Teach me venous infarct of brain
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cerebral venous thrombosis"[MeSH Terms] AND ("diagnosis" OR "treatment")
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
cerebral venous sinus thrombosis MRI CT imaging empty delta sign
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks plus excellent imaging. Let me compile a thorough, well-structured teaching response.
Venous Infarct of the Brain (Cerebral Venous Thrombosis / CVT)
1. Overview & Epidemiology
Cerebral venous thrombosis (CVT) is an uncommon but potentially devastating form of stroke accounting for 0.5–1% of all strokes. It is distinct from arterial stroke in its mechanism, imaging, clinical behaviour, and — importantly — its treatment. The increasing recognition of CVT is due to enhanced clinical awareness and widespread use of MRI.
- Most common in adult women, especially in association with pregnancy, the puerperium, and oral contraceptive use
- Also occurs in neonates and young infants (about half of paediatric cases)
- Rare but recognized complication of SARS-CoV-2 infection
- Incidence ~0.08% among hospitalized patients
Bradley and Daroff's Neurology in Clinical Practice — CVT constitutes 0.5–1% of all strokes; most modern cases involve adult women with puerperium or pregnancy-related risk factors.
2. Anatomy of Cerebral Venous Drainage
Understanding which veins drain which areas predicts the clinical syndrome:
| Structure | Drains |
|---|---|
| Superior sagittal sinus (SSS) | Bilateral parasagittal cortex (legs/feet region) |
| Transverse/lateral sinus | Temporal lobe convexity |
| Straight sinus | Deep structures (thalami, basal ganglia) via internal cerebral veins |
| Vein of Labbé | Superior temporal lobe |
| Vein of Trolard | Parietal cortex |
| Cavernous sinus | Orbit and frontal base |
The superior sagittal sinus is the most frequently thrombosed structure.
3. Pathophysiology
Why venous infarct differs from arterial infarct
In arterial occlusion, blood flow to the territory simply stops → cytotoxic oedema → infarction.
In venous occlusion, the sequence is:
- Sinus/vein thrombosis → outflow obstruction
- → Venous hypertension upstream in draining veins
- → Impaired perfusion pressure (arteries still deliver blood but it cannot drain)
- → Vasogenic oedema (interstitial fluid leaks from congested capillaries)
- → Blood-brain barrier breakdown → haemorrhagic transformation (very common — much more so than arterial infarct)
- → Eventually cytotoxic oedema and infarction if untreated
Key consequences of this mechanism:
- Venous infarcts are frequently haemorrhagic (fragmented, petechial haemorrhage into congested tissue)
- They do not respect arterial territory boundaries
- They are often multifocal and bilateral
- Both grey matter and subcortical white matter are affected (cortex + immediate subcortex)
- Cerebral oedema is paradoxically less prominent than in large arterial infarcts
Grainger & Allison's Diagnostic Radiology — "Reduction in parenchymal venous drainage leads to venous hypertension and subsequent infarction, which is frequently haemorrhagic."
4. Causes & Risk Factors
Aseptic CVT (the majority):
| Category | Examples |
|---|---|
| Hypercoagulable states | Protein C/S deficiency, antithrombin III deficiency, Factor V Leiden, antiphospholipid syndrome, polycythaemia, paroxysmal nocturnal haemoglobinuria |
| Hormonal | OCP, pregnancy, puerperium |
| Inflammatory/vasculitic | Behçet disease, SLE, IBD, sarcoidosis |
| Infection | Meningitis, encephalitis |
| Malignancy | Direct invasion or hypercoagulability |
| Dehydration | Especially in neonates and infants |
| Local trauma | Head injury, neurosurgery, lumbar puncture |
| COVID-19 | Vaccine-induced immune thrombocytopenia (VITT) |
| Idiopathic | ~15–20% of cases |
Septic CVT (less common today due to antibiotics):
- Cavernous sinus thrombosis: complication of facial/orbital infection → proptosis, chemosis, painful ophthalmoplegia
- Lateral sinus thrombosis: complication of otitis media/mastoiditis → headache, fever, otalgia, vertigo, papilledema, abducens palsy
Patients should be screened for thrombophilia after CVT.
5. Clinical Presentation
CVT is a great masquerader. Onset may be acute, subacute, or chronic.
Symptoms by mechanism:
Raised intracranial pressure (from impaired CSF absorption — the arachnoid granulations drain into the SSS):
- Headache (most common symptom — present in >90%) — typically diffuse, progressive, worsening over days
- Vomiting
- Papilledema
- Transient visual obscurations
- Sixth nerve palsy (false localising)
Focal brain injury (venous infarction/haemorrhage):
- Hemiparesis or paraparesis (bilateral leg weakness in SSS thrombosis — affects parasagittal motor cortex)
- Hemisensory loss
- Aphasia
- Hemianopia
- Alternating focal deficits (unusual for arterial stroke)
Cortical irritation (from congestion and haemorrhage):
- Focal or generalised seizures — very common, more so than arterial stroke
Encephalopathy (deep vein thrombosis or extensive disease):
- Lethargy, stupor, coma
- Bilateral thalamic infarction (straight sinus/internal cerebral vein thrombosis) → coma, memory loss
Adams and Victor's Principles of Neurology — "A slower evolution of the stroke syndrome than with arterial occlusion strokes, multiple cerebral lesions not in arterial territories, and a convulsive and hemorrhagic character favor venous over arterial thrombosis."
6. Syndromes by Location
| Thrombosed Structure | Classic Syndrome |
|---|---|
| Superior sagittal sinus | Bilateral leg weakness/sensory loss, raised ICP, papilledema, bilateral parasagittal haemorrhagic infarcts |
| Transverse/sigmoid sinus | Raised ICP ± temporal lobe haemorrhagic infarct |
| Straight sinus / deep system | Bilateral thalamic infarction → coma, memory impairment, hypersomnolence |
| Cavernous sinus | Proptosis, chemosis, painful ophthalmoplegia (septic > aseptic) |
| Cortical vein (isolated) | Focal cortical haemorrhagic infarct, focal seizures, no ICP rise |
| Vein of Labbé | Superior temporal lobe infarct (aphasia if dominant side) |
7. Imaging
CVT imaging has two components: (1) the thrombosed vessel itself and (2) the upstream parenchymal changes.
CT (Non-contrast)
- Dense/hyperdense sinus or vein = acute clot (the "dense triangle sign" in SSS)
- "Cord sign" = hyperdense thrombosed cortical vein on plain CT
- Haemorrhagic infarction in a non-arterial distribution
- Small ventricles (cerebral swelling)
CT with contrast (CT Venography)
- Empty delta sign (empty triangle sign): triangular filling defect (hypodense clot centre) surrounded by enhancing dural walls in the posterior SSS — the most classic CT sign
- Filling defect within sinus on CTV
- Absent opacification of sinus confirms thrombosis
MRI
- Loss of normal flow void in the sinus (normally seen as black stripe)
- Thrombosed sinus can be hyperintense on T1 and T2 (subacute thrombus — methhaemoglobin)
- Very acute thrombus can be hypointense on T2 (deoxy-Hb) — can mimic normal flow void (pitfall!)
- FLAIR/T2: high signal (oedema) in venous territory ± haemorrhage
SWI (Susceptibility-Weighted Imaging) — most sensitive
- "Blooming" = exaggerated hypointensity of thrombosed vein/sinus (beyond expected size)
- Multiple prominent serpiginous veins in the congested territory = venous hypertension
- Identifies acute haemorrhage
- Phase images can identify occluded cortical veins
MR Venography (MRV) — the gold standard
- Loss of flow signal in affected sinus
- Absence or irregularity of venous flow confirms thrombosis
- Has replaced conventional angiography for diagnosis
- Useful also for follow-up and recanalisation assessment
Parenchymal lesion distribution by sinus:
- SSS → bilateral (often asymmetric) cortical/subcortical lesions, parasagittal, parietal/frontal
- Lateral sinus → posterolateral temporal lobe, inferior parietal lobule
- Straight sinus/internal cerebral vein → bilateral thalami ± basal ganglia
- Vein of Labbé → anterolateral right temporal lobe
8. Imaging Examples
Cord Sign (MRI) + Empty Delta Sign (CTV)
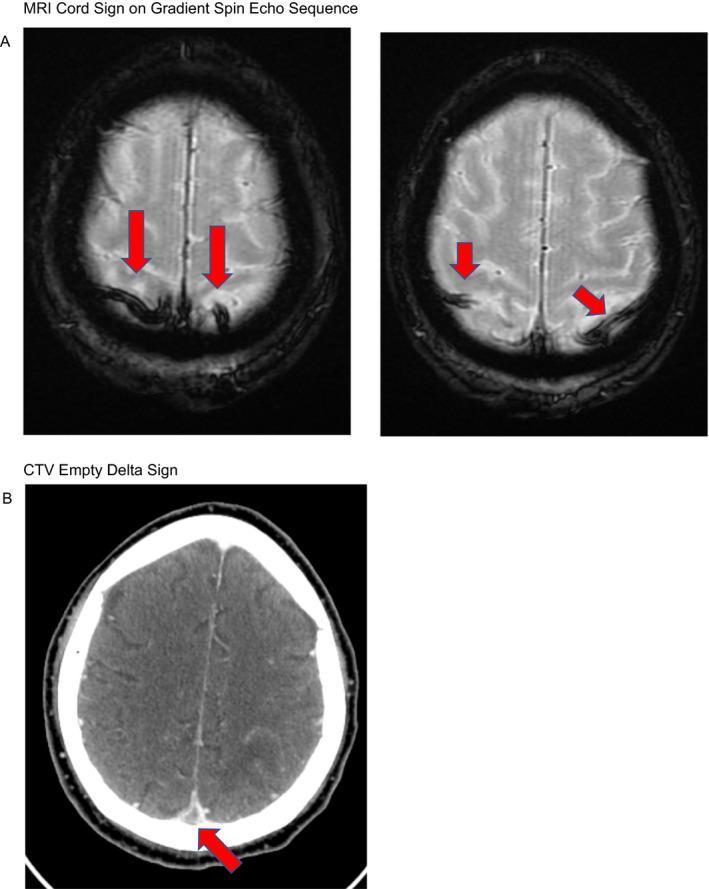
Panel A (MRI gradient echo): Red arrows show the "cord sign" — hypointense thickened cortical veins indicating acute thrombus. Panel B (CT venogram): Red arrow shows the classic "empty delta sign" — central hypodense thrombus surrounded by enhanced dural walls in the superior sagittal sinus.
CVT with Haemorrhagic Infarction (Multi-modality from Grainger & Allison)
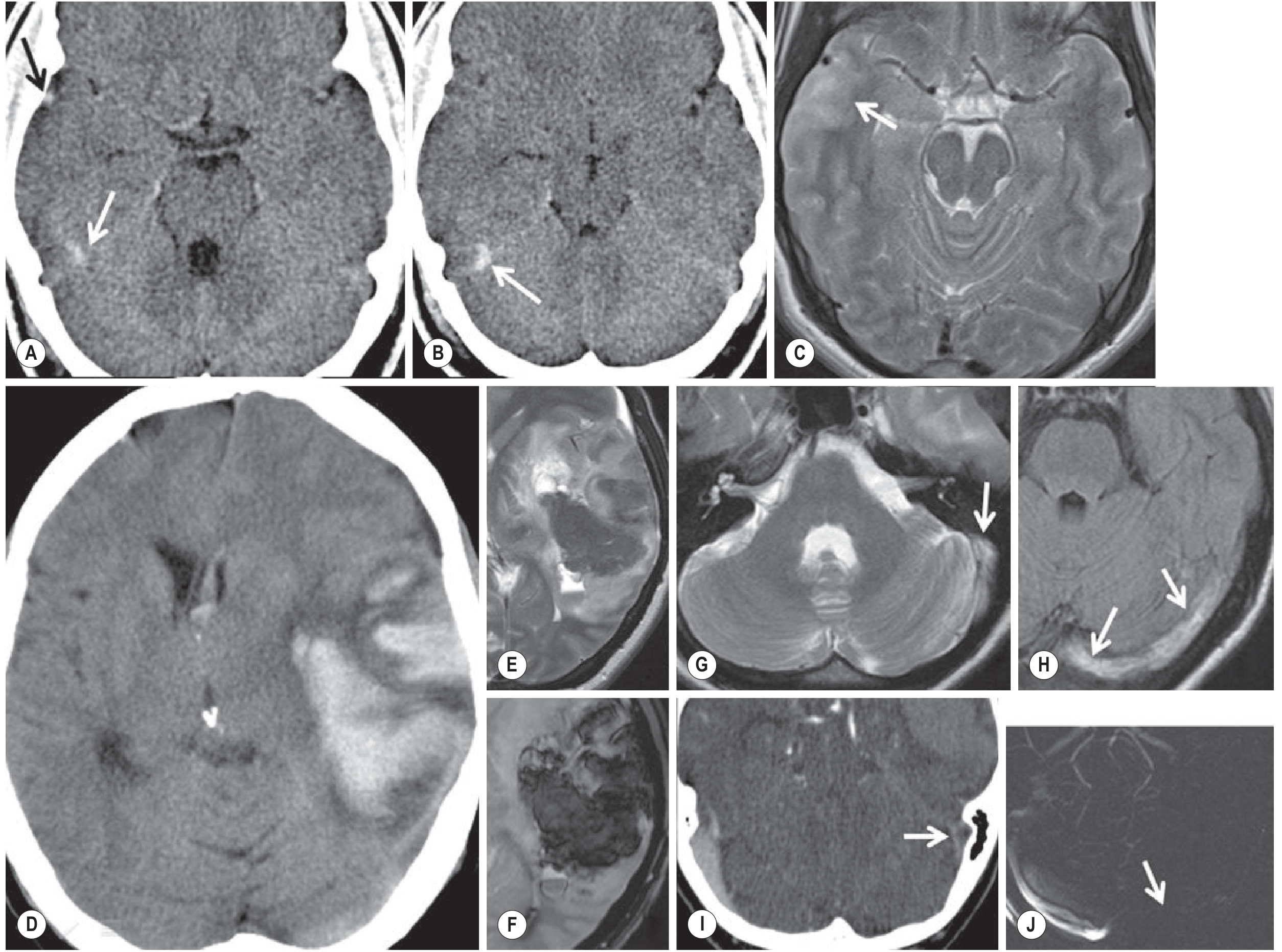
A: Cortical venous thrombosis (right vein of Labbé — serpiginous hyperdensity, black arrow; right lateral sinus, white arrows). B: Small early venous ischaemia right temporal lobe (T2W MRI). D: Large haemorrhagic left fronto-temporal venous infarct. E/F: T2/SWI — acute blood products (hypointense). G/H: Left lateral sinus thrombosis — loss of flow void on T2/FLAIR. I: CT venogram filling defect in left lateral sinus. J: SWI phase image — absent flow.
9. Diagnosis
- Clinical suspicion — headache + seizures + encephalopathy or stroke in young woman, peripartum, or OCP user
- CT/NECT — quick screening; look for dense sinus, dense cortical vein, non-arterial haemorrhage
- CT venography — excellent for major dural sinuses; shows empty delta, filling defects
- MRI + MRV — preferred combination; better for parenchymal lesions and small cortical veins
- SWI — most sensitive for cortical vein thrombosis
- DSA (conventional angiography) — now rarely needed; reserved for endovascular therapy planning
- CSF — raised opening pressure; may be xanthochromic; not required for diagnosis
- Thrombophilia screen — essential after diagnosis
MRV alone can be misleading (hypoplastic sinus vs thrombosis vs slow flow). Correlation with T1/T2/SWI is essential.
10. Treatment
Anticoagulation — cornerstone (even with haemorrhagic infarction)
This is counter-intuitive but well-established: the benefit of stopping clot propagation outweighs the risk of worsening haemorrhage.
| Phase | Drug | Notes |
|---|---|---|
| Acute | IV unfractionated heparin (UFH) or weight-adjusted LMWH SC | LMWH may have lower mortality vs UFH |
| Long-term (≥3 months) | Warfarin (INR 2.0–3.0) | Duration depends on aetiology |
| DOACs | No proven benefit over warfarin; evidence limited | May be considered (limited data) |
ICP Management
- Acetazolamide, repeated LP for raised ICP
- Head elevation, hyperventilation (short-term)
- Avoid hyperosmolar therapy if significant oedema
Anticonvulsants
- Prophylactic or therapeutic seizure medications (especially if cortical involvement/seizures present)
Antibiotics
- For septic CVT only
Escalation if deteriorating:
- Local sinus thrombolysis (urokinase/tPA via catheter) — if failing anticoagulation
- Mechanical thrombectomy of occluded sinus — endovascular option
- Decompressive craniectomy — for malignant oedema/herniation (life-saving in selective cases)
Bradley and Daroff's — "The efficacy of heparin has been shown even in patients who have evidence of intracranial hemorrhage by neuroimaging studies."
11. CVT vs Arterial Infarct — Key Differences
| Feature | Venous Infarct | Arterial Infarct |
|---|---|---|
| Territory | Non-arterial, bilateral possible | Single arterial territory |
| Haemorrhage | Common, multifocal, fragmented | Less common; uniform |
| Oedema | Vasogenic predominant, less severe | Cytotoxic, severe |
| Seizures | Very common | Less common |
| ICP rise | Common (especially SSS) | Uncommon early |
| Onset | Hours to days | Typically sudden |
| DWI restriction | Incomplete/variable | Complete/uniform in core |
| Anticoagulation | Indicated (even with haemorrhage) | Contraindicated early with haemorrhage |
12. Prognosis
- Most patients with prompt anticoagulation have good outcomes
- Mortality ~5–10% in modern series
- Recanalisation occurs in a majority
- Risk of recurrent thromboembolism — screen for underlying hypercoagulability
- Long-term anticoagulation depends on underlying cause (provoked vs unprovoked, persistent risk factors)
Sources:
- Bradley and Daroff's Neurology in Clinical Practice (Chapter 65)
- Adams and Victor's Principles of Neurology, 12th Edition (Chapter 33)
- Grainger & Allison's Diagnostic Radiology (Chapter 56)
- Goldman-Cecil Medicine, 26th Edition (Chapter 376)
- Neuroanatomy through Clinical Cases, 3rd Edition (Case 10.13)
This is a shared conversation. Sign in to Orris to start your own chat.