Post tb sequele case presentation for md final practical exam full details
Reading File
search_medical_text
post tuberculosis sequelae complications clinical features management
search_medical_text
tuberculosis destroyed lung bronchiectasis aspergilloma chronic respiratory failure
search_medical_image
post tuberculosis sequelae chest X-ray fibrosis bronchiectasis aspergilloma
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive Post-TB Sequelae Case Presentation formatted for an MD Final Practical Exam:
📋 Case Presentation: Post-Tuberculosis Sequelae
MD Final Practical Examination
🔵 CASE VIGNETTE
Patient: Mr. Ramesh Kumar, 52-year-old male
Occupation: Former construction worker
Residence: Urban slum dwelling
Presenting complaint: Progressive breathlessness + recurrent blood-stained cough for 6 months
🔵 HISTORY OF PRESENTING ILLNESS
A 52-year-old male presents with:
- Progressive exertional dyspnea for 6 months, now present at rest (MMRC Grade 3–4)
- Recurrent hemoptysis — small to moderate amounts of bright red blood
- Chronic productive cough with mucopurulent sputum
- Fatigue, weight loss, and evening rise of temperature for 3 months
- Bilateral leg swelling (ankle edema) for 1 month
History of past illness:
- Treated for pulmonary tuberculosis 10 years ago — completed a full 6-month DOTS regimen (2HRZE/4HR); declared cured
- Has had recurrent chest infections since then
- No history of diabetes, HIV, or immunosuppression
Drug history: Salbutamol inhaler as needed
Social history: Ex-smoker (30 pack-years), no alcohol
Family history: Elder brother died of TB
🔵 GENERAL PHYSICAL EXAMINATION
| Finding | Detail |
|---|---|
| Built & nourishment | Thin, malnourished |
| Pallor | Present (moderate) |
| Cyanosis | Central cyanosis (perioral) |
| Clubbing | Grade III bilateral clubbing |
| Lymphadenopathy | Absent |
| Edema | Bilateral pitting pedal edema (ankles) |
| JVP | Raised (+3 cm) |
| Temperature | 37.8°C (low-grade fever) |
| Pulse | 96/min, regular |
| RR | 26/min |
| BP | 110/70 mmHg |
| SpO₂ | 88% on room air |
Clubbing + central cyanosis + raised JVP + bilateral edema = COR PULMONALE — a classical post-TB sequela
🔵 RESPIRATORY SYSTEM EXAMINATION
Inspection
- Barrel-shaped chest (hyperinflation)
- Use of accessory muscles
- Trachea deviated to the left
- Left hemithorax — decreased movement
- Prominent intercostal spaces on right
Palpation
- Trachea: shifted LEFT (fibrosis/collapse of left upper lobe)
- Apex beat: shifted (mediastinal displacement)
- Tactile vocal fremitus: increased left upper zone, decreased left lower zone
Percussion
- Left upper zone: dull (fibrosis/consolidation)
- Left lower zone: stony dull (pleural effusion/thickening)
- Right upper zone: hyperresonant (compensatory emphysema)
Auscultation
- Left upper zone: bronchial breathing + coarse crackles
- Left lower zone: absent breath sounds (pleural thickening)
- Right side: rhonchi (obstructive component)
- Amphoric breathing over cavitary region
🔵 CARDIOVASCULAR EXAMINATION
- Loud P2 (pulmonary hypertension)
- Right ventricular heave (parasternal)
- TR murmur at tricuspid area
🔵 DIFFERENTIAL DIAGNOSIS
| Priority | Diagnosis | Reasoning |
|---|---|---|
| 1st | Post-TB sequelae (Destroyed Lung) | H/o TB, fibrosis, bronchiectasis, cavity |
| 2nd | Chronic Pulmonary Aspergillosis / Aspergilloma | Hemoptysis + residual cavity + fungal ball |
| 3rd | TB Reactivation / Re-infection | Evening fever, weight loss, hemoptysis |
| 4th | Lung Carcinoma | Smoker, weight loss, hemoptysis |
| 5th | COPD + Emphysema | Smoking history, obstructive pattern |
🔵 INVESTIGATIONS
Sputum Examination
- AFB smear × 3 (morning) — to rule out recurrence/reactivation
- Sputum culture (LJ medium / MGIT) — gold standard for active TB
- Drug sensitivity testing (DST) — if positive
- Sputum for fungal culture + KOH — for Aspergillus
- Sputum cytology — to rule out malignancy
Blood Investigations
| Test | Expected Finding |
|---|---|
| CBC | Anemia, leukocytosis |
| ESR | Elevated (>100 mm/hr) |
| CRP | Elevated |
| Serum Aspergillus IgG precipitins | Positive (chronic pulmonary aspergillosis) |
| LFT/RFT | Baseline before antifungals |
| ABG | Hypoxemia (PaO₂ <60), Hypercapnia (type II RF) |
| BNP | Elevated (cor pulmonale/RHF) |
| Blood cultures | Rule out secondary infection |
Imaging
Chest X-Ray (PA View):
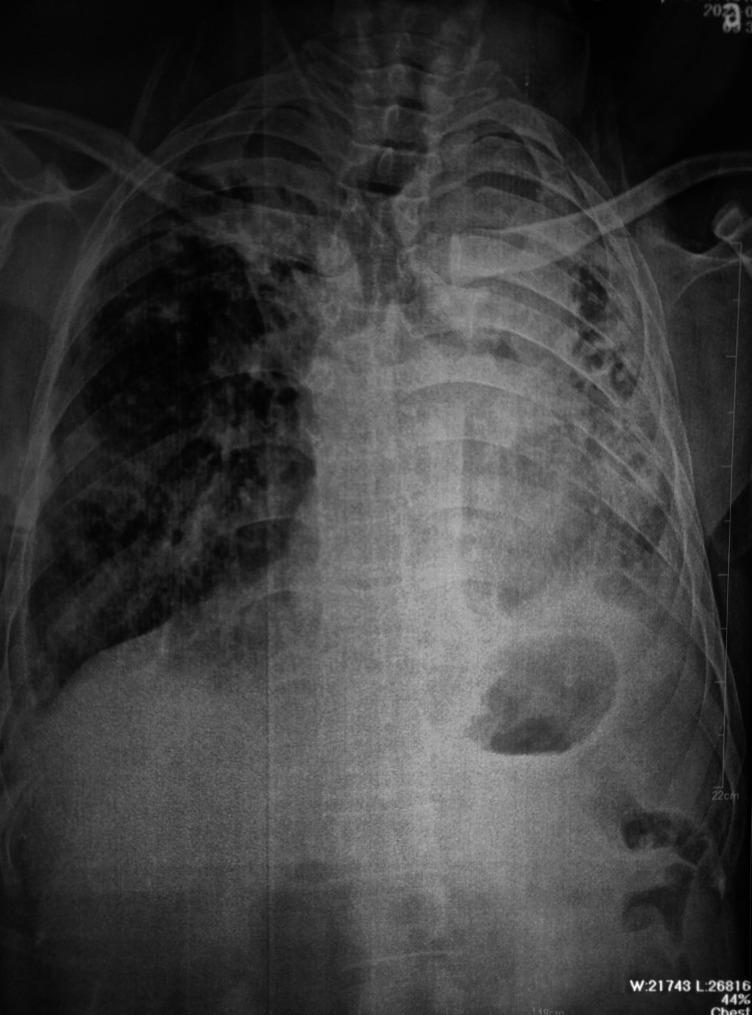
AP chest X-ray showing extensive left lung field opacification with cavitation, traction bronchiectasis, mediastinal shift to the left (volume loss), thickened cavity walls with a fungal ball (aspergilloma), and right-sided compensatory changes — consistent with post-TB destroyed lung with chronic pulmonary aspergillosis.
Expected CXR findings in Post-TB sequelae:
- Upper lobe fibrosis and volume loss
- Tracheal/mediastinal shift toward the affected side
- Pleural thickening / calcification
- Cavitary lesions (with or without Monod sign = fungal ball)
- Bronchiectatic changes
- Elevated diaphragm on affected side
HRCT Chest:
- Gold standard to assess:
- Extent of bronchiectasis (cylindrical/varicose/saccular)
- Fibrotic bands and traction changes
- Cavitary lesions with fungal ball (hyperdense rounded mass)
- Pleural thickening/calcification
- Emphysematous bullae
Echocardiography:
- Right ventricular hypertrophy
- Raised RVSP (pulmonary hypertension)
- TR jet velocity > 3.4 m/s
PFT (Pulmonary Function Tests):
- Mixed (restrictive + obstructive) pattern
- Reduced FEV1, FVC, FEV1/FVC
- Reduced DLCO (destroyed parenchyma)
🔵 DIAGNOSIS
Post-Tuberculosis Sequelae manifesting as:
- Destroyed Left Lung (fibrosis + bronchiectasis)
- Chronic Cavitary Pulmonary Aspergillosis (aspergilloma in residual cavity)
- Cor Pulmonale (secondary to chronic hypoxic pulmonary hypertension)
- Chronic Respiratory Failure (Type II)
🔵 PATHOPHYSIOLOGY (For Viva)
TB infection
↓
Granuloma formation → Caseous necrosis → Cavity formation
↓
Healing with FIBROSIS → Volume loss → Traction bronchiectasis
↓
Residual cavity → Colonized by Aspergillus fumigatus → Aspergilloma
↓
Chronic hypoxia → Pulmonary vasoconstriction → Pulmonary hypertension
↓
RV hypertrophy → Cor pulmonale → Right heart failure
🔵 MANAGEMENT
A. General Measures
- Oxygen therapy (controlled, 24–28% via Venturi mask — caution in Type II RF)
- Nutritional rehabilitation (high-protein diet)
- Pulmonary rehabilitation
- Smoking cessation
B. Specific Medical Treatment
| Condition | Treatment |
|---|---|
| Aspergilloma (simple) | Oral Itraconazole 200 mg BD for ≥6 months (Harrison's, p. 5145) — improvement in 60–75% |
| Chronic cavitary aspergillosis | IV Voriconazole (preferred) or IV Amphotericin B (if severe) |
| Hemoptysis (moderate) | Tranexamic acid, FFP; if massive → bronchial artery embolization |
| Cor Pulmonale | Diuretics (furosemide), O₂ therapy, treat underlying cause |
| Bronchiectasis | Chest physiotherapy, airway clearance, antibiotics during exacerbations |
| COPD component | LABA + LAMA (Tiotropium), ICS if indicated |
| Secondary infection | Broad-spectrum antibiotics based on culture sensitivity |
C. Surgical Options
- Surgical resection of aspergilloma — considered if:
- Massive hemoptysis unresponsive to medical/radiological treatment
- Adequate lung reserve exists
- Single localized lesion
Note: Surgery is risky due to adherent pleura and poor lung reserve (Harrison's, p. 5145) - Bronchial artery embolization (BAE) — preferred non-surgical option for massive hemoptysis
- Lung transplantation — in end-stage destroyed lung (rare, selected cases)
🔵 COMPLICATIONS OF POST-TB SEQUELAE
| Sequela | Mechanism |
|---|---|
| Bronchiectasis | Airway wall destruction + repeated infections |
| Aspergilloma | Aspergillus colonization of residual cavities |
| Hemoptysis (massive) | Rasmussen's aneurysm rupture or Aspergillus erosion |
| Restrictive lung disease | Fibrosis |
| Obstructive lung disease | Airway involvement, bronchostenosis |
| Pleural thickening/calcification | Organized pleural TB |
| Bronchopleural fistula | Cavity rupture into pleural space |
| Cor Pulmonale | Chronic hypoxia → pulmonary hypertension |
| Type II Respiratory Failure | Loss of functional lung parenchyma |
| Malignancy | Scar carcinoma (squamous cell) |
| Recurrence / Reinfection | Residual foci, immunosuppression |
| PTSD / Depression | Psychological sequelae |
🔵 PROGNOSIS
- Depends on extent of lung destruction, presence of aspergilloma, and cor pulmonale
- 5-year mortality in cor pulmonale + Type II RF is high (~50%)
- Early antifungal therapy (itraconazole ≥6 months) stabilizes/improves 60–75% of aspergilloma cases
- Regular follow-up with PFTs, CXR, and echo every 6 months
🔵 VIVA / EXAMINER QUESTIONS TO PREPARE
| Question | Key Answer |
|---|---|
| What is the most common cause of massive hemoptysis in a post-TB patient? | Aspergilloma (fungal ball) erosion of vessels / Rasmussen's aneurysm |
| What is Monod's sign? | Crescent of air around a fungal ball (aspergilloma) seen on CXR/CT — pathognomonic |
| What is Rasmussen's aneurysm? | Pseudoaneurysm of pulmonary artery branch eroded by a TB cavity |
| Drug of choice for aspergilloma? | Itraconazole 200 mg BD for ≥6 months; Voriconazole for invasive/chronic |
| Why is surgery risky in aspergilloma? | Dense pleural adhesions, poor lung reserve, high operative mortality |
| What is the treatment of massive hemoptysis? | Bronchial artery embolization (BAE) — first-line interventional therapy |
| How does cor pulmonale develop in post-TB? | Hypoxic pulmonary vasoconstriction → pulmonary HTN → RVH → cor pulmonale |
| What PFT pattern is expected? | Mixed restrictive (fibrosis) + obstructive (bronchiectasis/bronchostenosis) pattern |
| How to differentiate TB recurrence from post-TB aspergilloma? | AFB smear negative, Aspergillus IgG precipitins positive, CT showing Monod sign |
| What is destroyed lung? | Near-total loss of function of one lung due to extensive TB — fibrosis, bronchiectasis, cavitation |
🔵 SUMMARY STATEMENT (For Exam Closing)
"This is a case of a 52-year-old male with a known history of treated pulmonary tuberculosis, now presenting with progressive dyspnea, hemoptysis, and features of right heart failure. Clinical and investigative findings are consistent with post-TB sequelae in the form of a destroyed left lung with chronic cavitary pulmonary aspergillosis, complicated by type II respiratory failure and cor pulmonale. Management includes controlled oxygen therapy, oral itraconazole for aspergilloma, diuretics for cor pulmonale, and consideration of bronchial artery embolization if massive hemoptysis occurs."
Sources: Harrison's Principles of Internal Medicine, 21st Edition (p. 5145); Bailey & Love's Short Practice of Surgery, 28th Edition (p. 110); clinical knowledge supplement.
This is a shared conversation. Sign in to Orris to start your own chat.