Write a structured well presented poin to point 15 mark answer on d/d of conductive hearing loss for my final year mbbs University proff examination of ent in pdu medical college, rajkot, gujarat, india, write what has been asked dont end trash extra things like defination epidemiology and blah blah blah
differential diagnosis conductive hearing loss causes clinical features
conductive hearing loss tuning fork tests audiometry tympanometry findings
otosclerosis CSOM ASOM otitis media with effusion wax foreign body tympanic membrane perforation hearing loss
cholesteatoma ossicular discontinuity eustachian tube dysfunction conductive hearing loss diagnosis
Differential Diagnosis of Conductive Hearing Loss
Classification Framework
A. External Ear Causes
1. Impacted Cerumen (Wax)
- Most common cause overall
- History: gradual, painless, unilateral hearing loss; often worsens after bathing (wax swells)
- Examination: brownish/yellowish plug occluding canal; no TM visible
- Rinne: Negative | Weber: Lateralizes to affected ear
- Treatment: Syringing / Aural toilet / Ear drops (sodium bicarbonate)
2. Foreign Body in External Auditory Canal (EAC)
- Common in children; also insects, cotton buds
- History: sudden onset, sometimes pain, tinnitus, sense of fullness
- Examination: FB visible on otoscopy; if insect — buzzing, severe discomfort
- Treatment: Removal under direct vision / syringing; live insects — kill with oil first
3. Otitis Externa
- Diffuse inflammation of EAC causing canal edema and debris
- History: Pain (severe), discharge, hearing loss; worsens on tragus pressure
- Examination: Canal edematous, red, tender; TM may not be visualized
- Treatment: Aural toilet + topical antibiotic + antifungal drops; systemic if severe
4. Exostoses / Osteoma of EAC
- Bony outgrowths; exostoses — bilateral, broad-based (surfers); osteoma — unilateral, pedunculated
- History: progressive hearing loss; predilection for cold-water exposure
- Examination: Hard bony swellings narrowing the canal
- Treatment: Surgical excision if symptomatic
5. Congenital Atresia of EAC
- Failure of canalization of the EAC
- History: present since birth; unilateral or bilateral
- Associated with microtia and ossicular anomalies
- Treatment: Surgical reconstruction / Bone-anchored hearing aid (BAHA)
B. Tympanic Membrane Causes
6. Traumatic Perforation of TM
- Causes: Slap, blast injury, instrumentation, barotrauma
- History: sudden pain, hearing loss, tinnitus; blood in canal
- Examination: Irregular perforation, often central; blood clot seen
- Rinne: Negative | Weber: Lateralizes to affected side
- Most heal spontaneously; large perforations → myringoplasty
7. Myringosclerosis / Tympanosclerosis
- Chalky white calcified plaques in the TM from healed inflammation
- History: previous ear infections; mild to moderate CHL
- Examination: White patches on TM; may involve ossicles (→ ossicular fixation)
C. Middle Ear Causes
8. Acute Suppurative Otitis Media (ASOM)
- History: severe earache, fever, hearing loss in a child; often preceded by URTI
- Examination: TM red, bulging, loss of landmarks; if ruptured — purulent discharge with relief of pain
- Stages: Hyperaemia → Exudation → Suppuration → Resolution / Complication
- Rinne: Negative | Weber: Lateralizes to affected ear
- Treatment: Antibiotics (Amoxicillin), analgesics; myringotomy if bulging
9. Otitis Media with Effusion (OME / Glue Ear / Secretory Otitis Media)
- Most common cause of CHL in children
- History: insidious, painless, bilateral hearing loss; usually noticed by parents/teachers
- Examination: TM dull, retracted, amber-coloured; air-fluid level or bubbles may be visible
- Tympanometry: Type B (flat) curve — pathognomonic
- Audiometry: CHL of 20–40 dB
- Treatment: Watchful waiting 3 months → Grommets (ventilation tube insertion); adenoidectomy if indicated
10. Chronic Suppurative Otitis Media (CSOM) — Tubotympanic (Safe) Type
- History: recurrent painless mucoid/mucopurulent discharge; progressive hearing loss; no pain
- Examination: Central perforation (pars tensa); TM remnant present; no cholesteatoma
- Rinne: Negative | Weber: Lateralizes to affected ear
- Audiometry: CHL 30–40 dB
- Treatment: Aural toilet + topical antibiotics (dry ear) → Myringoplasty + ossiculoplasty
11. CSOM — Atticoantral (Unsafe) Type / Cholesteatoma
- History: foul-smelling scanty discharge; progressive CHL; may have complications (facial palsy, vertigo, intracranial spread)
- Examination: Attic/posterosuperior marginal perforation; white keratinous debris (cholesteatoma); aural polyp highly suggestive
- CT Temporal Bone: Bony erosion, soft tissue mass
- CHL due to ossicular erosion (especially long process of incus)
- Treatment: Surgery (Mastoidectomy) — Canal wall up / Canal wall down; no conservative management
12. Otosclerosis
- Abnormal spongy bone formation at the Fissula ante fenestram, causing fixation of the stapes footplate
- Epidemiology: Young adult females; autosomal dominant; bilateral (70%); worsened by pregnancy
- History: Bilateral, progressive, painless CHL; paracusis Willisii (hears better in noisy surroundings)
- Examination: TM normal; Schwartze sign (flamingo pink blush through TM — active otospongiosis)
- Rinne: Negative bilaterally | Weber: Lateralizes to worse ear
- Audiometry: CHL; Carhart's notch at 2000 Hz is characteristic
- Tympanometry: Type As (shallow) curve
- Treatment: Stapedectomy / Stapedotomy (surgery of choice); sodium fluoride (medical — slows progression); hearing aid
13. Ossicular Chain Discontinuity
- Causes: Trauma (incudo-malleal or incudo-stapedial joint disruption), CSOM erosion, cholesteatoma
- History: CHL following head trauma or chronic ear disease
- Tympanometry: Type Ad (deep/floppy) curve
- Audiometry: Large air-bone gap (up to 60 dB)
- Treatment: Ossiculoplasty (TORP/PORP)
14. Glomus Tympanicum (Middle Ear Tumour)
- Paraganglioma of the middle ear
- History: Pulsatile tinnitus + CHL; low-pitched "blowing" tinnitus synchronous with pulse
- Examination: Reddish pulsatile mass behind TM; Brown's sign (blanching on pneumatic otoscopy)
- Treatment: Surgical excision; embolization pre-operatively
D. Eustachian Tube Dysfunction
15. Eustachian Tube Dysfunction (ETD)
- Impaired pressure equalization → negative middle ear pressure → retraction of TM → effusion
- History: ear fullness, muffled hearing, popping sensation; worse with altitude changes
- Causes: Adenoid hypertrophy (children), nasopharyngeal mass, cleft palate, allergic rhinitis
- Examination: Retracted TM; prominent lateral process of malleus
- Tympanometry: Type C curve (negative peak pressure)
- Treatment: Treat underlying cause; Valsalva manoeuvre; decongestants; grommet insertion
Summary Comparison Table
| Condition | TM Findings | Rinne | Tympanogram | Key Feature |
|---|---|---|---|---|
| Wax | Not visible | Negative | Normal/Type B | Brownish plug |
| ASOM | Red, bulging | Negative | Type B | Pain + fever |
| OME (Glue Ear) | Dull, retracted | Negative | Type B (flat) | Painless, children |
| CSOM Tubotympanic | Central perforation | Negative | Not performed | Mucoid discharge |
| Cholesteatoma | Attic/marginal perf. | Negative | — | Foul discharge, erosion |
| Otosclerosis | Normal | Negative (bilateral) | Type As | Carhart's notch; young female |
| Ossicular D/C | Normal / perf. | Negative | Type Ad | Trauma; large ABG |
| ETD | Retracted | Negative | Type C | Ear fullness; altitude |
| Glomus Tympanicum | Red pulsatile mass | Negative | — | Pulsatile tinnitus |
Investigations to Differentiate
- Otoscopy / Microscopy — TM status, discharge, cholesteatoma
- Pure Tone Audiometry (PTA) — Air-bone gap confirms CHL; Carhart's notch in otosclerosis
- Tympanometry — Type A (normal), As (otosclerosis), Ad (ossicular D/C), B (effusion), C (ETD)
- Acoustic Reflexes — Absent in CHL
- CT Temporal Bone (HRCT) — Cholesteatoma, otosclerosis, ossicular anomalies, glomus
- MRI — Soft tissue differentiation; glomus, petrous apex lesions
- BERA / OAE — To rule out sensorineural component (mixed hearing loss)
Examiner's Tip: Always state "Air-Bone Gap on PTA is the hallmark of CHL" and mention the specific tympanogram type for each condition. Differentiating safe vs. unsafe CSOM and highlighting surgical urgency of cholesteatoma scores extra marks.
Write a structured well presented poin to point 15 mark answer on d/d of conductive hearing loss for my final year mbbs University proff examination of ent in pdu medical college, rajkot, gujarat, india, write what has been asked dont add trash extra things like defination epidemiology and blah blah blah
differential diagnosis conductive hearing loss external ear middle ear causes clinical features
otosclerosis CSOM cholesteatoma OME otitis media audiometry tympanometry tuning fork tests
Differential Diagnosis of Conductive Hearing Loss
I. EXTERNAL EAR CAUSES
1. Impacted Cerumen (Wax)
- Symptom: Gradual, painless, unilateral hearing loss; worse after bathing (wax swells with water)
- Sign: Brownish plug on otoscopy; TM not visible
- Tuning Fork: Rinne negative, Weber lateralises to affected ear
- Treatment: Syringing / aural toilet / softening drops (sodium bicarbonate)
2. Foreign Body in EAC
- Symptom: Sudden hearing loss; common in children; live insects cause pain and loud buzzing
- Sign: FB visible on otoscopy
- Treatment: Direct removal; live insects — instill oil first to kill, then remove
3. Otitis Externa
- Symptom: Pain (severe, worsens on tragus pressure), scanty discharge, hearing loss
- Sign: Canal oedematous, red, tender; TM may not be visible due to swelling
- Treatment: Aural toilet + topical antibiotic/antifungal drops; systemic antibiotics if severe
4. Furuncle of EAC
- Symptom: Intense localised pain, tenderness, hearing loss in outer 1/3 of canal (hair-bearing area)
- Sign: Localised red swelling in outer EAC; no discharge unless ruptured
- Treatment: Analgesics, local heat, topical/systemic antistaphylococcal antibiotics; incision if pointing
5. Exostosis / Osteoma of EAC
- Symptom: Progressive hearing loss; exostoses linked to cold water exposure (surfer's ear)
- Sign: Hard bony swellings narrowing the EAC on otoscopy
- Treatment: Surgical removal if causing significant obstruction
6. Congenital Atresia of EAC
- Symptom: Present since birth; may be unilateral or bilateral
- Sign: Absent EAC; associated microtia; ossicular anomalies common
- Treatment: Surgical canaloplasty or bone-anchored hearing aid (BAHA)
II. TYMPANIC MEMBRANE CAUSES
7. Traumatic Perforation of TM
- Cause: Slap, blast, barotrauma, instrumentation (cotton bud)
- Symptom: Sudden pain, hearing loss, tinnitus; blood from ear
- Sign: Irregular perforation; blood clot in canal; TM remnants visible
- Tuning Fork: Rinne negative, Weber lateralises to affected ear
- Treatment: Most small perforations heal spontaneously; large ones → myringoplasty
8. Myringosclerosis / Tympanosclerosis
- Symptom: Mild CHL; usually follows recurrent ear infections
- Sign: Chalky white calcified plaques on TM; if ossicles involved → significant CHL
- Treatment: Surgical removal of plaques if symptomatic; ossiculoplasty if needed
III. MIDDLE EAR CAUSES
9. Acute Suppurative Otitis Media (ASOM)
- Symptom: Severe earache, fever, hearing loss; preceded by URTI; if TM perforates — pain suddenly relieved, purulent discharge appears
- Sign: TM red, bulging, loss of light reflex and landmarks
- Tuning Fork: Rinne negative, Weber lateralises to affected ear
- Tympanometry: Type B (flat)
- Treatment: Amoxicillin, analgesics; myringotomy if TM bulging with no spontaneous rupture
10. Otitis Media with Effusion (OME / Glue Ear)
- Symptom: Painless, insidious, bilateral CHL in children; often noticed by teachers/parents; no fever, no discharge
- Sign: TM dull, retracted, amber-coloured; air-fluid level or bubbles visible; prominent lateral process of malleus
- Tuning Fork: Rinne negative, Weber lateralises to worse ear
- Audiometry: CHL of 20–40 dB
- Tympanometry: Type B (flat curve) — hallmark finding
- Treatment: Watchful waiting 3 months → grommet insertion; adenoidectomy if adenoids enlarged
11. CSOM — Tubotympanic (Safe) Type
- Symptom: Recurrent painless, mucoid/mucopurulent discharge; progressive CHL; no pain, no vertigo
- Sign: Central perforation (pars tensa); TM remnant present; no cholesteatoma; no bony erosion
- Tuning Fork: Rinne negative, Weber lateralises to affected ear
- Audiometry: CHL 30–45 dB; air-bone gap present
- Treatment: Aural toilet + topical antibiotics (dry ear phase) → Myringoplasty ± ossiculoplasty (definitive)
12. CSOM — Atticoantral (Unsafe) Type / Cholesteatoma
- Symptom: Foul-smelling, scanty, persistent discharge unresponsive to antibiotics; progressive CHL; may develop facial palsy, vertigo, headache (danger signs)
- Sign: Attic or posterosuperior marginal perforation; white keratinous (cheesy) debris in attic; aural polyp is highly suggestive
- Tuning Fork: Rinne negative, Weber lateralises to affected ear
- HRCT Temporal Bone: Bony erosion, soft tissue mass in attic/antrum — investigation of choice
- Treatment: Surgery is mandatory — Mastoidectomy (canal wall up or canal wall down); no conservative management
13. Otosclerosis
- Symptom: Bilateral, progressive, painless CHL in young adult females; paracusis Willisii (hears better in noisy surroundings); worsens during pregnancy
- Sign: TM normal; Schwartze sign — flamingo-pink blush through TM in active disease (rare)
- Tuning Fork: Rinne negative bilaterally; Weber lateralises to worse ear; Absolute Bone Conduction (ABC) test — normal (distinguishes from SNHL)
- Audiometry: CHL with Carhart's notch at 2000 Hz — pathognomonic
- Tympanometry: Type As (shallow — stiffness pattern)
- Treatment: Stapedectomy / Stapedotomy (surgery of choice); sodium fluoride (slows progression); hearing aid if surgery declined
14. Ossicular Chain Discontinuity
- Cause: Head trauma (incudostapedial joint most commonly disrupted), CSOM erosion, cholesteatoma
- Symptom: Sudden/progressive CHL following trauma or chronic ear disease
- Sign: TM may be normal or show perforation depending on cause
- Audiometry: Large air-bone gap up to 60 dB — maximum possible CHL
- Tympanometry: Type Ad (deep, flaccid — hypermobile ossicular chain)
- Treatment: Ossiculoplasty (PORP / TORP)
15. Glomus Tympanicum
- Symptom: Pulsatile tinnitus synchronous with pulse + progressive CHL — classic presentation
- Sign: Reddish, pulsatile vascular mass visible behind intact TM; Brown's sign — mass blanches on pneumatic otoscopy pressure
- Investigation: HRCT temporal bone + MRI; angiography for large tumours
- Treatment: Surgical excision; pre-operative embolisation for large tumours
IV. EUSTACHIAN TUBE DYSFUNCTION
16. Eustachian Tube Dysfunction (ETD)
- Cause: Adenoid hypertrophy, nasopharyngeal mass (carcinoma — must exclude in adults), cleft palate, allergic rhinitis
- Symptom: Ear fullness, muffled hearing, popping sensation; worse with altitude change
- Sign: TM retracted; prominent lateral process and handle of malleus; no perforation
- Tympanometry: Type C (negative peak pressure — pathognomonic of ETD)
- Treatment: Treat underlying cause; Valsalva manoeuvre; nasal decongestants; grommet insertion
Quick Differentiating Summary
| Condition | TM | Discharge | Audiogram | Tympanogram | Key Feature |
|---|---|---|---|---|---|
| Wax | Not visible | None | CHL | Normal | Brownish plug |
| ASOM | Red, bulging | Purulent (if ruptured) | CHL | Type B | Pain + fever |
| OME | Dull, retracted | None | CHL 20–40 dB | Type B | Painless, children |
| CSOM Tubotympanic | Central perf. | Mucoid | CHL | — | Safe type |
| Cholesteatoma | Attic/marginal perf. | Foul, scanty | CHL | — | Bony erosion on CT |
| Otosclerosis | Normal | None | CHL + Carhart's notch | Type As | Young female, bilateral |
| Ossicular D/C | Normal/perf. | ± | CHL up to 60 dB | Type Ad | Trauma history |
| ETD | Retracted | None | CHL | Type C | Ear fullness |
| Glomus Tympanicum | Red pulsatile mass | None | CHL | — | Pulsatile tinnitus |
Key Points to Write in Exam
- Air-bone gap on PTA is the hallmark of all CHL
- Tympanogram types: B = effusion/wax, As = otosclerosis, Ad = ossicular D/C, C = ETD
- Carhart's notch at 2000 Hz = otosclerosis
- Atticoantral CSOM = always surgical; tubotympanic = medical then surgical
- Always mention nasopharyngeal carcinoma must be excluded in an adult presenting with unilateral ETD/OME
Write a structured well presented poin to point 15 mark answer on manifestation of hiv in ent specially oral for my final year mbbs University proff examination of ent in pdu medical college, rajkot, gujarat, india
HIV manifestations ENT ear nose throat head neck
HIV oral manifestations candidiasis hairy leukoplakia kaposi sarcoma aphthous ulcers
HIV oral hairy leukoplakia aphthous ulcers periodontal disease HIV gingivitis necrotizing
HIV sinusitis otitis media salivary gland lymphadenopathy neck ENT complications
HIV Kaposi sarcoma oral cavity palate treatment diagnosis
HIV laryngeal manifestations pharyngitis tonsil neck lymphoma CD4 count
Manifestations of HIV in ENT — Special Emphasis on Oral Cavity
HIV/AIDS affects the ENT system at every stage of the disease. Up to 40–70% of HIV-positive patients present with head and neck manifestations, often as the first clinical indicator of HIV infection.
STAGE-WISE ENT INVOLVEMENT
| Stage | CD4 Count | ENT Features |
|---|---|---|
| Acute seroconversion | Normal | Glandular fever-like picture — cervical lymphadenopathy, pharyngitis |
| Pre-AIDS / ARC | 200–500/μL | Otitis externa, rhinosinusitis, oral candidiasis, hairy leukoplakia |
| AIDS | <200/μL | Kaposi's sarcoma, lymphoma, CMV, severe infections |
I. ORAL MANIFESTATIONS (Most Important — Highest Yield)
1. Oral Candidiasis (Thrush) ⭐ Most Common Oral Manifestation
- Organism: Candida albicans
- CD4 trigger: Usually < 300/μL; 59% of patients develop AIDS within a year of oral candidiasis
- Types:
- Pseudomembranous (most common) — white, creamy, cheesy plaques on soft palate, buccal mucosa, tongue; wipes off leaving erythematous bleeding base
- Erythematous (atrophic) — red, flat patches on hard/soft palate or dorsum of tongue
- Angular cheilitis — cracking, redness at corners of mouth
- Diagnosis: KOH scraping shows pseudohyphae and budding yeast
- Treatment: Topical nystatin / clotrimazole; systemic fluconazole for refractory cases; treat underlying HIV with ART
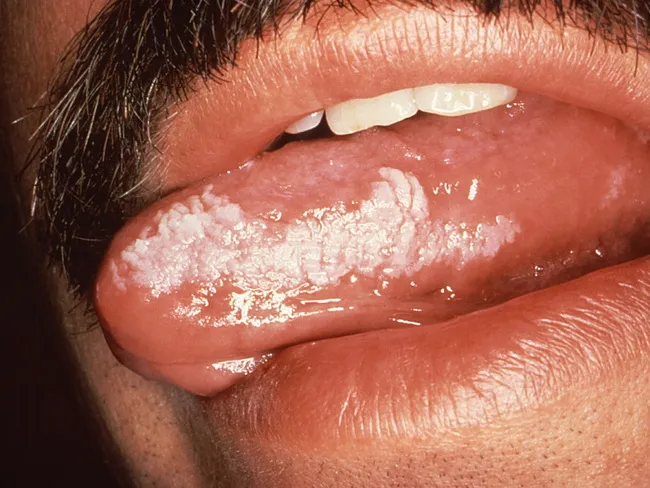
2. Oral Hairy Leukoplakia (OHL) ⭐ Pathognomonic of HIV
- Organism: Epstein-Barr Virus (EBV) reactivation
- CD4 trigger: < 300/μL
- Site: Lateral borders of tongue (bilateral) — classic location
- Appearance: White, corrugated (hairy/shaggy), vertically ridged plaques; cannot be wiped off (distinguishes from candidiasis)
- Significance: Strong predictor of HIV progression to AIDS; AIDS develops within 2–3 years in 50% of cases
- Diagnosis: Clinical; biopsy shows koilocytes, EBV in situ hybridisation
- Treatment: ART (lesions regress); high-dose acyclovir/valacyclovir for symptomatic cases
3. Aphthous Ulcers (Recurrent Aphthous Stomatitis — RAS)
- Types in HIV:
- Minor — < 1 cm, heal in 1–2 weeks
- Major — > 1 cm, deep, extremely painful, heal with scarring; more common in HIV
- Herpetiform — multiple tiny ulcers
- Site: Non-keratinised mucosa — buccal mucosa, soft palate, floor of mouth, labial mucosa
- Appearance: Round/oval, yellow-grey fibrinous base with erythematous halo
- Significance: Major aphthous ulcers in HIV are larger, deeper, more painful, slower to heal than in immunocompetent patients
- Treatment: Topical corticosteroids; thalidomide for refractory major ulcers in HIV; ART
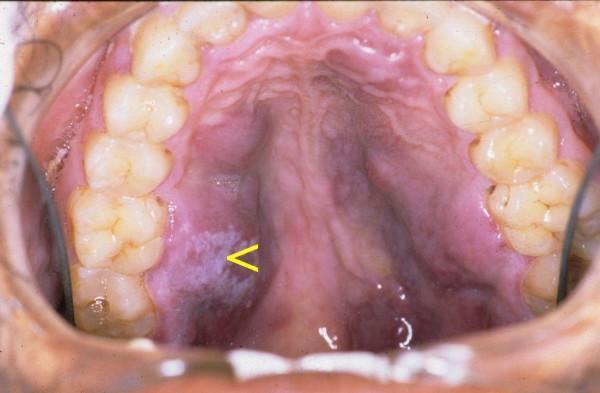
4. Kaposi's Sarcoma (KS) of Oral Cavity
- Organism: Human Herpesvirus-8 (HHV-8)
- CD4 trigger: < 200/μL
- Site: Hard palate most common intraoral site; also gingiva, tongue, buccal mucosa
- Appearance: Flat, red/violaceous (purple), painless macules → progress to raised nodules/plaques → may ulcerate and become painful
- Significance: Oral KS is often the first sign of AIDS; presence of oral KS = advanced disease
- Diagnosis: Biopsy — spindle cells, slit-like vascular spaces, extravasated RBCs
- Treatment: ART alone (early/localised); intralesional vinblastine for local lesions; systemic liposomal doxorubicin for extensive disease
5. HIV-Associated Periodontal Diseases
- Linear Gingival Erythema (LGE):
- Bright red band (2–3 mm) along the free gingival margin; disproportionate to plaque burden
- Does not respond to normal oral hygiene
- Necrotising Ulcerative Gingivitis (NUG):
- Painful, ulceration and necrosis of interdental papillae; fetid odour; bleeding
- Punched-out interdental papillae — classic sign
- Necrotising Ulcerative Periodontitis (NUP):
- Extension of NUG into alveolar bone; rapid bone destruction; tooth loss
- May progress to Necrotising Stomatitis in severe HIV
- Treatment: Metronidazole + chlorhexidine rinse; debridement; ART
6. Herpes Simplex Virus (HSV) Oral Ulcers
- CD4 trigger: < 100/μL
- Appearance: Multiple, painful, shallow ulcers on keratinised (hard palate, gingiva) and non-keratinised mucosa; perioral vesicles/crusting
- Key difference from aphthous: HSV affects keratinised mucosa; aphthous affects non-keratinised mucosa
- Treatment: Acyclovir / Valacyclovir; foscarnet for acyclovir-resistant strains
7. Oral Non-Hodgkin's Lymphoma (NHL)
- Type: High-grade B-cell lymphoma (EBV-associated)
- CD4 trigger: < 100/μL
- Site: Palate, gingiva, tongue, tonsillar area
- Appearance: Rapidly enlarging soft tissue mass; may ulcerate; painless initially
- Diagnosis: Biopsy + immunohistochemistry; CT/PET for staging
- Treatment: CHOP chemotherapy + ART; radiotherapy for localised disease
8. Salivary Gland Disease
- HIV-associated Salivary Gland Disease (HIVSGD):
- Bilateral parotid swelling (parotid most commonly affected)
- Due to lymphoepithelial cysts or diffuse infiltrative lymphocytosis syndrome (DILS)
- Xerostomia (dry mouth) — common; increases caries and candidiasis risk
- Examination: Soft, non-tender bilateral parotid enlargement
- Treatment: ART; pilocarpine for xerostomia
II. OTHER ENT MANIFESTATIONS
9. EAR
- Otitis Externa: Recurrent, often fungal (Aspergillus, Candida); severe and refractory
- Otitis Media: Recurrent ASOM; serous otitis media from Eustachian tube dysfunction
- Sensorineural Hearing Loss: Due to CMV, cryptococcal meningitis, or HIV itself (direct cochlear damage)
- Pneumocystis jirovecii Otitis:* Polypoid lesions in EAC — rare but characteristic
10. NOSE AND SINUSES
- Recurrent Rhinosinusitis: Bacterial (Pseudomonas, S. pneumoniae), fungal (invasive aspergillosis, mucormycosis in severe immunosuppression)
- Nasal Kaposi's Sarcoma: Violaceous lesions on nasal mucosa; epistaxis
- Nasal Polyps: Associated with recurrent sinusitis
11. PHARYNX AND LARYNX
- Non-specific Pharyngitis: At seroconversion — resembles infectious mononucleosis
- CMV Pharyngitis/Oesophagitis: Painful shallow ulcers; CD4 < 50/μL
- Laryngeal Candidiasis: Hoarseness; seen with advanced AIDS; odynophagia
- Laryngeal Kaposi's Sarcoma: Hoarseness, stridor, dysphagia; may cause airway compromise
12. NECK / LYMPHADENOPATHY
- Persistent Generalised Lymphadenopathy (PGL):
- Bilateral cervical, submandibular lymph nodes enlarged > 1 cm for > 3 months
- Due to follicular hyperplasia; soft, non-tender, mobile
- CD4 usually still normal at this stage
- Malignant Lymphadenopathy:
- NHL or KS involvement; nodes hard, matted, rapidly growing
- Nasopharyngeal lymphoma — presents with nasal obstruction, epistaxis, neck nodes
Summary Table — High-Yield Oral Lesions
| Lesion | Organism | Site | Cannot Wipe Off | CD4 |
|---|---|---|---|---|
| Oral Candidiasis | Candida | Soft palate, tongue | ✗ (wipes off) | < 300 |
| Oral Hairy Leukoplakia | EBV | Lateral tongue | ✓ | < 300 |
| Kaposi's Sarcoma | HHV-8 | Hard palate | ✓ | < 200 |
| Aphthous Ulcers | Immune dysregulation | Non-keratinised | — | Variable |
| HSV Ulcers | HSV-1/2 | Keratinised mucosa | — | < 100 |
| NHL | EBV/B-cell | Palate, tonsil | — | < 100 |
Key Exam Points
- OHL on lateral tongue that cannot be wiped off = Pathognomonic of HIV — always write this
- Oral candidiasis that wipes off + bleeds = Pseudomembranous type
- Hard palate violaceous lesion = Kaposi's Sarcoma until proven otherwise
- Bilateral parotid swelling in a young adult = Think HIV
- PGL = bilateral cervical lymphadenopathy > 1 cm, > 3 months, with no other cause
- ART is the backbone of treatment for ALL HIV-related ENT manifestations
Keep content exactly same just add images, i cant remember it, it js very hard to remember
oral candidiasis thrush HIV white plaques
oral hairy leukoplakia lateral tongue HIV
Kaposi sarcoma oral cavity hard palate HIV
aphthous ulcer oral HIV major minor
necrotizing ulcerative gingivitis HIV periodontal disease gingiva
HIV bilateral parotid swelling salivary gland enlargement
Manifestations of HIV in ENT — Special Emphasis on Oral Cavity
HIV/AIDS affects the ENT system at every stage of the disease. Up to 40–70% of HIV-positive patients present with head and neck manifestations, often as the first clinical indicator of HIV infection.
STAGE-WISE ENT INVOLVEMENT
| Stage | CD4 Count | ENT Features |
|---|---|---|
| Acute seroconversion | Normal | Glandular fever-like picture — cervical lymphadenopathy, pharyngitis |
| Pre-AIDS / ARC | 200–500/μL | Otitis externa, rhinosinusitis, oral candidiasis, hairy leukoplakia |
| AIDS | <200/μL | Kaposi's sarcoma, lymphoma, CMV, severe infections |
I. ORAL MANIFESTATIONS (Most Important — Highest Yield)
1. Oral Candidiasis (Thrush) ⭐ Most Common Oral Manifestation

- Organism: Candida albicans
- CD4 trigger: Usually < 300/μL; 59% of patients develop AIDS within a year of oral candidiasis
- Types:
- Pseudomembranous (most common) — white, creamy, cheesy plaques on soft palate, buccal mucosa, tongue; wipes off leaving erythematous bleeding base
- Erythematous (atrophic) — red, flat patches on hard/soft palate or dorsum of tongue
- Angular cheilitis — cracking, redness at corners of mouth
- Diagnosis: KOH scraping shows pseudohyphae and budding yeast
- Treatment: Topical nystatin / clotrimazole; systemic fluconazole for refractory cases; treat underlying HIV with ART
2. Oral Hairy Leukoplakia (OHL) ⭐ Pathognomonic of HIV
- Organism: Epstein-Barr Virus (EBV) reactivation
- CD4 trigger: < 300/μL
- Site: Lateral borders of tongue (bilateral) — classic location
- Appearance: White, corrugated (hairy/shaggy), vertically ridged plaques; cannot be wiped off (distinguishes from candidiasis)
- Significance: Strong predictor of HIV progression to AIDS; AIDS develops within 2–3 years in 50% of cases
- Diagnosis: Clinical; biopsy shows koilocytes, EBV in situ hybridisation
- Treatment: ART (lesions regress); high-dose acyclovir/valacyclovir for symptomatic cases
3. Aphthous Ulcers (Recurrent Aphthous Stomatitis — RAS)

- Types in HIV:
- Minor — < 1 cm, heal in 1–2 weeks
- Major — > 1 cm, deep, extremely painful, heal with scarring; more common in HIV
- Herpetiform — multiple tiny ulcers
- Site: Non-keratinised mucosa — buccal mucosa, soft palate, floor of mouth, labial mucosa
- Appearance: Round/oval, yellow-grey fibrinous base with erythematous halo
- Significance: Major aphthous ulcers in HIV are larger, deeper, more painful, slower to heal than in immunocompetent patients
- Treatment: Topical corticosteroids; thalidomide for refractory major ulcers in HIV; ART
4. Kaposi's Sarcoma (KS) of Oral Cavity
- Organism: Human Herpesvirus-8 (HHV-8)
- CD4 trigger: < 200/μL
- Site: Hard palate most common intraoral site; also gingiva, tongue, buccal mucosa
- Appearance: Flat, red/violaceous (purple), painless macules → progress to raised nodules/plaques → may ulcerate and become painful
- Significance: Oral KS is often the first sign of AIDS; presence of oral KS = advanced disease
- Diagnosis: Biopsy — spindle cells, slit-like vascular spaces, extravasated RBCs
- Treatment: ART alone (early/localised); intralesional vinblastine for local lesions; systemic liposomal doxorubicin for extensive disease
5. HIV-Associated Periodontal Diseases

- Linear Gingival Erythema (LGE):
- Bright red band (2–3 mm) along the free gingival margin; disproportionate to plaque burden
- Does not respond to normal oral hygiene
- Necrotising Ulcerative Gingivitis (NUG):
- Painful, ulceration and necrosis of interdental papillae; fetid odour; bleeding
- Punched-out interdental papillae — classic sign
- Necrotising Ulcerative Periodontitis (NUP):
- Extension of NUG into alveolar bone; rapid bone destruction; tooth loss
- May progress to Necrotising Stomatitis in severe HIV
- Treatment: Metronidazole + chlorhexidine rinse; debridement; ART
6. Herpes Simplex Virus (HSV) Oral Ulcers
- CD4 trigger: < 100/μL
- Appearance: Multiple, painful, shallow ulcers on keratinised (hard palate, gingiva) and non-keratinised mucosa; perioral vesicles/crusting
- Key difference from aphthous: HSV affects keratinised mucosa; aphthous affects non-keratinised mucosa
- Treatment: Acyclovir / Valacyclovir; foscarnet for acyclovir-resistant strains
7. Oral Non-Hodgkin's Lymphoma (NHL)
- Type: High-grade B-cell lymphoma (EBV-associated)
- CD4 trigger: < 100/μL
- Site: Palate, gingiva, tongue, tonsillar area
- Appearance: Rapidly enlarging soft tissue mass; may ulcerate; painless initially
- Diagnosis: Biopsy + immunohistochemistry; CT/PET for staging
- Treatment: CHOP chemotherapy + ART; radiotherapy for localised disease
8. Salivary Gland Disease
- HIV-associated Salivary Gland Disease (HIVSGD):
- Bilateral parotid swelling (parotid most commonly affected)
- Due to lymphoepithelial cysts or diffuse infiltrative lymphocytosis syndrome (DILS)
- Xerostomia (dry mouth) — common; increases caries and candidiasis risk
- Examination: Soft, non-tender bilateral parotid enlargement
- Treatment: ART; pilocarpine for xerostomia
II. OTHER ENT MANIFESTATIONS
9. EAR
- Otitis Externa: Recurrent, often fungal (Aspergillus, Candida); severe and refractory
- Otitis Media: Recurrent ASOM; serous otitis media from Eustachian tube dysfunction
- Sensorineural Hearing Loss: Due to CMV, cryptococcal meningitis, or HIV itself (direct cochlear damage)
- Pneumocystis jirovecii Otitis: Polypoid lesions in EAC — rare but characteristic
10. NOSE AND SINUSES
- Recurrent Rhinosinusitis: Bacterial (Pseudomonas, S. pneumoniae), fungal (invasive aspergillosis, mucormycosis in severe immunosuppression)
- Nasal Kaposi's Sarcoma: Violaceous lesions on nasal mucosa; epistaxis
- Nasal Polyps: Associated with recurrent sinusitis
11. PHARYNX AND LARYNX
- Non-specific Pharyngitis: At seroconversion — resembles infectious mononucleosis
- CMV Pharyngitis/Oesophagitis: Painful shallow ulcers; CD4 < 50/μL
- Laryngeal Candidiasis: Hoarseness; seen with advanced AIDS; odynophagia
- Laryngeal Kaposi's Sarcoma: Hoarseness, stridor, dysphagia; may cause airway compromise
12. NECK / LYMPHADENOPATHY
- Persistent Generalised Lymphadenopathy (PGL):
- Bilateral cervical, submandibular lymph nodes enlarged > 1 cm for > 3 months
- Due to follicular hyperplasia; soft, non-tender, mobile
- CD4 usually still normal at this stage
- Malignant Lymphadenopathy:
- NHL or KS involvement; nodes hard, matted, rapidly growing
- Nasopharyngeal lymphoma — presents with nasal obstruction, epistaxis, neck nodes
Summary Table — High-Yield Oral Lesions
| Lesion | Organism | Site | Cannot Wipe Off | CD4 |
|---|---|---|---|---|
| Oral Candidiasis | Candida | Soft palate, tongue | ✗ (wipes off) | < 300 |
| Oral Hairy Leukoplakia | EBV | Lateral tongue | ✓ | < 300 |
| Kaposi's Sarcoma | HHV-8 | Hard palate | ✓ | < 200 |
| Aphthous Ulcers | Immune dysregulation | Non-keratinised | — | Variable |
| HSV Ulcers | HSV-1/2 | Keratinised mucosa | — | < 100 |
| NHL | EBV/B-cell | Palate, tonsil | — | < 100 |
Key Exam Points
- OHL on lateral tongue that cannot be wiped off = Pathognomonic of HIV — always write this
- Oral candidiasis that wipes off + bleeds = Pseudomembranous type
- Hard palate violaceous lesion = Kaposi's Sarcoma until proven otherwise
- Bilateral parotid swelling in a young adult = Think HIV
- PGL = bilateral cervical lymphadenopathy > 1 cm, > 3 months, with no other cause
- ART is the backbone of treatment for ALL HIV-related ENT manifestations