Miliary tb Full details for md exams 15marks
Reading File
search_medical_text
miliary tuberculosis pathogenesis etiology dissemination
search_medical_text
miliary tuberculosis clinical features diagnosis investigation chest X-ray
search_medical_image
miliary tuberculosis chest X-ray CT findings
GradeResponse
GradeResponse
GradeResponse
search_medical_text
miliary tuberculosis treatment antitubercular therapy corticosteroids management
search_medical_text
miliary tuberculosis complications prognosis ARDS meningitis
Here is a comprehensive, exam-ready answer on Miliary Tuberculosis suitable for a 15-mark MD question.
MILIARY TUBERCULOSIS
Definition
Miliary TB is a form of disseminated tuberculosis resulting from massive lymphohematogenous spread of Mycobacterium tuberculosis, producing uniform, discrete, 1–3 mm granulomatous lesions (resembling millet seeds) throughout one or more organs — most prominently the lungs, liver, spleen, bone marrow, meninges, and choroid.
Pathogenesis
Mechanism of Dissemination
- Primary infection: M. tuberculosis is inhaled as droplet nuclei → deposited in alveoli → ingested by alveolar macrophages.
- Containment failure: In immunocompetent hosts, a Ghon focus + caseous necrosis occurs. In susceptible individuals, the focus erodes into a blood vessel or lymphatic, releasing large numbers of bacilli.
- Lymphohematogenous spread: Bacilli disseminate via the bloodstream → seed multiple organs simultaneously.
- Granuloma formation: Each seeded focus develops into a discrete 1–3 mm granuloma ("millet seed" = milium).
- Two major pathways:
- Primary miliary TB: Progressive dissemination from a fresh primary complex (children, infants)
- Post-primary (reactivation) miliary TB: Reactivation of a latent focus → erodes into a blood vessel → systemic spread (adults, immunocompromised)
Predisposing Factors (High-risk groups)
| Group | Reason |
|---|---|
| HIV/AIDS (CD4 <200/μL) | Loss of T-cell mediated immunity |
| Malnutrition | Impaired macrophage function |
| Extremes of age (infants, elderly) | Immature or waning immunity |
| Diabetes mellitus | Defective neutrophil/macrophage function |
| Corticosteroid/immunosuppressive therapy | Suppressed CMI |
| Hematological malignancies | Impaired cellular immunity |
| Post-primary TB (reactivation) | Caseous focus eroding vessel |
| Organ transplant recipients | Iatrogenic immunosuppression |
| Pregnancy/postpartum | Relative immunosuppression |
| Silicosis | Impaired macrophage clearance |
Pathology
- Gross: Pinpoint yellow-white nodules (1–3 mm) scattered over organ surfaces (lung, liver, spleen, meninges)
- Histology: Epithelioid cell granuloma with central caseous necrosis, Langhans giant cells, surrounded by lymphocytes and fibroblasts
- Distribution in lungs: Random/hematogenous — nodules present in all zones uniformly (unlike post-primary TB which is upper-zone predominant)
Clinical Features
Presentation (Three patterns)
| Type | Features |
|---|---|
| Acute miliary TB | Most common. Acute febrile illness. |
| Subacute/Chronic miliary TB | Insidious onset, weeks–months |
| Cryptic miliary TB | Occult, elderly patients; no obvious pulmonary findings |
Symptoms
- Constitutional (universal): Prolonged fever (high, persistent, unremitting), night sweats, anorexia, weight loss, fatigue
- Respiratory (50–70%): Dry cough, progressive dyspnea, tachypnea — can progress to ARDS
- Neurological (25–40%): Headache, vomiting, altered sensorium → TB meningitis (most dangerous complication)
- Abdominal (20–30%): Hepatomegaly, splenomegaly, abdominal pain, diarrhea
- Ocular (rare but pathognomonic): Choroidal tubercles (seen on fundoscopy) — bilateral, pale, discrete lesions near optic disc
Signs
- Fever (remittent/continuous)
- Hepatosplenomegaly
- Lymphadenopathy (peripheral)
- Choroidal tubercles on fundoscopy (pathognomonic — found in ~13%)
- Signs of meningism (neck rigidity, Kernig's sign) if TB meningitis present
- Crepitations on auscultation
- Skin: Papulonecrotic tuberculid, scrofuloderma (rarely)
Investigations
1. Chest X-Ray (Key investigation)
- Classic pattern: Bilateral, symmetric, diffuse micronodular (1–3 mm) "snow-storm" or "millet-seed" pattern in all lung zones
- Nodules are uniform in size and distribution
- May be normal early in disease (first 2–3 weeks)
- Hilar/mediastinal lymphadenopathy may coexist
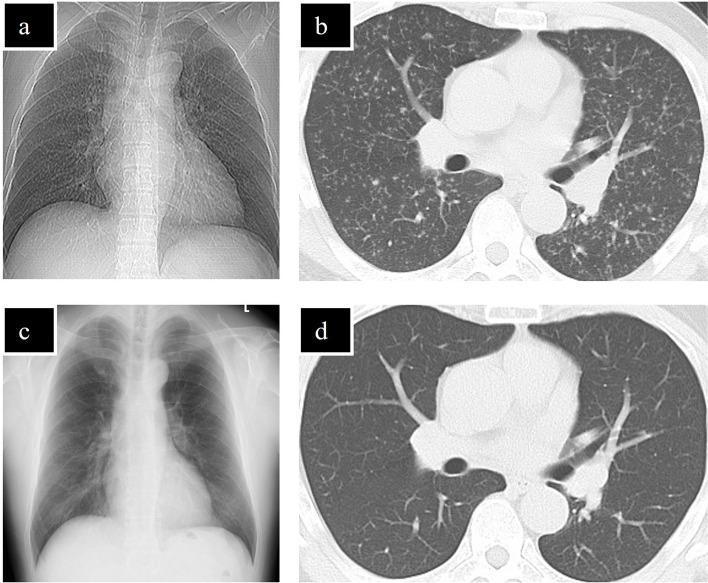
2. HRCT Chest (Gold standard imaging)
- Random micronodules (1–3 mm) with uniform distribution
- Nodules in relation to fissures, pleura, vessels (random distribution)
- Ground-glass opacities, interlobular septal thickening
- More sensitive than CXR; detects early disease
3. Sputum Examination
- AFB smear: Positive in only ~30% — often negative because lesions are hematogenous, not endobronchial
- Culture (Löwenstein-Jensen or MGIT liquid culture): Gold standard; takes 2–8 weeks
- Xpert MTB/RIF: Rapid molecular test, detects TB + rifampicin resistance in ~2 hours
4. Blood Investigations
- CBC: Leukopenia or leukocytosis; pancytopenia if bone marrow involved; anemia of chronic disease
- ESR: Markedly elevated
- LFTs: Elevated alkaline phosphatase, bilirubin (hepatic involvement)
- Hyponatremia: Due to SIADH (common)
- Hypoalbuminemia
- Serum ferritin: Markedly elevated in disseminated disease
5. Tuberculin Skin Test (Mantoux)
- Negative in 40–70% of miliary TB cases due to anergy (T-cell exhaustion/immunosuppression)
- A negative Mantoux does NOT exclude miliary TB
6. Interferon-Gamma Release Assays (IGRAs)
- QuantiFERON-TB Gold / T-SPOT.TB
- May be negative in active miliary TB due to immunosuppression
- Useful adjunct; does not differentiate latent from active TB
7. Bronchoalveolar Lavage (BAL)
- AFB smear + culture from BAL: Positive in 40–70%
- Transbronchial biopsy: Granuloma on histology is highly diagnostic
8. Biopsy (Most definitive diagnostic modality)
- Liver biopsy: Granulomas in ~80–90%; most accessible site
- Bone marrow biopsy: Granulomas; also reveals pancytopenia cause
- Lymph node biopsy (if lymphadenopathy present)
- Histology: Caseating/non-caseating epithelioid granulomas with Langhans giant cells + AFB on Ziehl-Neelsen stain
9. CSF Analysis (if CNS involvement suspected — always do LP)
| Parameter | Finding in TB Meningitis |
|---|---|
| Appearance | Clear/xanthochromic |
| Pressure | Raised |
| Cells | 100–500/μL, lymphocytic pleocytosis |
| Protein | Raised (>45 mg/dL) |
| Glucose | Low (CSF:serum ratio <0.5) |
| AFB smear | Positive in <10% |
| ADA | Elevated |
10. Fundoscopy
- Choroidal tubercles: Bilateral, creamy-yellow, discrete lesions near optic disc — pathognomonic; seen in ~13%
Diagnosis
Miliary TB is diagnosed by a combination of:
- Clinical suspicion (fever + constitutional symptoms + respiratory symptoms)
- Classic CXR/HRCT findings (diffuse 1–3 mm nodules)
- Bacteriological confirmation (AFB smear/culture/Xpert from any site)
- Histological confirmation (caseating granuloma on biopsy)
- Response to anti-TB therapy (therapeutic trial in doubtful cases)
Diagnostic certainty levels:
- Confirmed: Culture/Xpert positive or histology positive
- Probable: Classic radiology + clinical features + positive TST/IGRA
- Possible: Clinical + radiological features without microbiological/histological proof
Treatment
Anti-Tuberculosis Therapy (ATT)
Standard Regimen (WHO/RNTCP):
| Phase | Duration | Drugs |
|---|---|---|
| Intensive phase | 2 months | HRZE (Isoniazid + Rifampicin + Pyrazinamide + Ethambutol) |
| Continuation phase | 7–10 months | HR (Isoniazid + Rifampicin) |
| Total duration | 9–12 months (extended beyond standard 6 months due to severity) |
For miliary TB with TB meningitis involvement: total duration is 12 months
Drug Doses (Adult):
| Drug | Dose |
|---|---|
| Isoniazid (H) | 5 mg/kg/day (max 300 mg) |
| Rifampicin (R) | 10 mg/kg/day (max 600 mg) |
| Pyrazinamide (Z) | 25 mg/kg/day (max 2 g) |
| Ethambutol (E) | 15 mg/kg/day (max 1.6 g) |
- Add Pyridoxine (Vitamin B6) 10–25 mg/day with Isoniazid to prevent peripheral neuropathy
Corticosteroids (Adjunct Therapy)
Indications (proven to reduce mortality):
- TB meningitis (Grade 1 evidence) — Dexamethasone 0.4 mg/kg/day tapered over 6–8 weeks
- Miliary TB with ARDS — Prednisolone 1–2 mg/kg/day
- Pericardial TB
- Adrenal insufficiency (TB-related)
- Dose: Prednisolone 1–2 mg/kg/day × 4 weeks, then taper over 4–8 weeks
HIV-Coinfected Patients
- Start ATT immediately
- Start ART within 2–8 weeks of ATT (earlier in severe immunosuppression, CD4 <50)
- Use NNRTI-based ART (Efavirenz preferred); avoid Rifampicin-Protease Inhibitor combinations
- Monitor for IRIS (Immune Reconstitution Inflammatory Syndrome)
Complications
| Complication | Notes |
|---|---|
| TB Meningitis | Most serious; 20–40% mortality even with treatment |
| ARDS | Fulminant respiratory failure; high mortality |
| Pancytopenia | Bone marrow involvement |
| Adrenal insufficiency (Addison's) | Bilateral adrenal gland TB |
| Hyponatremia (SIADH) | Common; can cause seizures |
| Choroidal involvement → blindness | Rare |
| Hepatic failure | Extensive hepatic granulomas |
| Hemophagocytic syndrome | Rare; aggressive macrophage activation |
| Multi-organ dysfunction syndrome | In severe cases |
| Drug-induced hepatotoxicity | Common with HRZE; monitor LFTs |
Prognosis
- Untreated: Nearly 100% fatal
- With treatment: Mortality ~15–20% in immunocompetent patients
- Poor prognostic factors:
- HIV coinfection
- TB meningitis / ARDS
- Delayed diagnosis
- Drug resistance (MDR-TB)
- Very high bacillary load
- Extremes of age
- Organ failure at presentation
- Radiological resolution: Takes 3–6 months on treatment (as shown in imaging above)
Differential Diagnosis of Miliary Pattern on CXR
| Condition | Distinguishing Feature |
|---|---|
| Miliary TB | Uniform 1–3 mm nodules; AFB culture positive |
| Sarcoidosis | Upper-lobe predominant; bilateral hilar adenopathy; non-caseating granuloma; ACE elevated |
| Pneumocystis pneumonia | HIV patient; bilateral ground-glass; LDH elevated |
| Metastatic carcinoma | Nodules >5 mm; varied sizes; known primary |
| Hemosiderosis | History of mitral stenosis/hemoptysis |
| Histoplasmosis | Endemic area; Histoplasma serology |
| Langerhans cell histiocytosis | Young smokers; upper-lobe; cysts |
Summary Table for Quick Revision
| Feature | Key Point |
|---|---|
| Causative organism | Mycobacterium tuberculosis |
| Mechanism | Lymphohematogenous dissemination |
| Pathognomonic sign | Choroidal tubercles (fundoscopy) |
| CXR finding | Bilateral 1–3 mm micronodules — "snow-storm" |
| Best imaging | HRCT chest |
| Best diagnostic test | Liver/bone marrow biopsy (caseating granuloma) |
| Mantoux | Often negative (anergy) |
| Treatment duration | 9–12 months (2HRZE + 7–10HR) |
| Steroid indication | TB meningitis, ARDS |
| Most fatal complication | TB meningitis / ARDS |
References: Harrison's Principles of Internal Medicine, 21st Edition (pp. 4176, 5886); WHO Guidelines on Management of Tuberculosis (2022); Park's Textbook of Preventive and Social Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.