Cryptic miliary tb Full details for md exams 15marks
Reading File
search_medical_text
cryptic miliary tuberculosis clinical features diagnosis
search_medical_text
miliary tuberculosis management complications pathogenesis
search_medical_image
miliary tuberculosis chest X-ray CT scan findings
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive, exam-ready answer on Cryptic Miliary Tuberculosis suitable for a 15-mark MD question.
Cryptic Miliary Tuberculosis — Complete Review
Definition
Miliary tuberculosis (TB) is a form of disseminated TB resulting from hematogenous spread of Mycobacterium tuberculosis, producing uniform, discrete granulomatous lesions of 1–2 mm in multiple organs — resembling millet seeds on gross pathology, hence the name.
Cryptic miliary TB is a specific subset where:
- The classic miliary pattern on chest X-ray is absent or undetectable (hence "cryptic" = hidden)
- The tuberculin skin test (TST) / Mantoux is negative (anergic)
- The clinical presentation is atypical, insidious, and non-specific
- Diagnosis is typically made late, often at autopsy or by biopsy
It is particularly seen in elderly patients, immunocompromised hosts, and those with severe malnutrition.
Historical Context
- Described by Simmonds (1949) in elderly patients at autopsy — widespread miliary TB with no ante-mortem diagnosis
- Term "cryptic" coined to distinguish from classic miliary TB with overt radiological and clinical features
- Also called "non-reactive" miliary TB when there is minimal granuloma formation (necrosis without palisading histiocytes)
Pathogenesis
Primary / Reactivation TB focus
↓
Erosion into blood vessel (artery or vein)
↓
Hematogenous dissemination
↓
Seeding of multiple organs (lung, liver, spleen, bone marrow, kidney, adrenal, brain, eye)
↓
Formation of miliary granulomas (1–2 mm)
↓
In cryptic form: immune anergy / old age → poor granuloma formation,
no recognizable X-ray pattern, negative TST
Why cryptic?
| Factor | Mechanism |
|---|---|
| Elderly / senescent immunity | Impaired delayed hypersensitivity → no TST reaction |
| HIV/AIDS, immunosuppressants | Loss of T-cell response → false-negative IGRA/TST |
| Malnutrition | Protein depletion → anergy |
| Steroid use | Suppresses inflammatory/granuloma response |
| Overwhelming bacillemia | Exhausts immune response |
Classification of Miliary TB
| Type | CXR | TST | Granulomas | Population |
|---|---|---|---|---|
| Classic miliary TB | Miliary mottling | Positive | Well-formed | Young, previously healthy |
| Cryptic miliary TB | Normal / atypical | Negative | Poorly formed / absent | Elderly, immunocompromised |
| Non-reactive miliary TB | Normal | Negative | Necrosis without palisading | Severely immunosuppressed |
| Miliary TB in immunocompromised | Variable | Negative | Variable | HIV, transplant |
Clinical Features
General Features (Nonspecific — classic clue for exams)
Cryptic miliary TB masquerades as a PUO (Pyrexia of Unknown Origin):
- Prolonged, low-grade fever — weeks to months, not responding to broad-spectrum antibiotics
- Night sweats
- Significant weight loss and anorexia
- Progressive weakness and malaise
- No localizing signs — this is the hallmark
Organ-Specific Features
| Organ Involved | Clinical Features |
|---|---|
| Lungs | Dry cough, progressive dyspnea, occasionally ARDS |
| Liver | Hepatomegaly, raised ALP/GGT (hepatic granulomas) |
| Spleen | Splenomegaly |
| Bone marrow | Pancytopenia, leukopenia, leukaemoid reaction, thrombocytopenia |
| Adrenal glands | Features of Addison's disease (hypotension, hyponatremia, hyperkalemia) |
| Brain/Meninges | Headache, confusion, neck stiffness (TB meningitis) |
| Eyes | Choroidal tubercles (pathognomonic — seen on fundoscopy) |
| Kidney | Sterile pyuria, hematuria |
| Skin | Tuberculids, lupus vulgaris (rare) |
Exam Pearl: Choroidal tubercles on fundoscopy in a patient with PUO strongly suggest miliary TB.
Investigations
1. Hemogram
- Pancytopenia — bone marrow involvement
- Leukopenia or leukocytosis
- Monocytosis — characteristic
- Anemia (normocytic normochromic)
- Leukaemoid reaction (rare but documented)
2. ESR
- Markedly elevated (often >100 mm/hr)
3. LFTs
- Elevated ALP and GGT >> ALT/AST (granulomatous hepatitis pattern)
4. Mantoux / TST
- Negative in cryptic miliary TB (anergic) — this is key
- Negative TST does NOT exclude TB (Harrison's, p. 684)
- Repeat TST may turn positive with treatment
5. IGRA (QuantiFERON-TB Gold)
- Sensitivity similar to TST — also false-negative in miliary TB and immunosuppression (Harrison's, p. 684)
- A negative IGRA does NOT rule out miliary TB
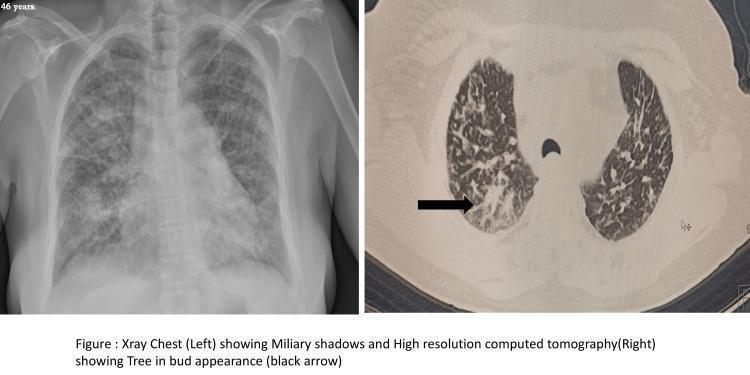
6. Chest X-Ray
- Normal in cryptic miliary TB — the defining feature
- May show subtle bilateral fine nodular shadows (1–2 mm) only in advanced disease
- Classic "snowstorm" appearance — absent in cryptic form
7. HRCT Thorax
- More sensitive than CXR — may show miliary nodules not visible on plain film
- Findings: diffuse 1–3 mm nodules in random distribution, ground-glass opacities, tree-in-bud pattern, interlobular septal thickening
8. Sputum Smear & Culture
- AFB smear: low sensitivity in miliary TB
- Culture (LJ medium / BACTEC): gold standard but takes 2–8 weeks
- GeneXpert MTB/RIF: rapid, detects MTB and rifampicin resistance (preferred if sputum available)
9. Biopsy — KEY DIAGNOSTIC TOOL
"If miliary TB is suspected, liver biopsy for acid-fast smear, culture, and PCR probably still has the highest diagnostic yield" — Harrison's, p. 684
| Biopsy Site | Yield | Notes |
|---|---|---|
| Liver biopsy | Highest | Caseating/non-caseating granulomas; AFB + PCR |
| Bone marrow biopsy | High | Granulomas + pancytopenia; send for culture |
| Transbronchial biopsy | Moderate | Useful if CXR/HRCT shows nodules |
| Lymph node biopsy | Variable | If lymphadenopathy present |
| Skin biopsy | Low | Only if skin lesions present |
Granulomatous disease in liver or bone marrow biopsy should ALWAYS prompt reconsideration of miliary TB (Harrison's, p. 684)
10. Fundoscopy
- Choroidal tubercles — pale/yellowish lesions near optic disc
- Pathognomonic of miliary TB — present in ~10–30% cases
- Should be done in every suspected case
11. CSF Analysis
- If meningism present: elevated protein, lymphocytosis, low glucose, AFB/culture/PCR
12. Urine
- Sterile pyuria → early morning urine for AFB culture
13. Serum Adenosine Deaminase (ADA)
- Elevated in TB (non-specific but supportive)
Diagnosis — Summary Algorithm
PUO + weight loss + night sweats
↓
CXR (may be NORMAL in cryptic TB)
↓
HRCT Thorax
↓
TST/IGRA (often NEGATIVE — do not rely on)
↓
Fundoscopy → choroidal tubercles?
↓
Blood counts, LFTs, bone marrow aspirate
↓
LIVER BIOPSY / BONE MARROW BIOPSY
(granulomas → AFB smear, culture, PCR)
↓
DIAGNOSIS CONFIRMED
Differential Diagnosis of Cryptic Miliary TB
| Condition | Key Differentiating Feature |
|---|---|
| Lymphoma | Lymph node biopsy: Reed-Sternberg cells |
| Sarcoidosis | Elevated ACE, bilateral hilar lymphadenopathy, TST negative but no AFB |
| Brucellosis | Rose spots, serology (Brucella agglutination) |
| Typhoid | Widal test, blood culture Salmonella typhi |
| Infective endocarditis | Murmur, echocardiography, blood culture |
| Leishmaniasis (Kala-azar) | Splenomegaly, LD bodies in bone marrow |
| Disseminated fungal infection | Cryptococcus, histoplasma antigen |
| Malignancy with hepatic mets | Biopsy, tumor markers |
Treatment
Based on expert opinion and guidelines (Treatment of Drug-Susceptible TB, p. 32):
Regimen
Standard 6-month regimen:
| Phase | Duration | Drugs | Doses |
|---|---|---|---|
| Intensive | 2 months | HRZE | Isoniazid + Rifampicin + Pyrazinamide + Ethambutol |
| Continuation | 4 months | HR | Isoniazid + Rifampicin |
- Drug doses: H = 5 mg/kg, R = 10 mg/kg, Z = 25 mg/kg, E = 15 mg/kg
CNS Involvement
- If TB meningitis co-exists: 9–12 month regimen with high-dose Rifampicin; follow TBM treatment protocol
Corticosteroids
- Prednisolone may be used as adjunct in:
- Severe respiratory failure / ARDS
- Addison's disease (adrenal insufficiency)
- TBM co-existing with miliary TB
- Role remains unclear/controversial in miliary TB without these indications (Treatment of Drug-Susceptible TB, p. 32)
Pyridoxine (Vitamin B6)
- 25 mg/day with Isoniazid to prevent peripheral neuropathy
Complications
| Complication | Notes |
|---|---|
| ARDS | Most serious pulmonary complication; high mortality |
| TB Meningitis | Indolent CNS involvement — always work up (Treatment of Drug-Susceptible TB, p. 32) |
| Addison's Disease | Bilateral adrenal destruction |
| Pancytopenia | Bone marrow failure |
| DIC | Disseminated intravascular coagulation |
| Hyponatremia | SIADH or Addison's |
| Multi-organ failure | End-stage disseminated disease |
| Paradoxical reaction | Worsening of symptoms after treatment initiation (immune reconstitution) |
Prognosis
- Mortality: 25–30% even with treatment (higher without it)
- Worse prognosis with:
- Delayed diagnosis
- ARDS
- CNS involvement
- Immunosuppression (HIV, malignancy)
- Drug-resistant TB
- Early diagnosis and prompt treatment are key to survival
Exam High-Yield Points Summary
| Key Point | Detail |
|---|---|
| Definition | Miliary TB where CXR is normal + TST negative + atypical presentation |
| Population | Elderly, immunocompromised, malnourished |
| Hallmark | PUO with no localizing signs, negative TST, normal CXR |
| Pathognomonic sign | Choroidal tubercles on fundoscopy |
| Best investigation | Liver biopsy (AFB, culture, PCR) — highest diagnostic yield |
| Bone marrow biopsy | Granulomas + pancytopenia diagnostic |
| TST/IGRA | Negative — do NOT use to exclude diagnosis |
| Treatment | 2HRZE + 4HR (6 months); 9–12 months if CNS involved |
| Steroids | Indicated for ARDS, adrenal insufficiency, TBM |
| Worst complication | ARDS, TB meningitis, multi-organ failure |
Sources: Harrison's Principles of Internal Medicine, 21st Edition (p. 684); Treatment of Drug-Susceptible Tuberculosis — CDC/IDSA Guidelines (p. 32)
This is a shared conversation. Sign in to Orris to start your own chat.