Candida tropicalis blood infection
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Candida tropicalis" AND candidemia
Reading File
Finding Sources
Searching PubMed
"Candida tropicalis" AND candidemia
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer.
Candida tropicalis Bloodstream Infection (Candidemia)
What is C. tropicalis?
Candida tropicalis is a non-albicans Candida species and a 2-6 µm yeastlike organism that reproduces by budding. Like most Candida species (except C. glabrata), it forms pseudohyphae and hyphae in tissue. It ranks among the top four causes of candidemia globally, alongside C. albicans, C. glabrata, and C. parapsilosis. In solid organ transplant recipients, C. albicans and C. tropicalis together account for ~90% of Candida infections. - Goldman-Cecil Medicine, 22nd Ed.
Epidemiology & Risk Factors
C. tropicalis candidemia follows the same risk-factor profile as candidemia in general, but it has a particularly strong association with neutropenia and hematologic malignancy:
- Neutropenic patients with hematologic cancers receiving cytotoxic chemotherapy and corticosteroids (classic host)
- ICU patients - broad-spectrum antibiotics, indwelling central venous catheters, parenteral nutrition, renal failure, dialysis, pancreatitis, high APACHE score
- Diabetes mellitus
- Recent abdominal/thoracic surgery
- Burn victims
- Solid organ transplant recipients
- HIV/AIDS (primarily mucocutaneous, but invasive in late disease)
The primary route of infection is translocation from the GI tract into the bloodstream; skin and genitourinary tract are secondary sources. - Goldman-Cecil Medicine, 22nd Ed.
A retrospective multicenter Korean cohort study noted that C. tropicalis carries a poorer prognosis than most other non-albicans Candida species in candidemia (cited in Tietz Textbook of Laboratory Medicine, 7th Ed.).
Clinical Presentation
Candidemia presents as fever in a patient with known risk factors and is often indistinguishable from bacterial sepsis. Key clinical clues suggesting dissemination:
Skin lesions (classic for C. tropicalis in neutropenic patients):
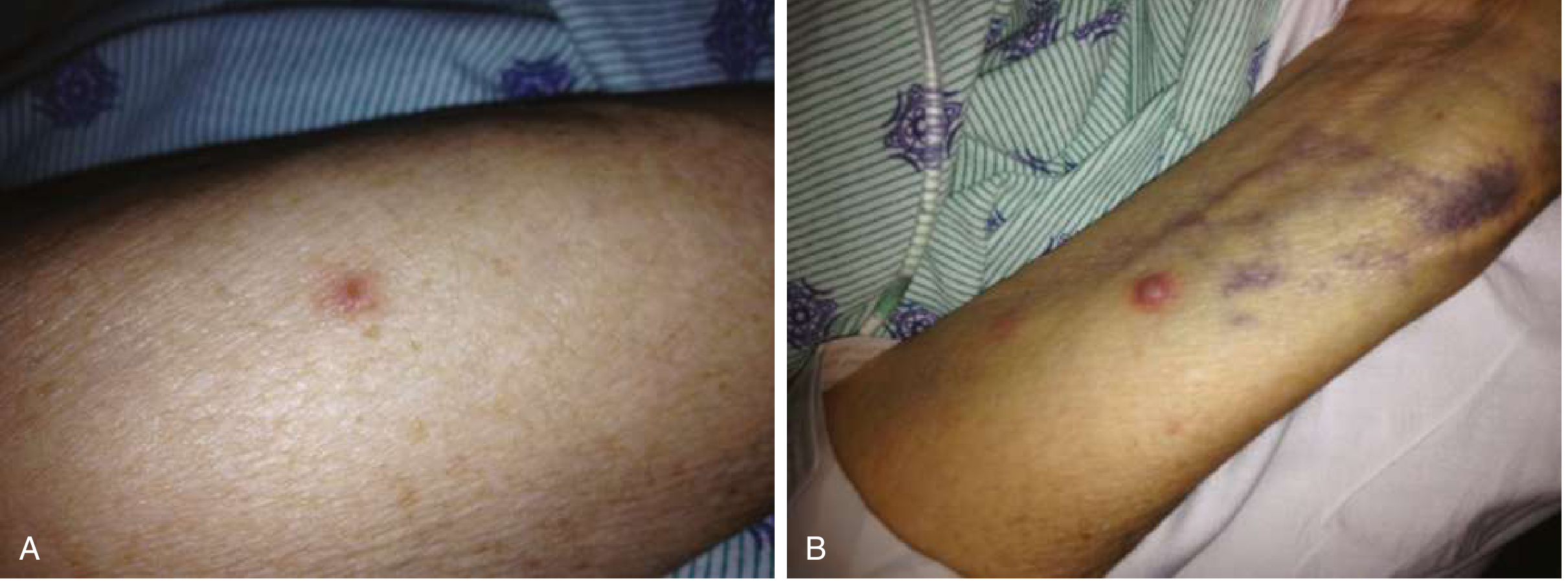
Panel A shows early tender papular lesions on the extremities in a neutropenic leukemia patient with C. tropicalis candidemia. Panel B shows progression to pustular lesions after neutropenia resolved. - Goldman-Cecil Medicine, 22nd Ed., Fig. 2.69
Other manifestations of disseminated C. tropicalis:
- Retinal lesions (Candida endophthalmitis) - can progress to endophthalmitis and blindness
- Chronic disseminated ("hepatosplenic") candidiasis - multiple microabscesses in liver/spleen, especially post-neutropenia recovery
- Candida endocarditis (rare, more common in IV drug users or prolonged candidemia)
- Osteoarticular infection, CNS involvement
Diagnosis
Blood Cultures
- Standard first-line test but not fully sensitive - up to 50% of invasive infections may be blood-culture negative
- Takes 1-4 days for growth (problematic in critically ill patients)
- All positive blood cultures for Candida require treatment - even a single positive bottle
Non-culture-based Methods
- β-D-glucan assay: Candida cell wall component; moderate sensitivity in high-risk patients; not specific (also positive in Aspergillus, PCP)
- PCR: More sensitive than blood cultures or β-D-glucan; not yet standardized widely
- Magnetic biosensor technology (newer): identifies Candida species rapidly from whole blood
Additional Workup Once Candidemia Confirmed
- Dilated fundoscopic exam (by ophthalmologist) - rule out retinal lesions in ALL candidemic patients
- Echocardiography - rule out endocarditis
- Remove and culture CVC tip - any yeast growth is significant
- Imaging (CT abdomen) - for chronic disseminated candidiasis or organ abscesses
- Repeat blood cultures - to confirm clearance
- Goldman-Cecil Medicine, 22nd Ed.
Treatment
First-line: Echinocandins (preferred for ALL patients)
| Drug | Dose |
|---|---|
| Caspofungin | 70 mg loading, then 50 mg/day IV |
| Micafungin | 100 mg/day IV |
| Anidulafungin | 200 mg loading, then 100 mg/day IV |
Echinocandins are preferred as initial therapy in both neutropenic and non-neutropenic patients, including for C. tropicalis, due to concerns about azole resistance in non-albicans species.
Fluconazole (acceptable alternative)
- 400-800 mg/day IV/oral
- Only appropriate if:
- Patient is not severely ill / hemodynamically stable
- Isolate is unlikely to be azole-resistant (C. tropicalis can develop fluconazole resistance)
- Confirmed-susceptible isolates: can step down from echinocandin to fluconazole once patient stabilizes
Step-down therapy
- After clinical stabilization + confirmed susceptible isolate: transition to fluconazole orally
- Voriconazole is an alternative step-down but offers no advantage over fluconazole
- Isavuconazole is not approved for candidemia (inferior to caspofungin in trials)
Duration
- Minimum 2 weeks after the first negative blood culture, AND resolution of symptoms/signs
- In neutropenic patients: continue until neutrophil recovery
Source Control (critical)
- Remove central venous catheter as soon as feasible - proven to hasten blood-culture clearance
- Endocarditis: lipid amphotericin B 3-5 mg/kg/day ± flucytosine 25 mg/kg QID x 6 weeks + valve replacement
Amphotericin B
-
0.7 mg/kg/day (conventional) or 3-5 mg/kg/day (lipid formulation)
-
Reserved for: neutropenic patients, neonates, severe/refractory cases, endocarditis
-
Goldman-Cecil Medicine, 22nd Ed.; Fitzpatrick's Dermatology, 5th Ed.; Red Book 2021
C. tropicalis-Specific Concerns
| Feature | Detail |
|---|---|
| Host predilection | Neutropenic patients, hematologic malignancies |
| Azole susceptibility | Can develop fluconazole resistance; susceptibility testing recommended |
| Virulence | More virulent than C. parapsilosis; associated with higher mortality vs. other non-albicans spp. |
| Skin lesions | Characteristic tender papular-to-pustular skin lesions during neutropenia |
| Prognosis | Poor compared to other non-albicans Candida in candidemia |
Summary of Management Algorithm
Suspected candidemia (fever + risk factors)
↓
Blood cultures x2 + beta-D-glucan + remove CVC
↓
Start empiric echinocandin immediately
↓
Ophthalmology exam + echo + repeat blood cultures
↓
Species identification + susceptibility testing
↓
C. tropicalis confirmed susceptible to fluconazole?
→ YES + patient stable: Step down to fluconazole
→ NO / resistant: continue echinocandin
↓
Treat 14 days from first negative blood culture
Recent literature note: A 2024 Nature Reviews Disease Primers article on invasive candidiasis (PMID 38514673) and a 2026 10-year Chinese observational study (PMID 41804483) continue to confirm C. tropicalis as a major candidemia pathogen with shifting antifungal susceptibility patterns - regular susceptibility testing remains essential.
This is a shared conversation. Sign in to Orris to start your own chat.