Megaloblastic anemia for MBBS final year exams 10 mark question
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed for a comprehensive 10-mark answer. Let me compose it.
Megaloblastic Anemia - MBBS Final Year 10-Mark Answer
Definition
Megaloblastic anemia is an anemia (often with pancytopenia) resulting from impaired DNA synthesis in hematopoietic precursor cells, leading to a characteristic imbalance between nuclear and cytoplasmic maturation (nuclear-cytoplasmic asynchrony). The cells grow large but fail to divide normally, producing "megaloblasts."
- Goldman-Cecil Medicine, p. 1728
Causes / Etiology
Vitamin B12 (Cobalamin) Deficiency
| Category | Examples |
|---|---|
| Lack of Intrinsic Factor | Pernicious anemia (autoimmune), gastrectomy, gastric bypass |
| Ileal malabsorption | Ileal resection, Crohn disease, Imerslund-Grasbeck syndrome |
| Competitive usurption | Fish tapeworm (Diphyllobothrium latum), bacterial overgrowth, blind loops |
| Nutritional | Strict veganism / lacto-vegetarian diet |
| Drugs | Metformin, proton pump inhibitors, nitrous oxide |
Folate Deficiency
| Category | Examples |
|---|---|
| Decreased intake | Alcoholism, poor diet (no green leafy vegetables) |
| Impaired absorption | Celiac disease, tropical sprue, Crohn disease |
| Increased demand | Pregnancy, hemolytic anemias, disseminated cancer |
| Drugs blocking folate | Methotrexate, trimethoprim, phenytoin, carbamazepine, sulfasalazine |
| Increased loss | Hemodialysis |
Other (not responsive to B12 or folate)
-
Drugs inhibiting DNA synthesis: cytosine arabinoside, hydroxyurea
-
Inborn errors of folate/cobalamin metabolism
-
Robbins Pathology, p. 608
Biochemical Mechanisms (Pathogenesis)
Vitamin B12 and folate are both required for DNA synthesis via a shared metabolic pathway.

Fig. 14.18 - Robbins Pathology: In B12 deficiency, folate is trapped as N5-Methyl FH4 ("folate trap"), preventing thymidylate synthesis and DNA replication.
Two key enzymatic reactions require B12:
-
Methionine synthase reaction: Methylcobalamin converts homocysteine → methionine, and simultaneously converts N⁵-methyl-THF → THF (tetrahydrofolate). In B12 deficiency, folate is "trapped" as N⁵-methyl-THF ("folate trap hypothesis"), making it unavailable for thymidylate synthesis.
-
Methylmalonyl-CoA mutase reaction: Adenosylcobalamin converts methylmalonyl-CoA → succinyl-CoA. Deficiency leads to elevated methylmalonic acid - the most sensitive/specific marker of B12 deficiency. Accumulation of abnormal fatty acids in neuronal membranes causes subacute combined degeneration of the spinal cord.
Key point: Folate deficiency causes anemia alone. B12 deficiency causes anemia plus neurological disease (subacute combined degeneration). Giving folate to a B12-deficient patient corrects anemia but worsens (or unmasks) neuropathy.
- Robbins Pathology, pp. 609-610
Morphology / Histopathology
Peripheral Blood Smear
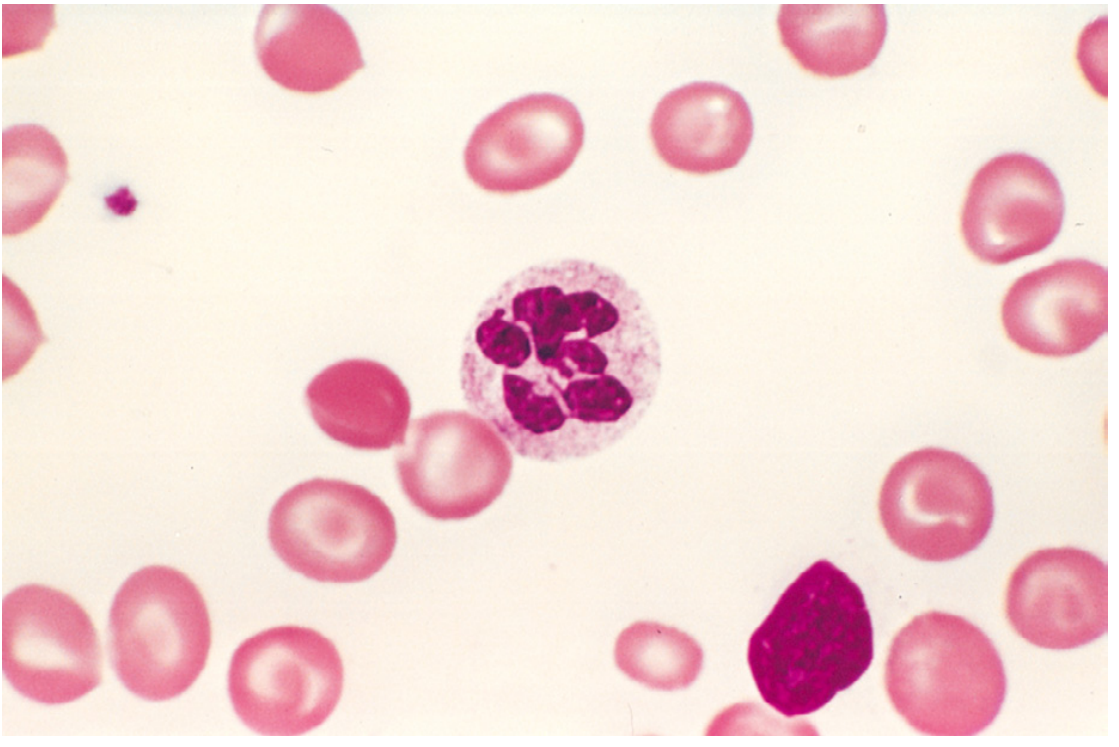
Fig. 14.15 - Robbins Pathology: Hypersegmented neutrophil (6 lobes) in megaloblastic anemia. Also note macro-ovalocytes.
- Macro-ovalocytes (macrocytic oval RBCs - most characteristic finding)
- MCV typically >100 fL (can be >120 fL)
- No central pallor (appear hyperchromic, but MCHC is NOT elevated)
- Marked anisocytosis and poikilocytosis
- Hypersegmented neutrophils (5+ lobes; a single neutrophil with 6+ lobes is diagnostic)
- Low reticulocyte count
- Thrombocytopenia (in severe disease - pancytopenia)
Bone Marrow Aspirate
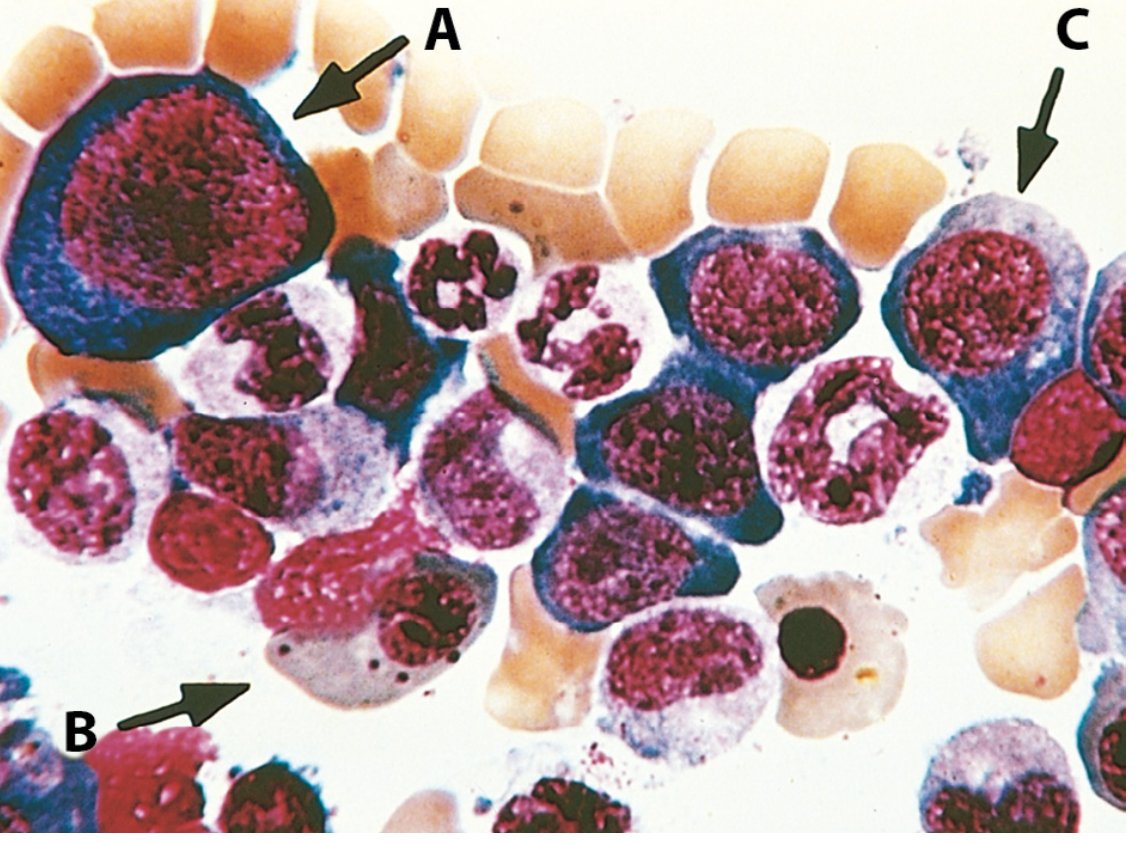
Fig. 14.16 - Robbins Pathology: Megaloblasts in various stages. Note the orthochromatic megaloblast (B) is hemoglobinized (pink cytoplasm) but retains an open, finely distributed nucleus instead of being pyknotic - hallmark of nuclear-cytoplasmic asynchrony.
-
Hypercellular marrow (response to erythropoietin)
-
Megaloblasts - large erythroid precursors with finely distributed ("open") chromatin despite cytoplasmic maturation
-
Nuclear-cytoplasmic asynchrony (cytoplasm matures normally, nucleus lags)
-
Giant metamyelocytes and band forms in granulocytic series
-
Abnormally large megakaryocytes with multilobate nuclei
-
Ineffective hematopoiesis - most precursors undergo apoptosis in marrow
-
Robbins Pathology, pp. 608-609
Pernicious Anemia (Special Form of B12 Deficiency)
Pernicious anemia is an autoimmune gastritis leading to loss of gastric parietal cells and absent intrinsic factor (IF) production.
Three types of autoantibodies:
| Antibody | Prevalence | Mechanism |
|---|---|---|
| Type I (anti-IF blocking Ab) | 75% | Blocks B12 binding to IF |
| Type II (binding/precipitating Ab) | ~50% | Blocks IF-B12 complex from binding cubilin receptor in ileum |
| Type III (anti-parietal cell Ab / anti-H+K+ATPase) | 85-90% | Targets gastric proton pump; marker but not primary cause |
Associated conditions: autoimmune thyroiditis, vitiligo, adrenalitis (Addison disease), other autoimmune disorders.
Gastric morphology: Fundic gland atrophy, loss of parietal and chief cells, intestinal metaplasia ("intestinalization"), atrophic glossitis (beefy red tongue).
Clinical Features
Hematologic
- Gradual onset of anemia: fatigue, pallor, dyspnoea on exertion
- Glossitis - sore, smooth, red tongue
- Mild jaundice (from intramedullary hemolysis / ineffective erythropoiesis)
- Splenomegaly (mild)
Neurological (B12 deficiency ONLY - not folate)
Subacute Combined Degeneration (SCD) of the spinal cord:
- Demyelination of dorsal columns (posterior columns) - loss of vibration sense, proprioception, positive Romberg sign
- Demyelination of lateral corticospinal tracts - upper motor neuron signs, spastic paraparesis
- Peripheral neuropathy, paresthesias ("glove and stocking")
- Cognitive changes, depression, memory loss
Note: Neurological symptoms may precede hematological findings in some patients.
Laboratory Diagnosis
| Investigation | Findings |
|---|---|
| CBC | Macrocytic anemia, MCV >100 fL; often pancytopenia |
| PBS | Macro-ovalocytes, hypersegmented neutrophils |
| Reticulocyte count | Low (hypoproliferative) |
| Bone marrow | Hypercellular, megaloblasts, nuclear-cytoplasmic asynchrony |
| Serum B12 | Low (<200 pg/mL) in B12 deficiency |
| Serum folate / RBC folate | Low in folate deficiency; RBC folate more reliable |
| Serum methylmalonic acid | Elevated in B12 deficiency only (most sensitive/specific) |
| Serum homocysteine | Elevated in both B12 and folate deficiency |
| LDH | Markedly elevated (intramedullary destruction) |
| Indirect bilirubin | Mildly elevated |
| Serum haptoglobin | Decreased |
| Anti-intrinsic factor Ab | Highly specific for pernicious anemia (Type I: 75% sensitivity) |
| Schilling test | Historically used to diagnose pernicious anemia (now rarely done) |
Key diagnostic rule:
-
Elevated methylmalonic acid + elevated homocysteine → B12 deficiency
-
Elevated homocysteine only (normal methylmalonic acid) → Folate deficiency
-
Goldman-Cecil Medicine, p. 1729
Treatment
Vitamin B12 Deficiency (Pernicious Anemia / severe)
- IM cyanocobalamin or hydroxycobalamin: 1000 µg daily for 7 days, then weekly for 8 weeks, then monthly for life
- High-dose oral B12 (1000-2000 µg/day): Effective via passive absorption even without IF; used in dietary deficiency
- Hydroxycobalamin retained longer than cyanocobalamin (can give every 2-3 months after loading)
Folate Deficiency
- Oral folic acid 1-5 mg/day for 4 months (or until deficiency corrected)
- IMPORTANT: Before giving folate, always rule out B12 deficiency to prevent precipitating/worsening neurological disease
Response to Treatment
- Reticulocyte crisis (peak) at 5-7 days after treatment initiation
- Hematological improvement within 2 months
- Neurological improvement may take months; severe neurological damage may be irreversible
Key Differences: B12 vs Folate Deficiency
| Feature | Vitamin B12 Deficiency | Folate Deficiency |
|---|---|---|
| Cause | Dietary (vegan), pernicious anemia, ileal disease | Alcoholism, poor diet, drugs, pregnancy |
| Stores | 3-5 years | 3-4 months |
| Neurological | Subacute combined degeneration | Absent |
| Methylmalonic acid | Elevated | Normal |
| Homocysteine | Elevated | Elevated |
| Neural tube defects (prevention) | Not applicable | Folate supplementation prevents NTDs |
| Treatment | B12 injections/high-dose oral | Oral folic acid |
Summary Points for Exam
- Megaloblastic anemia = impaired DNA synthesis → nuclear-cytoplasmic asynchrony → ineffective erythropoiesis
- Most common causes: B12 deficiency (especially pernicious anemia) and folate deficiency
- Key CBC finding: MCV >100 fL; key PBS finding: macro-ovalocytes + hypersegmented neutrophils
- Bone marrow is hypercellular with megaloblasts - ineffective erythropoiesis causes paradox of hypercellular marrow with pancytopenia
- B12 deficiency UNIQUELY causes subacute combined degeneration (posterior + lateral cord)
- Methylmalonic acid is elevated ONLY in B12 deficiency - best differentiator
- "Folate trap": In B12 deficiency, folate cannot be regenerated as THF → same end result as folate deficiency (anemia), but with added neurological disease
- Pernicious anemia: autoimmune - anti-IF antibodies diagnostic; treat with lifelong B12
- Giving folate to B12-deficient patient corrects anemia but worsens neuropathy - dangerous error
- Reticulocyte peak at day 5-7 confirms diagnosis and response to treatment
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 608-611; Goldman-Cecil Medicine, Chapter 150, pp. 1728-1731
This is a shared conversation. Sign in to Orris to start your own chat.