syntehtic cannabinoids
Reading File
Finding Sources
Searching PubMed
synthetic cannabinoids pharmacology toxicity
Searching the Web
synthetic cannabinoids pharmacology mechanism toxicity clinical effects 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Here is a full, synthesized overview:
Synthetic Cannabinoids
What Are They?
Synthetic cannabinoids (SCs) are laboratory-synthesized chemicals designed to bind cannabinoid receptors (CB1 and CB2). Unlike THC, which is a partial agonist, most SCs are full, high-efficacy CB1 agonists - making them far more potent and unpredictable than natural cannabis. They are sold as "herbal incense," "Spice," "K2," or "fake marijuana," labeled "not for human consumption" to circumvent drug laws.
- Rosen's Emergency Medicine, p. 2974
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 2772
Chemical Structure
SCs are structurally diverse and generally bear little resemblance to THC, which is why standard urine drug screens miss them (only HU-210, a structural THC analogue, triggers a positive THC immunoassay).
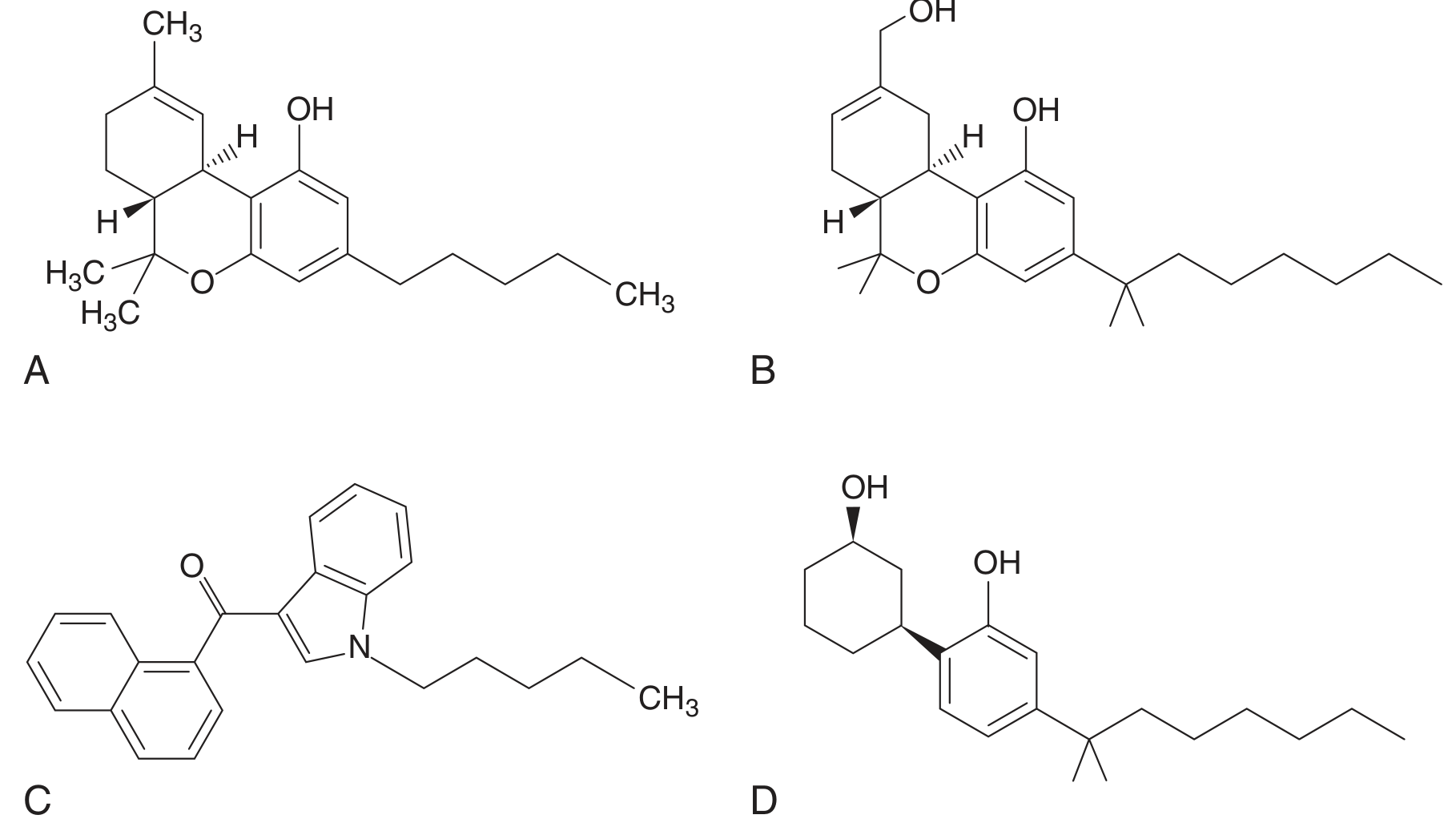
Cannabinoid structures: (A) Δ9-THC, (B) HU-210, (C) JWH-018, (D) CP-47,497 - Rosen's Emergency Medicine
Major Structural Classes
| Class | Examples |
|---|---|
| Naphthoylindoles | JWH-018, JWH-073, JWH-200 |
| Cyclohexylphenols | CP-47,497, cannabicyclohexanol |
| THC analogues | HU-210 |
| Indazole carboxamides | AB-FUBINACA, ADB-PINACA |
| Quinolone carboxylates | PB-22, 5F-PB-22 |
Pharmacology
Mechanism of Action
- CB1R (CNS) and CB2R (peripheral immune cells) are the primary targets
- SCs act as full agonists at CB1R - compared to THC's partial agonism, this produces far greater receptor activation, higher intrinsic efficacy, and more severe psychological/physiological effects
- Their "off-target" receptor activities are largely uncharacterized; they may engage serotonin, dopamine, opioid, or other receptors unpredictably - Goodman & Gilman's, p. 2772
- Because they are produced in illicit labs with minimal quality control, products may also contain contaminants (synthetic opioids, vitamin K antagonists, caffeine)
The Endocannabinoid System (Briefly)
SCs hijack the endocannabinoid system (ECS), which normally uses lipid signaling molecules (anandamide/AEA, 2-arachidonoylglycerol/2-AG) synthesized "on demand" to modulate neurotransmission. The ECS regulates stress, pain, reward, metabolism, and inflammation. Full agonism at CB1R by SCs overwhelms this modulatory system.
Potency
Synthetic cannabinoids are 2 to 100 times more potent than THC - CDC MMWR data documented a range of severe neuropsychiatric, cardiovascular, and renal effects at doses far lower than comparable cannabis.
Routes of Administration & Onset
SCs are dissolved in solvent and sprayed onto dried plant material, then typically smoked in paper (similar to marijuana). They can also be vaporized or taken as liquids.
- Onset: Within minutes of inhalation
- Duration: Generally 2-4 hours (first-generation); may be prolonged with newer agents
- Peak blood levels occur within ~8 minutes of inhalation
Generations and Clinical Features
First-Generation (JWH-018, JWH-073, HU-210, CP-47,497)
- Tachycardia
- Agitation and anxiety
- Nausea/vomiting
- Altered mentation, hallucinations
- Seizures
Second-Generation (ADB-PINACA, AB-FUBINACA)
More severe profile per Rosen's Emergency Medicine, p. 2975:
- Profound agitation and aggression followed by CNS depression
- Seizures
- Tachycardia followed by bradycardia
- Hypertension followed by hypotension
- Ischemic stroke (uncommon)
- Cardiac toxicity
General Adverse Effects Summary
| System | Effects |
|---|---|
| CNS | Agitation, anxiety, hallucinations, psychosis, seizures, coma |
| Cardiovascular | Tachycardia (most common), bradycardia, hypertension/hypotension, arrhythmias, ischemic stroke |
| Renal | Acute kidney injury |
| GI | Nausea, vomiting, cannabinoid hyperemesis syndrome |
| Psychiatric | Precipitation of psychosis (especially in predisposed individuals), paranoia |
| Hematologic | Coagulopathy (brodifacoum contamination - see below) |
Brodifacoum Contamination Outbreak
A notable hazard: in 2018, an outbreak in Illinois (160+ cases, 4 deaths) was traced to SC products contaminated with brodifacoum, a long-acting vitamin K antagonist rodenticide. Patients presented with unexplained multi-site bleeding and bruising requiring prolonged vitamin K supplementation. This illustrates the unpredictable danger of illicit SC products - Rosen's Emergency Medicine, p. 2975.
Diagnosis
- Standard urine drug screens are negative for most SCs (only HU-210 cross-reacts with THC immunoassay)
- Specific SC testing requires mass spectrometry (GC-MS or LC-MS/MS) and is not routinely available at point of care
- Diagnosis is largely clinical, based on history of use and presentation
- Differential includes: acute psychosis, opioid or sedative overdose (in children), and co-ingestion with ethanol or other drugs
Management
Treatment is supportive - there is no specific antidote:
| Symptom | Treatment |
|---|---|
| Agitation, anxiety, tachycardia | Benzodiazepines (titrated to effect) |
| Severe psychosis | Antipsychotics if necessary |
| Nausea/vomiting | Ondansetron 4-8 mg IV, metoclopramide 10-20 mg IV, or butyrophenones (haloperidol/droperidol 0.625-2.5 mg IV) |
| Cannabinoid hyperemesis | Hot showers, topical capsaicin (TRPV1 mechanism) |
| Brodifacoum coagulopathy | Vitamin K supplementation (long-term) |
| Bradycardia/hypotension | Supportive hemodynamic management |
Most patients can be discharged once awake with normal vital signs. Severe or persistent symptoms warrant hospital admission - Tintinalli's Emergency Medicine, p. 1288.
Legal Status & Regulation
- 2012 Synthetic Drug Abuse Prevention Act placed 26 SC types permanently into Schedule I (US)
- DEA emergency-scheduled JWH-018, JWH-073, JWH-200, CP-47,497, cannabicyclohexanol (2011), then AB-FUBINACA, ADB-PINACA, PB-22, 5F-PB-22 (2014)
- Manufacturers circumvent scheduling by rapidly substituting unscheduled analogues - effective regulation remains challenging
- A 2025 NYC Health Department advisory noted a renewed surge in SC-related ED visits, with arrhythmias, agitation, and unresponsiveness as dominant presentations
Withdrawal
Regular SC users can develop withdrawal syndrome, whose symptoms significantly overlap with overdose symptoms, complicating clinical assessment - NYC DOH Advisory, 2025.
Recent Evidence
A 2024 systematic review (PMID 39273431) on new psychoactive substance toxicity confirmed acute and chronic psychiatric effects including psychosis, anxiety disorders, and cognitive impairment. A 2025 review on neurological aspects of drug misuse (PMID 40425276) highlighted SC-associated ischemic stroke as an increasingly recognized complication. A 2025 systematic review (PubMed 40334326) of 49 studies confirmed SC use is linked to more severe cardiovascular and neurological complications than natural cannabis.
This is a shared conversation. Sign in to Orris to start your own chat.