Please tell me everything about fatty liver in pathology chapter cell injury from the book Robbins mbbs second year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
I now have all the information needed from both Robbins books. Let me compile a comprehensive answer.
Fatty Liver (Steatosis / Fatty Change) - Cell Injury Chapter, Robbins
Context Within Cell Injury
Fatty change is one of the two most consistent morphologic correlates of reversible cell injury (the other being cellular swelling). It is discussed under the heading of Intracellular and Extracellular Depositions / Intracellular Accumulations within the Cell Injury chapter.
- Robbins & Kumar Basic Pathology, p. 36 - "Fatty change is manifested by the appearance of lipid vacuoles in the cytoplasm. It is principally encountered in organs that are involved in lipid metabolism, such as the liver."
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 73
Definition
Steatosis and fatty change are synonymous terms that describe abnormal accumulations of triglycerides within parenchymal cells.
"The terms steatosis and fatty change describe abnormal accumulations of triglycerides within parenchymal cells."
- Robbins, Cotran & Kumar, Ch. 2
Organs Affected
The liver is the primary organ involved because it is the major organ of fat metabolism. However, fatty change also occurs in:
- Heart
- Skeletal muscle
- Kidney
- Other organs
Mechanism: Why Does Fatty Liver Occur?
This is classified as Mechanism 1 among the four mechanisms of intracellular accumulation: inadequate removal of a normal substance due to defects in production and transport (as illustrated in Fig. 2.29 below).
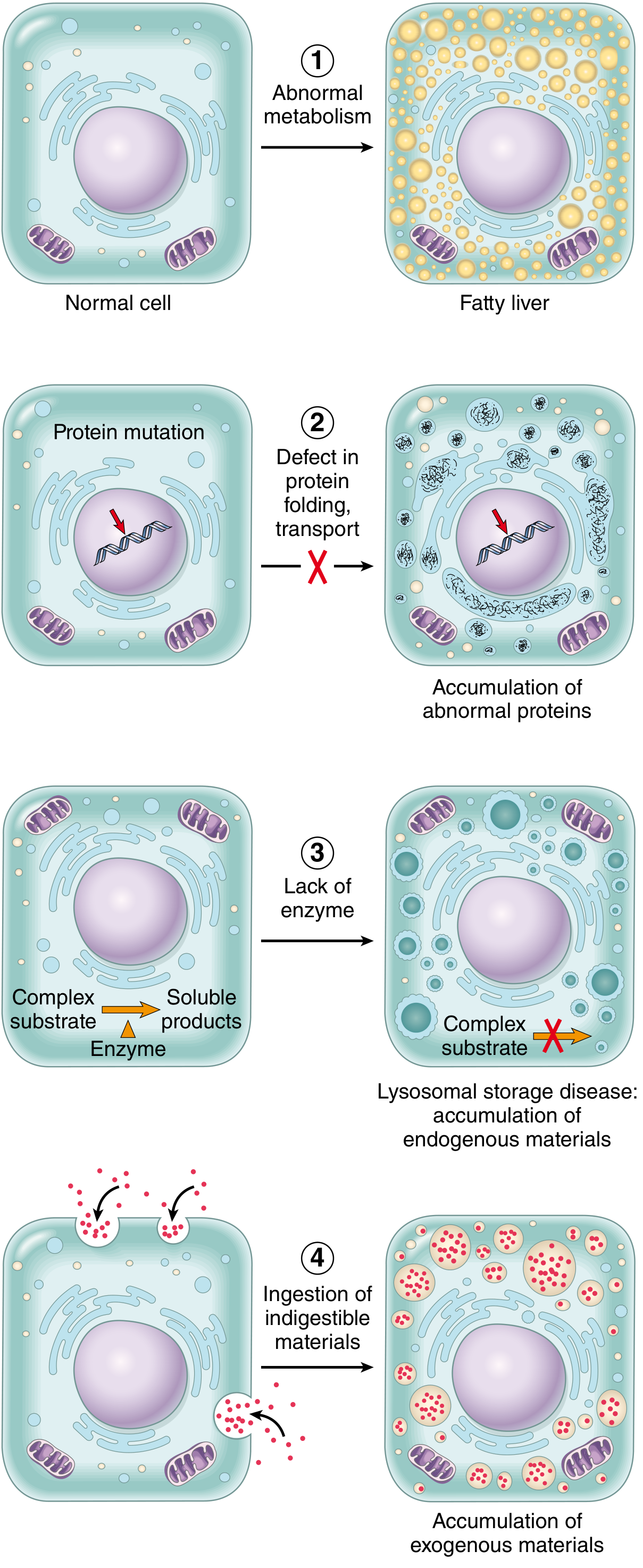
Fig. 2.29 Mechanisms of intracellular accumulations. Fatty liver is Mechanism 1 - abnormal metabolism leading to triglyceride accumulation in hepatocytes.
The liver normally handles fat by:
- Taking up free fatty acids (FFAs) from the blood
- Esterifying them into triglycerides
- Packaging triglycerides into lipoproteins (VLDL)
- Secreting VLDL into the blood for transport to peripheral tissues
Fatty accumulation occurs when any of these steps are disrupted:
- Increased delivery of FFAs to the liver (e.g., obesity, starvation, diabetes)
- Decreased oxidation of FFAs (e.g., hypoxia, toxins that impair mitochondria)
- Decreased synthesis of transport proteins (apolipoproteins) - e.g., protein malnutrition, alcohol, carbon tetrachloride (CCl4) toxicity
- Impaired lipoprotein secretion from the liver
- Increased triglyceride synthesis from FFAs (alcohol stimulates this)
Causes (Etiology)
| Category | Examples |
|---|---|
| Toxins | Alcohol (most common in higher-income countries), CCl4, phosphorus |
| Metabolic disorders | Diabetes mellitus, obesity |
| Nutritional | Protein malnutrition, starvation |
| Hypoxia/ischemia | Anoxia, congestive heart failure |
| Other | Nonalcoholic fatty liver disease (NAFLD), associated with metabolic syndrome |
"In higher-income nations, the most common causes of significant fatty change in the liver (fatty liver) are excessive alcohol use and nonalcoholic fatty liver disease, which is often associated with diabetes and obesity."
- Robbins, Cotran & Kumar, Ch. 2
Morphology (Gross and Microscopic)
Gross Appearance
- The liver is enlarged, soft, yellow, and greasy
- In severe cases, the entire liver may appear bright yellow due to massive lipid deposition
Microscopic Appearance (Histology)
On H&E staining:
- Lipid vacuoles appear as clear, empty-looking spaces within hepatocyte cytoplasm (lipid is dissolved out during routine tissue processing with organic solvents)
- Two patterns:
- Microvesicular steatosis: many small fat droplets scattered throughout the cytoplasm; nucleus remains central
- Macrovesicular steatosis: one or a few large fat vacuoles that expand the cell and displace the nucleus to the periphery of the cell (signet ring-like appearance)
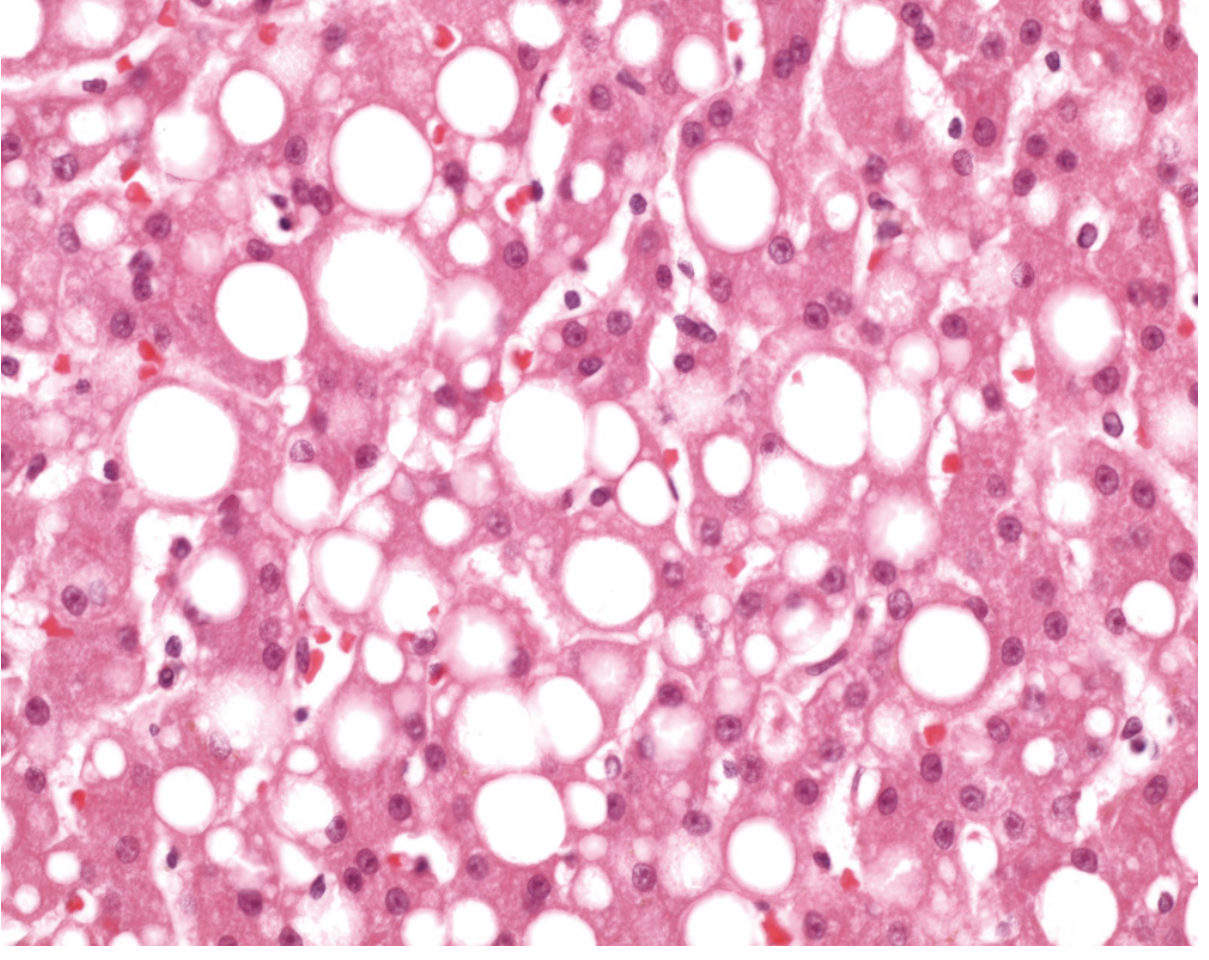
Fig. 2.30 Fatty liver. High-power H&E detail of fatty change of the liver. In most cells, the well-preserved nucleus is squeezed into the displaced rim of cytoplasm about the fat vacuole. (Courtesy Dr. James Crawford, Hofstra Northwell School of Medicine)
"In most cells, the well-preserved nucleus is squeezed into the displaced rim of cytoplasm about the fat vacuole."
- Robbins, Cotran & Kumar, Fig. 2.30 caption
Special stains:
- Oil Red O or Sudan IV stain lipid droplets red/orange and can be used on frozen sections (not formalin-fixed paraffin sections, since lipid is dissolved during processing)
Key Concepts Summary (from Robbins)
| Feature | Details |
|---|---|
| Substance accumulated | Triglycerides (free fatty acids esterified) |
| Mechanism | Inadequate removal/defective transport of normal endogenous substance |
| Reversibility | Reversible - if cause is removed, the liver can return to normal |
| Clinical significance | Usually mild, but severe and persistent fatty change can progress to steatohepatitis, fibrosis, and cirrhosis |
| Most common causes | Alcohol excess, NAFLD/obesity/diabetes |
| Histological pattern | Clear cytoplasmic vacuoles; large vacuoles displace nucleus peripherally |
Relationship to Reversible vs. Irreversible Injury
Fatty change is a hallmark of reversible cell injury - it indicates the cell is metabolically stressed but still viable. If the offending cause is removed (e.g., patient stops drinking alcohol), the accumulated triglycerides can be cleared and the hepatocytes return to normal. This distinguishes it from irreversible injury (necrosis), where the cell has crossed the "point of no return."
Summary Table: Four Mechanisms of Intracellular Accumulation (as in Robbins Fig. 2.29)
| Mechanism | Example |
|---|---|
| 1. Abnormal metabolism / inadequate removal | Fatty liver (steatosis) |
| 2. Defect in protein folding/transport | α1-antitrypsin deficiency |
| 3. Lack of enzyme (lysosomal) | Lysosomal storage diseases |
| 4. Ingestion of indigestible materials | Carbon, silica particle accumulation |
- Robbins & Kumar Basic Pathology (MBBS edition), Chapter 1: Cell Injury, Cell Death, and Adaptations, pp. 36-37
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 2: Cell Injury, Cell Death, and Adaptations, pp. 72-73
This is a shared conversation. Sign in to Orris to start your own chat.