Tracomatis treatment
Reading File
Finding Sources
Searching PubMed
"Chlamydia trachomatis" AND treatment
Finding Sources
Reading Article
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Treatment of Chlamydia trachomatis Infections
Overview
C. trachomatis strains are susceptible to macrolides and tetracyclines. Treatment regimen depends on the clinical syndrome (genital, ocular, LGV, neonatal).
1. Uncomplicated Urogenital Infections (Cervicitis, Urethritis, Proctitis - non-LGV serovars D-K)
| Drug | Dose | Duration | Role |
|---|---|---|---|
| Doxycycline | 100 mg orally twice daily | 7 days | First-line (preferred per 2025 European guideline) |
| Azithromycin | 1 g orally | Single dose | Alternative (historically co-equal; now downgraded for most sites) |
| Ofloxacin | 300 mg orally twice daily | 7 days | Alternative |
| Levofloxacin | 500 mg orally once daily | 7 days | Alternative |
Important 2025 update: The 2025 European guideline (White et al., PMID 40037375) now recommends doxycycline as first-line in preference to single-dose azithromycin for all C. trachomatis infections. This reflects evidence of azithromycin treatment failure, particularly for rectal infections and in heterosexual men with nongonococcal urethritis.
- Erythromycin is generally not recommended due to GI side effects that compromise compliance, though it remains an option in specific circumstances.
- After treatment, patients should abstain from sex for 7 days (7-day regimen) or 7 days after single-dose therapy, until symptoms resolve and partners are treated.
2. Rectal Chlamydia (LGV and non-LGV)
- Non-LGV proctitis (serovars D-K): Same regimen as urogenital infection - doxycycline 100 mg twice daily x 7 days preferred over azithromycin (azithromycin shows lower efficacy for rectal infections).
- LGV proctitis (serovars L1, L2, L3): Doxycycline 100 mg twice daily for 21 days (3 weeks). This longer course is critical because LGV serovars are more invasive and can cause severe ulcerative proctocolitis mimicking Crohn's disease. Erythromycin is an alternative at the same dose for 3 weeks.
3. Lymphogranuloma Venereum (LGV)
- Doxycycline 100 mg orally twice daily for 21 days - drug of choice
- Erythromycin as alternative, same duration
- Azithromycin is not the preferred choice for LGV
4. Trachoma (Ocular - serovars A, B, Ba, C)
- Azithromycin single oral dose - treatment of choice
- Systemic doxycycline is also effective
- Topical therapy (tetracycline eye ointment) suppresses symptoms but does not eradicate the organism; systemic treatment is required
5. Neonatal Infections (Ophthalmia Neonatorum / Neonatal Pneumonia)
- Erythromycin (systemic) is first-line for newborns
- Topical erythromycin or silver nitrate eye prophylaxis has limited efficacy (15-25% of exposed infants still develop inclusion conjunctivitis)
- Systemic treatment is necessary to eradicate the organism
6. Special Populations
Pregnancy
- Azithromycin 1 g single dose - preferred (doxycycline is contraindicated in pregnancy)
- Amoxicillin 500 mg three times daily x 7 days is an alternative
- Untreated infection is associated with preterm birth and adverse pregnancy outcomes
Pediatric (Harriet Lane)
- Children follow adult regimens adjusted by weight; systemic erythromycin for neonatal disease
- Partners within 60 days of symptom onset should be treated; expedited partner therapy may be appropriate
7. Partner Management
- All sexual partners within 60 days prior to symptom onset (or the last sexual partner) should be tested and treated
- Expedited partner therapy is an option where legally permitted
Drug of Choice Summary
| Syndrome | First-line | Duration |
|---|---|---|
| Genital (urethritis/cervicitis) | Doxycycline 100 mg BID | 7 days |
| Rectal (non-LGV) | Doxycycline 100 mg BID | 7 days |
| LGV | Doxycycline 100 mg BID | 21 days |
| Trachoma | Azithromycin 1 g PO | Single dose |
| Neonatal | Erythromycin (systemic) | 14 days |
| Pregnancy | Azithromycin 1 g PO | Single dose |
Sources:
- Sherris & Ryan's Medical Microbiology, 8th ed.
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Harrison's Principles of Internal Medicine, 22nd ed. (2025)
- Harriet Lane Handbook, 23rd ed.
- Katzung's Basic and Clinical Pharmacology, 16th ed.
- 2025 European guideline on C. trachomatis management (White JA et al., PMID 40037375) - recommends doxycycline over azithromycin as first-line for all sites
Eye swelling with redness causes
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
I now have comprehensive data. Let me compile the full, well-organized answer.
Causes of Eye Swelling with Redness
Eye swelling with redness (periorbital erythema + edema) has two broad categories: inflammatory (usually tender) and non-inflammatory (usually non-tender). The distinction - and further narrowing by location, acuity, and associated features - guides both diagnosis and urgency.
Inflammatory Causes (Erythematous + Tender)
Common
1. Hordeolum (Stye)
Acute infection of an oil gland (meibomian or Zeiss/Moll) or eyelid hair follicle. Usually caused by Staphylococcus aureus. Presents as a painful, tender, localized red swelling on or within the eyelid margin, often with a visible pus point. Frequently associated with acute blepharitis.
2. Blepharitis
Chronic diffuse inflammation of the eyelid margins. Presents as bilateral erythema and thickening of the lid margins with crusting, itching, burning, and tearing. Telangiectasias surround the eyelid margin. Unlike preseptal cellulitis, inflammation is confined to the lid margin. Associated with rosacea, atopic dermatitis, and eczema.
- Rosen's Emergency Medicine - Blepharitis can be complicated by more diffuse periorbital cellulitis.
3. Conjunctivitis (Red Eye + Chemosis)
Inflammation of the conjunctiva causes redness, discharge, and sometimes conjunctival swelling (chemosis) that can push the eyelids out. Three major subtypes:
| Type | Key Feature | Discharge |
|---|---|---|
| Viral (adenovirus, HSV) | Watery, highly contagious, preauricular node | Watery/serous |
| Bacterial (S. aureus, H. influenzae, N. gonorrhoeae) | Copious, purulent | Mucopurulent |
| Allergic | Bilateral, intense itch, seasonal/environmental triggers | Watery, stringy mucus |
4. Preseptal (Periorbital) Cellulitis
Infection of eyelid and periocular soft tissues anterior to the orbital septum. Common in children <10 years. Presents with lid erythema, warmth, tenderness, swelling, and low-grade fever. Sources: sinusitis (especially paranasal), hordeolum, chalazion, insect bites, trauma. Organisms: S. aureus, S. epidermidis, Streptococcus spp., anaerobes. Generally benign and treated outpatient.
- Tintinalli's Emergency Medicine
5. Orbital (Postseptal) Cellulitis ⚠️ URGENT
Infection of orbital soft tissues posterior to the orbital septum. Life- and vision-threatening. Presents similarly to preseptal but has additional red flags:
- Proptosis (eye pushed forward)
- Ophthalmoplegia (restricted or painful eye movement)
- Chemosis
- Visual loss (in severe cases)
- Systemic toxicity and fever
Contrast-enhanced CT of orbits and sinuses is required to differentiate from preseptal and to identify abscess. Most often a complication of ethmoid sinusitis.
From Rosen's: "Post-septal cellulitis may be life and vision threatening and must be treated as an inpatient with IV antibiotics and occasionally surgical drainage."
6. Dacryocystitis
Infection of the lacrimal sac, usually from nasolacrimal duct obstruction. More common in females. Swelling, pain, tenderness, and erythema over the medial canthal area (medial lower eyelid). Pressure over the lacrimal sac may express purulent material through the puncta.

Fig. A - Dacryocystitis
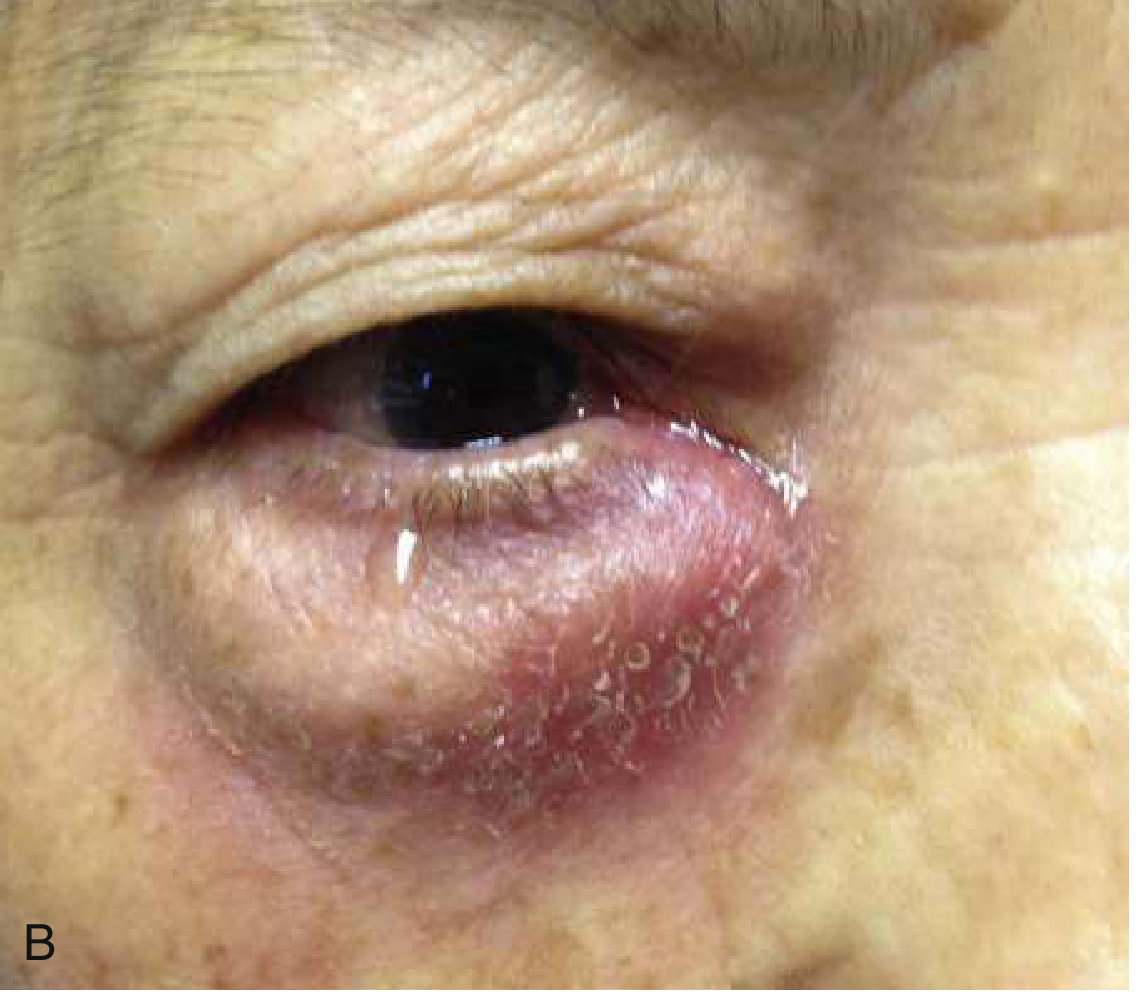
Fig. B - Dacryocystitis (Courtesy Jeffrey Lee, MD, UCSD) - from Rosen's Emergency Medicine
7. Dacryoadenitis
Infection or inflammation of the lacrimal gland (upper outer orbit). Presents as erythema, swelling, and tenderness lateral to and above the upper eyelid. Can be viral (mumps, EBV) or bacterial.
8. Contact Dermatitis / Allergic Reaction
Very common. Swollen, red, itchy eyelids with periorbital skin involvement. Most common offenders: makeup, facial moisturizers, cleansers, dyes, and perfumes. The patient may describe pain, but the skin is more likely to be itchy and inflamed without frank infection signs. Often bilateral.
- Rosen's: "Cutaneous allergic reactions and dermatitis commonly afflict the skin around the eyes as well as the eyelids."
9. Herpes Simplex (HSV) or Varicella Zoster Dermatitis
Viral vesicular rash affecting the eyelid and periorbital skin. HSV may recur. Herpes zoster ophthalmicus (VZV reactivation in the ophthalmic branch of CN V1) causes intense periorbital swelling, redness, and vesicles on the forehead/eyelid - ocular involvement requires urgent ophthalmology referral. Hutchinson's sign (vesicles on the nasal tip) predicts ocular involvement.
10. Trauma
Direct blunt trauma causes bruising, swelling, and erythema (periorbital hematoma/"black eye"). Always evaluate for underlying fracture (orbital blowout), globe injury, or hyphema.
11. Erysipelas
Superficial bacterial skin infection (Group A Streptococcus) of the face extending to periorbital skin. Sharply demarcated, raised, bright-red, warm, tender plaques.
12. Insect Bite
Localized inflammatory reaction causing periorbital swelling and erythema, sometimes disproportionately large due to the loose periorbital skin. Usually unilateral with a visible bite mark.
13. Uveitis / Episcleritis / Scleritis
These cause redness of the globe itself rather than the eyelid, but may accompany periorbital swelling. Scleritis in particular causes deep, boring eye pain with scleral injection and can be vision-threatening; it is associated with rheumatoid arthritis, lupus, and IBD.
Less Common Inflammatory Causes
- Autoimmune conditions: Discoid lupus, dermatomyositis (heliotrope rash - violaceous periorbital rash is classic)
- Ectropion with secondary inflammation
- Eyelid or lacrimal gland mass (tumor causing secondary inflammation)
- Urticaria / angioedema - rapid-onset bilateral lid swelling, often with systemic allergic features
Non-Inflammatory Causes (Swelling without Redness/Tenderness)
| Cause | Key Feature |
|---|---|
| Chalazion | Chronic, painless, non-erythematous nodule from meibomian gland granuloma |
| Prolapse of orbital fat | Soft, non-tender bulge, no erythema |
| Nephrotic syndrome / renal disease | Bilateral, dependent, pitting periorbital edema, no warmth |
| Cardiac / thyroid disease | Bilateral systemic edema; thyroid eye disease may add proptosis |
| Superior vena cava (SVC) syndrome | Bilateral facial/neck swelling with venous distension |
| Orbital tumor / lacrimal gland mass | Gradually progressive proptosis + swelling |
Key Differentiating "Red Flags" Requiring Urgent Evaluation
| Sign | Concern |
|---|---|
| Proptosis | Orbital cellulitis, orbital tumor |
| Pain with eye movement | Orbital cellulitis |
| Restricted eye movement | Orbital cellulitis, orbital apex syndrome |
| Visual loss | Orbital cellulitis, acute angle-closure glaucoma |
| Vesicles on forehead/tip of nose | Herpes zoster ophthalmicus |
| Medial canthal mass with pus expression | Dacryocystitis |
| Bilateral, systemic edema, no fever | Systemic disease (renal, cardiac) |
Sources:
- Wills Eye Manual, Office and Emergency Room Diagnosis and Treatment of Eye Disease - Eyelid Swelling differential
- Rosen's Emergency Medicine, Concepts and Clinical Practice - Periorbital infections
- Tintinalli's Emergency Medicine - Preseptal and Postseptal Cellulitis
- Harrison's Principles of Internal Medicine, 22nd ed. (2025)
Pregablain and methylcobalamine contraindications
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
pregabalin contraindications precautions drug interactions renal pregnancy
Reading File
Searching the Web
methylcobalamin contraindications precautions Leber disease polycythemia vera interactions
Reading File
I now have comprehensive information from both textbooks and authoritative sources. Let me compile the complete answer.
Contraindications and Precautions: Pregabalin & Methylcobalamin
PREGABALIN (Lyrica)
Absolute Contraindication
| Contraindication | Details |
|---|---|
| Known hypersensitivity to pregabalin or any component | The only FDA-listed absolute contraindication. Angioedema and hypersensitivity reactions have occurred (urticaria, dyspnea, wheezing). If angioedema occurs - discontinue immediately. |
Warnings & Relative Contraindications (Use with Caution / Avoid)
1. Angioedema
Swelling of the face, mouth, throat, or neck can cause life-threatening respiratory compromise. Prior history of angioedema (including from ACE inhibitors) significantly increases risk. Co-administration with ACE inhibitors (e.g., benazepril) is to be avoided - additive risk of angioedema.
2. Renal Impairment
Pregabalin is eliminated entirely by the kidneys unchanged. Dose adjustment is mandatory in all stages of renal impairment (including patients on dialysis). Failure to reduce dose leads to accumulation and toxicity. - Katzung's Basic & Clinical Pharmacology, 16th ed.
3. Pregnancy
- FDA Category C (animal studies showed fetal structural abnormalities)
- Human data suggest a possible small increase in overall major birth defects
- A pregnancy exposure registry exists
- Breastfeeding is not recommended during treatment
4. Male Fertility
Pregabalin decreases sperm count in animal studies and may impair male fertility. Animal studies show birth defects in offspring of treated males.
5. CNS Depressants (Pharmacodynamic Interaction - Avoid or Use with Extreme Caution)
Additive CNS and respiratory depression with:
- Opioids (benzodiazepines + pregabalin + opioids = high risk of fatal respiratory depression)
- Benzodiazepines
- Ethanol / alcohol
- Antihistamines, muscle relaxants, other sedatives
Limit use to patients for whom alternative options are inadequate; use the lowest effective dose.
6. Respiratory / Pulmonary Disease
Patients with COPD or pre-existing respiratory compromise are at elevated risk of respiratory depression, especially when combined with CNS depressants.
7. Suicidal Behavior and Ideation
As with all antiepileptic drugs, pregabalin carries an FDA black-box warning for increased risk of suicidal thoughts and behavior. Monitor for mood changes, depression, and unusual behavior. Use with caution in patients with a history of mood disorders or prior suicidal ideation.
8. Abrupt Discontinuation
Do not stop suddenly - may precipitate seizures (in epilepsy patients) or withdrawal symptoms (anxiety, insomnia, nausea, pain, sweating). Taper gradually.
9. Peripheral Edema / Congestive Heart Failure
Pregabalin causes peripheral edema, particularly when combined with thiazolidinediones (e.g., pioglitazone, rosiglitazone) - additive fluid retention that can worsen or precipitate congestive heart failure.
10. PR Interval Prolongation
May prolong the cardiac PR interval. Use with caution in patients with conduction abnormalities or those taking other PR-prolonging drugs.
11. Creatine Kinase Elevation / Rhabdomyolysis
Rare cases of rhabdomyolysis reported. Instruct patients to promptly report unexplained muscle pain, tenderness, or weakness, especially with fever or malaise.
12. Thrombocytopenia
Decreased platelet count has been reported (rare). Monitor in patients with bleeding disorders or on anticoagulants.
13. Ophthalmological Effects
Blurred vision, diplopia reported. Monitor for visual changes.
14. Drug/Alcohol Dependence History
Pregabalin is a Schedule V controlled substance (USA). Carefully evaluate for history of substance abuse; some patients develop tolerance, dose escalation, or drug-seeking behavior.
15. Diabetes (general caution)
Weight gain from pregabalin can worsen glycemic control. Also, peripheral edema may complicate diabetic foot monitoring.
Key Drug Interactions Summary (Pregabalin)
| Drug/Class | Interaction | Action |
|---|---|---|
| Opioids | Fatal respiratory/CNS depression | Avoid or limit |
| Benzodiazepines | Additive sedation, respiratory depression | Avoid or limit |
| Alcohol | Additive CNS depression | Avoid |
| ACE inhibitors | Additive angioedema risk | Avoid |
| Thiazolidinediones | Additive edema, worsen CHF | Monitor closely |
| Other antiepileptics | No pharmacokinetic interactions (no hepatic metabolism) | Generally safe |
METHYLCOBALAMIN (Active Vitamin B12)
Methylcobalamin has very few absolute contraindications since it is a naturally occurring coenzyme form of vitamin B12.
Absolute Contraindications
| Contraindication | Details |
|---|---|
| Hypersensitivity to methylcobalamin or cobalt | Anaphylactic shock and death have followed parenteral administration in sensitized patients. An intradermal test dose should be given if cobalt hypersensitivity is suspected before any parenteral administration. |
| Leber's hereditary optic neuropathy (early stage) | Methylcobalamin can worsen optic nerve atrophy in patients whose B12 levels are already elevated. The mechanism involves impaired mitochondrial function in an already-compromised optic nerve. Hydroxocobalamin is the preferred alternative in this population. |
Warnings & Relative Contraindications
1. Polycythemia Vera
Vitamin B12 deficiency suppresses the clinical manifestations of polycythemia vera. Correcting B12 deficiency with methylcobalamin may unmask polycythemia vera, causing a sudden rise in red cell mass. Baseline hematological evaluation is recommended before initiating treatment.
2. Hypokalemia Risk
When methylcobalamin corrects megaloblastic anemia (and red cell production suddenly accelerates), rapid uptake of potassium into new cells can cause hypokalemia, which may be severe enough to cause cardiac arrhythmia. Particularly dangerous in patients with pre-existing heart disease. Monitor serum potassium.
3. Benzyl Alcohol Preservative
Many injectable formulations of methylcobalamin contain benzyl alcohol as a preservative.
- Risk of hypersensitivity in sensitive individuals
- Contraindicated in premature neonates - benzyl alcohol causes "Gasping Syndrome" (metabolic acidosis, CNS/respiratory/circulatory/renal dysfunction - potentially fatal)
4. Folic Acid Deficiency
Methylcobalamin should not be given alone when both B12 and folate deficiencies coexist. Treating B12 deficiency without correcting folate deficiency can mask hematological improvement while neurological deterioration continues (and vice versa). Combined supplementation is typically required.
5. Iron Deficiency
Concurrent iron deficiency may blunt the hematological response to methylcobalamin. Evaluate and correct iron stores alongside B12 supplementation.
6. Pregnancy and Breastfeeding
Generally considered safe; B12 deficiency in pregnancy is harmful to the fetus. However, use should be under medical supervision and doses should not exceed recommended daily allowances unless deficiency is documented.
7. Renal Impairment (for injectable/cyanocobalamin forms)
Some injectable B12 preparations contain aluminum - accumulation possible in renal failure. This concern is more relevant to cyanocobalamin than methylcobalamin, but injectable forms should be used cautiously in severe renal impairment.
8. Oncology Patients
High-dose B12 in certain malignancies (particularly hematological) may theoretically stimulate cell proliferation. This remains largely theoretical for standard therapeutic doses.
Drug Interactions (Methylcobalamin)
| Drug | Effect |
|---|---|
| Alcohol (chronic heavy use) | Impairs B12 absorption from gut - reduces efficacy |
| Metformin | Long-term use reduces B12 absorption; monitor B12 levels |
| Proton pump inhibitors / H2 blockers | Reduce gastric acid, impairing B12 absorption from food (less relevant for oral methylcobalamin supplements) |
| Chloramphenicol | May antagonize the hematological response to B12 treatment |
| Colchicine, neomycin | Reduce B12 absorption |
Quick Summary Table
| Feature | Pregabalin | Methylcobalamin |
|---|---|---|
| Absolute CI | Hypersensitivity | Hypersensitivity/cobalt allergy; Leber's disease |
| Renal impairment | Dose reduction mandatory | Caution with injectable forms containing aluminum |
| Pregnancy | Caution (Category C) | Generally safe; use medically supervised |
| CNS depressants | Avoid / limit (fatal respiratory depression risk) | Not applicable |
| Abrupt stop | Never stop suddenly | Can stop without tapering |
| Special populations | Avoid in respiratory disease, CHF, substance abuse | Avoid in Leber's; neonates (benzyl alcohol) |
| Key unique risk | Angioedema, suicidality, PR prolongation | Unmasks polycythemia vera; hypokalemia on starting treatment |
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th ed. - Gabapentinoids section
- FDA Pregabalin Prescribing Information - Contraindications and Warnings
- StatPearls - Vitamin B12 (Cobalamin) - Contraindications
- StatPearls - Cyanocobalamin - Leber's disease, benzyl alcohol
This is a shared conversation. Sign in to Orris to start your own chat.