Audiology tuning fork tests explain mechanisms and tests
Reading File
search_medical_text
tuning fork tests audiology Rinne Weber Schwabach mechanisms
search_medical_text
conductive sensorineural hearing loss tuning fork interpretation
search_medical_image
tuning fork Rinne Weber test diagram audiology
GradeResponse
GradeResponse
GradeResponse
Audiology Tuning Fork Tests
Underlying Mechanisms: Air vs. Bone Conduction
To understand tuning fork tests, the two pathways of sound transmission must be clear:
| Pathway | Route | Structures Involved |
|---|---|---|
| Air Conduction (AC) | Sound waves → EAC → tympanic membrane → ossicles (malleus, incus, stapes) → oval window → cochlea → auditory nerve | Outer + middle + inner ear |
| Bone Conduction (BC) | Vibration of skull → bypasses outer and middle ear → directly stimulates cochlear fluids → auditory nerve | Inner ear only |
Key principle: In a normal ear, AC > BC because the outer and middle ear amplify sound. When the middle or outer ear is damaged (conductive hearing loss), this amplification is lost, so BC becomes relatively better than AC. When the inner ear or auditory nerve is damaged (sensorineural hearing loss), both AC and BC are reduced proportionally, so AC remains > BC.
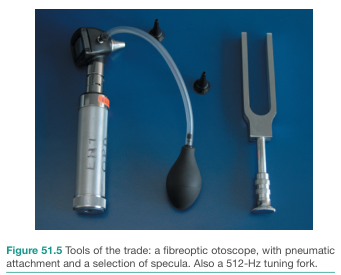
The Standard Tuning Fork: 512 Hz
The 512 Hz fork is the clinical standard (Harrison's, p. 1037):
- Low enough to produce a tone perceptible by bone conduction
- High enough to avoid tactile vibration confounding the result (lower frequencies like 128 Hz can be felt)
- Falls within the critical speech frequency range
The Tests
1. Rinne Test
Purpose: Compares AC vs. BC in the same ear.
Technique:
- Strike the tuning fork and place the vibrating tines near the external auditory canal opening (AC position)
- Then place the stem on the mastoid process (BC position)
- Ask: "Which is louder?" or use the sequential method: hold at mastoid until no longer heard, then move to EAC — ask if sound returns
Interpretation:
| Result | Finding | Meaning |
|---|---|---|
| AC > BC (Rinne Positive) | Normal | Normal hearing OR sensorineural hearing loss |
| BC > AC (Rinne Negative) | Abnormal | Conductive hearing loss ≥30 dB |
| Equal | Borderline | May indicate mild conductive loss |
According to Harrison's (p. 1037): "with conductive hearing loss of ≥30 dB, the bone-conduction stimulus is perceived as louder than the air-conduction stimulus."
False-negative Rinne (important pitfall): In severe unilateral sensorineural hearing loss, the patient may report BC > AC on the affected side — not because of conductive loss, but because bone vibration crosses the skull and is heard by the contralateral normal cochlea. This is the "false negative Rinne." To avoid this, the opposite ear must be masked.
2. Weber Test
Purpose: Detects lateralization of bone-conducted sound; useful when hearing loss is present in one or both ears.
Technique:
- Strike the tuning fork and place the stem on the midline — vertex of the skull, forehead, or upper central incisor teeth
- Ask: "Where do you hear the sound — left, right, or center?"
Interpretation:
| Result | Meaning |
|---|---|
| Midline (no lateralization) | Normal hearing bilaterally OR equal bilateral hearing loss |
| Lateralizes to the WORSE ear | Conductive hearing loss on that side |
| Lateralizes to the BETTER ear | Sensorineural hearing loss on the worse side |
Why does Weber lateralize to the worse ear in conductive loss?
- The occluded/damaged middle ear creates an environment where ambient noise is excluded, reducing "masking" in that ear
- Bone-conducted energy is not dissipated via the normal ossicular pathway, so more energy reaches the cochlea on the conductive-loss side
- This is also why plugging a normal ear with a finger causes the Weber to lateralize to that side (the occlusion effect)
3. Schwabach Test
Purpose: Compares the patient's BC with the examiner's BC (assumes examiner has normal hearing).
Technique:
- Place the vibrating fork stem on the patient's mastoid
- When the patient signals they no longer hear it, immediately transfer to the examiner's mastoid
Interpretation:
| Result | Meaning |
|---|---|
| Examiner still hears it ("Schwabach shortened") | Patient has sensorineural hearing loss (reduced cochlear reserve) |
| Patient hears it longer ("Schwabach prolonged") | Patient has conductive hearing loss (less ambient noise masking) |
| Equal duration | Normal hearing |
Limitation: Heavily dependent on the examiner having genuinely normal hearing; not standardized.
4. Bing Test (Occlusion Test)
Purpose: Tests for the occlusion effect; distinguishes conductive from sensorineural loss.
Technique:
- Place the fork stem on the mastoid
- Alternately occlude and release the external auditory canal with a fingertip
- Ask if the sound gets louder when the ear is blocked
Interpretation:
| Result | Meaning |
|---|---|
| Sound gets louder with occlusion (Bing positive) | Normal or sensorineural hearing loss |
| No change with occlusion (Bing negative) | Conductive hearing loss (occlusion effect already lost) |
5. Gelle Test
Purpose: Tests ossicular mobility, specifically for otosclerosis.
Technique: A pneumatic otoscope increases pressure in the EAC while a tuning fork is applied to the mastoid; if the ossicular chain is mobile, increased pressure damps it and the sound softens.
| Result | Meaning |
|---|---|
| Sound diminishes with pressure (Gelle positive) | Normal ossicular mobility |
| No change (Gelle negative) | Fixed ossicular chain (e.g., otosclerosis) |
Combined Interpretation Summary
| Rinne (Affected Ear) | Weber | Diagnosis |
|---|---|---|
| Positive (AC > BC) | Midline | Normal |
| Positive (AC > BC) | Lateralizes to better ear | Sensorineural loss (worse ear) |
| Negative (BC > AC) | Lateralizes to worse ear | Conductive loss (worse ear) |
| Bilateral negative | Midline or bilateral | Bilateral conductive loss |
| Positive (AC > BC) — but false negative possible | Lateralizes to better ear | Severe unilateral SNHL (mask contralateral ear) |
Clinical Pearls
- Always use a 512 Hz fork — 256 Hz causes too much tactile sensation, 1024 Hz is too quiet for BC
- Strike the fork against the knee or palm, not a hard surface (avoids overtones)
- The Rinne only detects conductive loss when the air-bone gap is ≥30 dB — smaller gaps may not be picked up
- Tuning fork tests are screening tools, not replacements for formal pure-tone audiometry
- In a noisy clinical environment, results may be unreliable; audiometry in a sound-treated booth is the gold standard
Primary source: Harrison's Principles of Internal Medicine, 21st Edition, p. 1037
Can u also include audiology and evaluation of audio gram
search_medical_text
audiogram pure tone audiometry interpretation air bone conduction thresholds
search_medical_text
audiologic assessment speech audiometry tympanometry acoustic reflex
search_medical_image
audiogram patterns conductive sensorineural hearing loss
GradeResponse
GradeResponse
GradeResponse
search_medical_text
tympanometry acoustic reflex decay retrocochlear cochlear hearing loss evaluation
search_medical_text
speech reception threshold word recognition score audiometry hearing loss severity classification
search_medical_image
tympanogram types A B C audiogram sensorineural presbycusis noise induced
GradeResponse
Here is the expanded section on audiologic evaluation and audiogram interpretation, building directly on the tuning fork content above.
Audiologic Evaluation & Audiogram Interpretation
The Minimum Audiologic Test Battery
According to Harrison's (p. 1037), the minimum assessment for any hearing loss complaint must include:
- Pure tone air-conduction thresholds
- Pure tone bone-conduction thresholds
- Speech reception threshold (SRT)
- Word recognition score (WRS)
- Tympanometry
- Acoustic reflexes
- Acoustic reflex decay
This battery screens the entire auditory system and determines whether further differentiation of cochlear (sensory) vs. retrocochlear (neural) pathology is needed.
1. Pure Tone Audiometry
How It Works
The patient wears headphones (AC) or a bone oscillator placed on the mastoid (BC). Pure tones of varying frequencies and intensities are presented; the patient signals when heard. The threshold — the lowest intensity perceived 50% of the time — is plotted on the audiogram.
The Audiogram Grid
| Axis | Values |
|---|---|
| X-axis (frequency) | 250 Hz → 8000 Hz (octave steps); speech range is 500–4000 Hz |
| Y-axis (intensity) | 0 dB HL (normal threshold) → 120 dB HL (profound loss); lower on page = worse |
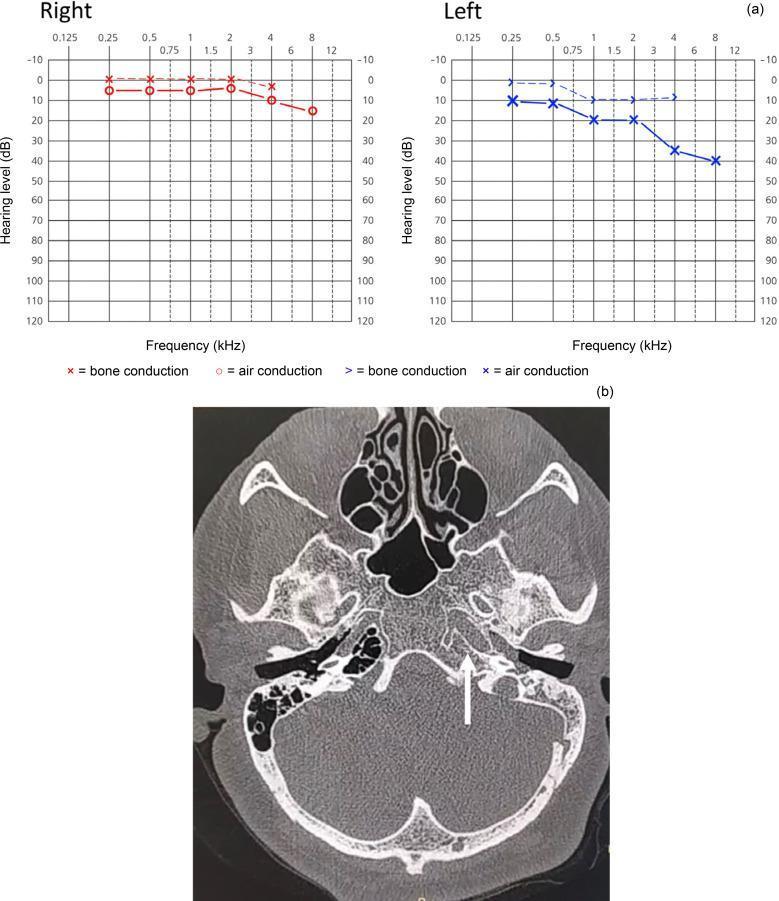
Standard Audiogram Symbols
| Symbol | Meaning |
|---|---|
| O (red) | Right ear, air conduction |
| X (blue) | Left ear, air conduction |
| < or [ (red) | Right ear, bone conduction |
| > or ] (blue) | Left ear, bone conduction |
| Arrows ↓ | No response at maximum output |
Air-Bone Gap (ABG)
The difference between AC and BC thresholds at any frequency:
- ABG = 0 → No conductive component
- ABG ≥ 10–15 dB → Significant conductive component
- Maximum possible ABG is ~60 dB (the limit of the conductive mechanism)
2. Severity Classification of Hearing Loss
| Threshold (dB HL) | Severity |
|---|---|
| 0–25 | Normal |
| 26–40 | Mild |
| 41–55 | Moderate |
| 56–70 | Moderately severe |
| 71–90 | Severe |
| >90 | Profound |
3. Audiogram Patterns by Type of Loss
A. Normal Audiogram
- All thresholds ≤25 dB HL
- AC and BC overlap (no ABG)
- Flat across all frequencies
B. Conductive Hearing Loss
- BC normal (≤25 dB HL across frequencies) — cochlea and nerve intact
- AC elevated — outer/middle ear pathway blocked
- ABG present at affected frequencies
- Pattern depends on pathology:
- Mass-dominant (middle ear effusion): thresholds elevated predominantly at high frequencies
- Stiffness-dominant (early otosclerosis): elevations at low frequencies
- Mixed stiffness + mass: flat elevation across all frequencies
(Harrison's, p. 1038)
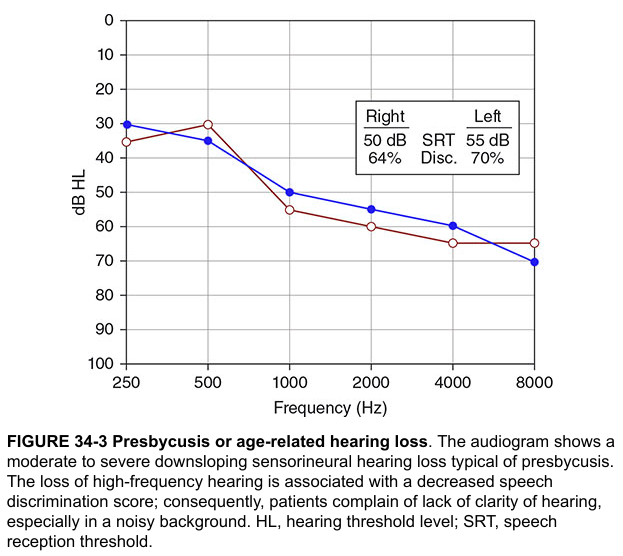
C. Sensorineural Hearing Loss (SNHL)
- BC and AC both elevated in parallel — no ABG
- Cochlea or auditory nerve is damaged
- Common patterns:
| Pattern | Pathology |
|---|---|
| High-frequency downsloping | Presbycusis (age-related), noise-induced |
| Notch at 4000 Hz | Noise-induced hearing loss (4 kHz notch, recovers at 8 kHz) |
| Low-frequency SNHL | Ménière's disease (early stages) |
| Flat SNHL | Sudden SNHL, autoimmune |
| Cookie-bite (mid-frequency dip) | Hereditary/genetic SNHL |
(Harrison's, p. 1038)
D. Presbycusis Audiogram
E. Mixed Hearing Loss
- Both AC and BC are elevated (SNHL component)
- ABG is still present (conductive component on top)
- Example: Chronic otitis media with superimposed presbycusis
F. Conductive Loss with Air-Bone Gap (Clinical Example)
4. Speech Audiometry
A. Speech Reception Threshold (SRT)
- The lowest intensity at which the patient correctly repeats 50% of spondee words (two-syllable words with equal stress, e.g., "baseball," "hotdog")
- Should agree with the pure tone average (PTA) of 500, 1000, and 2000 Hz within ±10 dB
- Discrepancy between SRT and PTA suggests non-organic hearing loss (functional/malingering)
B. Word Recognition Score (WRS) / Speech Discrimination Score
- Monosyllabic words presented at a suprathreshold level (usually SRT + 30–40 dB)
- Expressed as percentage correct (0–100%)
- Distinguishes cochlear from retrocochlear pathology:
| WRS | Interpretation |
|---|---|
| 90–100% | Normal or mild conductive loss |
| 75–90% | Mild difficulty; mild SNHL |
| 50–75% | Moderate difficulty; moderate SNHL |
| <50% | Poor discrimination; suspect retrocochlear pathology |
| Rollover (score drops at higher intensities) | Retrocochlear (acoustic neuroma) — pathognomonic |
5. Tympanometry (Immittance Audiometry)
Measures middle ear compliance (how easily the TM and ossicles move) by varying air pressure in the sealed EAC.
Tympanogram Types (Jerger Classification)
| Type | Shape | Peak | Compliance | Interpretation |
|---|---|---|---|---|
| Type A | Normal peaked curve | At 0 daPa | Normal (0.3–1.6 mL) | Normal middle ear |
| Type As ("shallow") | Low-amplitude peak | At 0 daPa | Reduced | Otosclerosis, ossicular fixation |
| Type Ad ("deep/discontinuous") | Exaggerated peak | At 0 daPa | Increased | Ossicular discontinuity, thin/flaccid TM |
| Type B | Flat, no peak | — | Very low | Middle ear effusion, TM perforation, PE tube |
| Type C | Peaked but shifted | Negative pressure (< −100 daPa) | Normal/low | Eustachian tube dysfunction |
6. Acoustic Reflexes
The stapedius muscle contracts bilaterally in response to loud sound (≥70–85 dB above threshold), stiffening the ossicular chain. This is the acoustic (stapedius) reflex.
Reflex Testing
| Measurement | What it tests |
|---|---|
| Ipsilateral reflex | Same ear stimulus + detection |
| Contralateral reflex | Stimulus one ear, detection other |
| Reflex threshold | Lowest intensity eliciting reflex |
| Reflex decay | Sustained tone — reflex should hold for ≥10 sec |
Interpretation
| Finding | Significance |
|---|---|
| Absent reflex with conductive loss | Expected — stiffened middle ear |
| Absent reflex with normal tympanogram | Suggests facial nerve (CN VII) pathology or severe SNHL |
| Reflex decay (reflex fades in <5 sec at 500 or 1000 Hz) | Retrocochlear pathology — acoustic neuroma, CN VIII lesion |
| Elevated reflex threshold | Cochlear hearing loss |
7. Distinguishing Cochlear vs. Retrocochlear on Audiometry
This is a critical diagnostic step:
| Feature | Cochlear (Sensory) | Retrocochlear (Neural) |
|---|---|---|
| WRS | Proportional to pure tone loss | Disproportionately poor |
| Rollover | Absent | Present |
| Acoustic reflex decay | Normal | Abnormal (fades <5 sec) |
| ABR (auditory brainstem response) | Normal latencies | Prolonged wave V latency or absent waves |
| Imaging | Normal | MRI may show vestibular schwannoma |
8. Integration: Tuning Fork Tests + Audiogram
| Rinne | Weber | Audiogram | Tympanogram | Likely Diagnosis |
|---|---|---|---|---|
| Positive bilateral | Midline | Normal | Type A | Normal hearing |
| Negative unilateral | Lateralizes to that ear | AC elevated, BC normal, ABG present | Type B or C | Conductive loss (effusion/otosclerosis) |
| Positive bilateral | Lateralizes to better ear | AC+BC elevated, no ABG, high freq | Type A | SNHL (presbycusis/noise) |
| Positive (false neg) | To better ear | Severe unilateral SNHL | Type A | Severe SNHL — mask contralateral |
| Negative unilateral | Midline | AC+BC elevated + ABG | Type A | Mixed hearing loss |
Key Clinical Pearls
- Pure tone audiometry defines the presence, type, and severity of loss; tuning fork tests are screening tools that must be confirmed by formal audiometry
- The SRT–PTA agreement rule (within ±10 dB) is an important validity check; larger discrepancies raise suspicion for functional hearing loss
- Rollover on WRS and acoustic reflex decay are the two most important screening signs of retrocochlear pathology — prompt MRI internal auditory canals with gadolinium if either is present
- The 4 kHz notch on audiogram is pathognomonic for noise-induced hearing loss; unlike presbycusis, it recovers slightly at 8 kHz
- Ménière's disease is the classic exception among SNHLs — it affects low frequencies first, opposite to most other SNHL causes
Sources: Harrison's Principles of Internal Medicine, 21st Edition, pp. 1037–1038; Bailey & Love's Short Practice of Surgery, 28th Edition, p. 774
This is a shared conversation. Sign in to Orris to start your own chat.