onset: Abrupt vs. gradual
- Abrupt in a young patient: drug poisoning, subarachnoid haemorrhage, head trauma
- Abrupt in the elderly: cerebral haemorrhage or infarction
- Gradual: metabolic disorders, space-occupying lesions
- Recent complaints: Headache, focal weakness, vertigo, fever, confusion
- Recent injury or falls
- Past medical history: Diabetes, renal failure, liver disease, cardiac disease, epilepsy
- Psychiatric history
- Medications and drug access: Sedatives, opioids, psychotropic drugs, insulin
- Alcohol or substance use
- Time last seen well
Step 4: General Physical Examination
Look for systemic clues before the focused neurological exam:
| Finding | Possible Cause |
|---|---|
| Fever | Infection (meningitis, encephalitis, sepsis) |
| Hypothermia | Hypothyroidism, exposure, barbiturate/alcohol toxicity |
| Hypertension + bradycardia + irregular respiration | Cushing's triad - raised ICP |
| Hypotension | Sepsis, haemorrhage, Addisonian crisis, toxins |
| Jaundice | Hepatic encephalopathy |
| Uraemic frost, pericardial rub | Uraemic encephalopathy |
| Needle tracks | IV drug use |
| Periorbital bruising ("raccoon eyes"), Battle's sign, haemotympanum | Skull base fracture |
| Meningism (neck stiffness, Kernig's, Brudzinski's) | Meningitis / SAH |
| Cherry-red skin | Carbon monoxide poisoning |
| Cyanosis | Hypoxia |
| Breath odour | Alcohol, ketones (DKA), hepatic fetor, uraemia |
Step 5: Focused Neurological Examination
The goal is to determine: structural lesion (requiring urgent imaging/surgery) vs. metabolic/diffuse cause (broader workup).
5a. Pain Stimulation Methods
When the patient does not respond to voice or shaking, apply noxious stimuli in a standardised way:
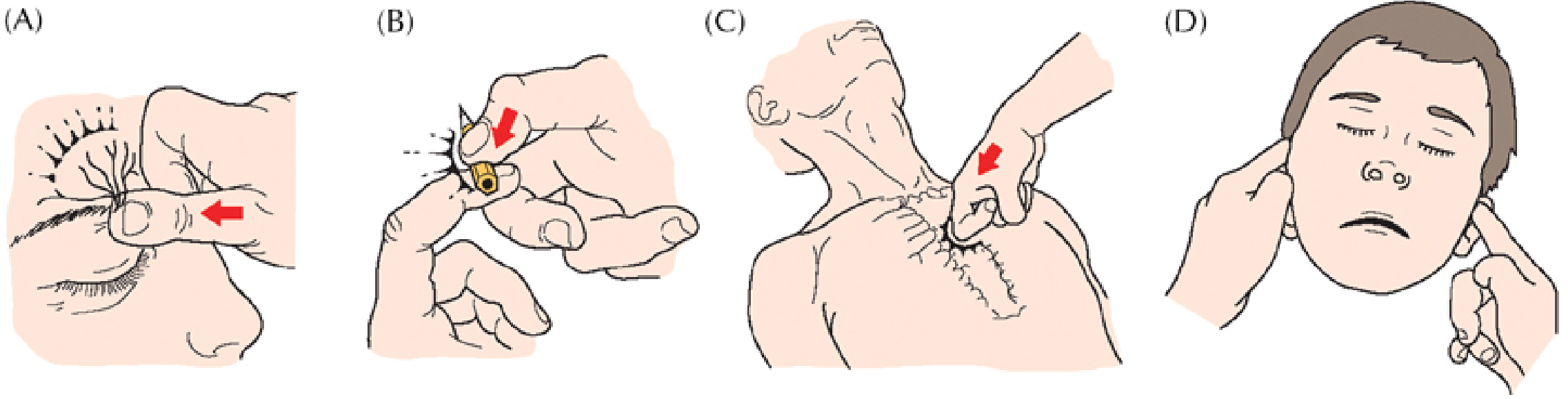
Figure: (A) Supraorbital ridge pressure, (B) nail-bed pressure, (C) sternal rub, (D) temporomandibular joint pressure. Begin with lateralised stimuli (A, B, D) to detect asymmetry; use sternal rub (C) only if no response. - Plum & Posner, Figure 2.1
5b. Pupillary Responses
Among the most diagnostically important findings:
| Pupil Finding | Interpretation |
|---|---|
| Mid-position, fixed (4-6 mm) | Midbrain lesion (tectal/tegmental); metabolic causes possible |
| Unilateral fixed, dilated | CN III compression - uncal herniation (surgical emergency) |
| Bilateral fixed, dilated | Severe midbrain damage; also atropine/sympathomimetic toxicity |
| Bilateral pinpoint, reactive | Pontine haemorrhage; opioid toxicity |
| Small, reactive (miosis) | Metabolic/bilateral diencephalic; opioids |
| Hippus (rhythmic fluctuation) | Generally indicates intact midbrain |
| Asymmetric pupils (anisocoria) | Structural lesion until proven otherwise |
5c. Ocular Movements
- Resting position: Conjugate deviation toward a hemisphere lesion; away from a pontine lesion ("eyes look at the lesion vs. away from the lesion")
- Oculocephalic reflex (doll's eyes): Intact = brainstem pathways functional
- Caloric testing (COWS): Cold water → eyes deviate toward; most sensitive brainstem test
- Dysconjugate gaze: Suggests structural brainstem pathology
5d. Motor Responses
| Response | Level of Injury |
|---|---|
| Purposeful/localising | Cortex partially intact; deep but not profoundly comatose |
| Withdrawal | Subcortical |
| Decorticate (flexion of arms, extension of legs) | Lesion above red nucleus (internal capsule, cerebral hemisphere) |
| Decerebrate (extension of arms and legs) | Lesion at midbrain/rostral pons |
| Flaccid / no response | Medulla or below; profound coma |
5e. Respiratory Patterns
| Pattern | Localisation |
|---|---|
| Cheyne-Stokes (crescendo-decrescendo) | Bilateral hemispheres or diencephalon; also heart failure |
| Central neurogenic hyperventilation | Midbrain-upper pons |
| Apneustic (prolonged inspiratory pause) | Mid-pons |
| Cluster (irregular bursts) | Lower pons |
| Ataxic (completely irregular) | Medulla - impending respiratory arrest |
Step 6: Differential Diagnosis - The Mnemonic AEIOU TIPS
A practical ED tool for organising the differential:
| Letter | Cause |
|---|---|
| A | Alcohol |
| E | Epilepsy (post-ictal state), Encephalopathy (hepatic, hypertensive) |
| I | Insulin (hypoglycaemia/hyperglycaemia), Infection |
| O | Opiates and other drugs/toxins |
| U | Uraemia and other metabolic causes |
| T | Trauma |
| I | Infection (meningitis, encephalitis, sepsis) |
| P | Poisoning (CO, medications, drugs) |
| S | Stroke / SAH / Structural lesions; Shock |
From Tintinalli's Emergency Medicine and Rosen's Emergency Medicine
Structural vs. Metabolic Causes at a Glance
| Feature | Structural | Metabolic/Toxic/Diffuse |
|---|---|---|
| Onset | Often abrupt | Usually gradual |
| Pupil abnormality | Common (asymmetric) | Usually symmetric, reactive |
| Focal deficits | Present | Absent (or symmetric) |
| Eye movements | Dysconjugate | Conjugate or absent |
| Motor signs | Asymmetric, posturing | Symmetric, tremor/asterixis |
| Imaging | Lesion visible | Usually normal early |
Step 7: Investigations
Order in parallel with the examination:
Bedside (immediate):
- Blood glucose
- SpO2, ECG, temperature
Blood tests:
- FBC, U&E (Na, K, Cr, BUN), glucose, Ca, Mg, phosphate
- LFTs, ammonia
- ABG (pH, pCO2, pO2, lactate)
- TFTs (if clinical suspicion)
- Blood cultures (if febrile)
- Serum drug levels (paracetamol, salicylate, alcohol, anticonvulsants as appropriate)
- Toxicology screen (blood and urine)
- Coagulation screen
Imaging:
- CT head (non-contrast) - first-line for any unexplained depressed consciousness; exclude haemorrhage before LP
- MRI brain if CT non-diagnostic (encephalitis, posterior fossa lesion, early infarct)
CSF (if indicated after imaging):
- Suspected meningitis, encephalitis, SAH with negative CT
EEG:
- If non-convulsive status epilepticus suspected (subtle motor movements, unexplained persistent AMS after seizure treatment)
Delirium vs. Coma: An Important Distinction
The drowsy patient may have delirium rather than coma. Key features of delirium:
- Acute fluctuating course (worsens at night - "sundowning")
- Inattention as the cardinal feature
- Perceptual disturbances (visual hallucinations, illusions)
- Three subtypes:
- Hypoactive (most missed; lethargy, decreased arousal - often mistaken for depression or "sleeping")
- Hyperactive (agitated, combative; drug-related; better prognosis)
- Mixed (~50% of cases)
- Memory impairment (time first, then place; person identity is rarely lost)
- Disrupted sleep-wake cycle
From Bradley and Daroff's Neurology in Clinical Practice
Summary: The Structured Approach
DROWSY PATIENT
|
A-B-C-D + finger-prick glucose
|
History (witness/EMS)
|
Vital signs + general exam
|
Neurological exam:
- Consciousness level (GCS/FOUR/AVPU)
- Pupils
- Eye movements
- Motor responses
- Respiratory pattern
|
Key question: STRUCTURAL vs. METABOLIC?
|
Urgent CT head (if focal signs, sudden onset, trauma, or unexplained)
+ Blood tests + Toxicology
|
Targeted treatment while awaiting results
(glucose, naloxone, thiamine, treat infection, reverse coagulopathy)
Key references:
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma (Examination of the Comatose Patient, Chapter 2)
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide (Altered Level of Consciousness)
- Rosen's Emergency Medicine: Concepts and Clinical Practice (Chapter 169 - Altered Mental Status)
- Bradley and Daroff's Neurology in Clinical Practice (Altered Level of Consciousness; Delirium subtypes)
This is a shared conversation. Sign in to Orris to start your own chat.