Stem cell. And regenerative medicine.
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching PubMed
"stem cells" AND "regenerative medicine"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Let me compile the full overview.
Stem Cells & Regenerative Medicine - An Overview for Medical Students
1. What Is Regenerative Medicine?
Regenerative medicine is an interdisciplinary field that combines cell biology, biomaterial science, bioengineering, and surgery to restore or replace damaged tissues and organs. Its clinical need is driven by the unrelenting burden of trauma, congenital disorders, ischemia, and degenerative disease - needs that intensify as populations age.
The field's primary incentive is the global organ shortage: organ transplantation is the gold standard for end-organ failure, but demand vastly exceeds supply. If regenerative medicine matures, it may also eliminate the need for lifelong immunosuppression (by using patient-derived cells), reducing long-term healthcare costs considerably. The regenerative medicine market reached ~$9.8 billion in 2021 and is projected to reach ~$37.9 billion by 2030.
- Sabiston Textbook of Surgery, p. 1026
2. Stem Cell Biology - Core Concepts
What Makes a Cell a "Stem Cell"?
Stem cells are defined by two fundamental properties:
- Self-renewal - the ability to divide and produce identical daughter cells indefinitely
- Potency - the ability to differentiate into one or more specialized cell types
Classification by Potency
| Term | Definition | Example |
|---|---|---|
| Totipotent | Can form any cell type including extraembryonic tissue | Fertilized zygote |
| Pluripotent | Can form all three germ layers (but not placenta) | Embryonic stem cells (ESCs), iPSCs |
| Multipotent | Restricted to a tissue lineage | Hematopoietic stem cells |
| Unipotent | Can only produce one cell type | Epidermal basal cells |
3. Types of Stem Cells
A. Embryonic Stem Cells (ESCs)
-
Derived from the inner cell mass of a fertilized blastocyst
-
Self-renewing and pluripotent - can differentiate into any of the three germ layers (endoderm, mesoderm, ectoderm)
-
Highly attractive for regenerative medicine, but carry two major problems:
- Teratoma formation in vivo
- Ethical controversy over use of human embryos
- Immunologic rejection (express HLA antigens foreign to the recipient)
-
Sabiston Textbook of Surgery, p. 1026; Robbins & Cotran Pathologic Basis of Disease, p. 44
B. Adult (Somatic) Stem Cells
- Tissue-resident stem cells found in many organs (bone marrow, gut, skin, liver, brain)
- Generally multipotent, restricted to their tissue of origin
- Key examples:
- Hematopoietic stem cells (HSCs) - the basis of bone marrow/stem cell transplantation
- Mesenchymal stromal cells (MSCs) - derived from bone marrow stroma; can differentiate into bone, cartilage, fat
- Tissue-specific progenitors in gut epithelium, skin basal layer, neural tissue
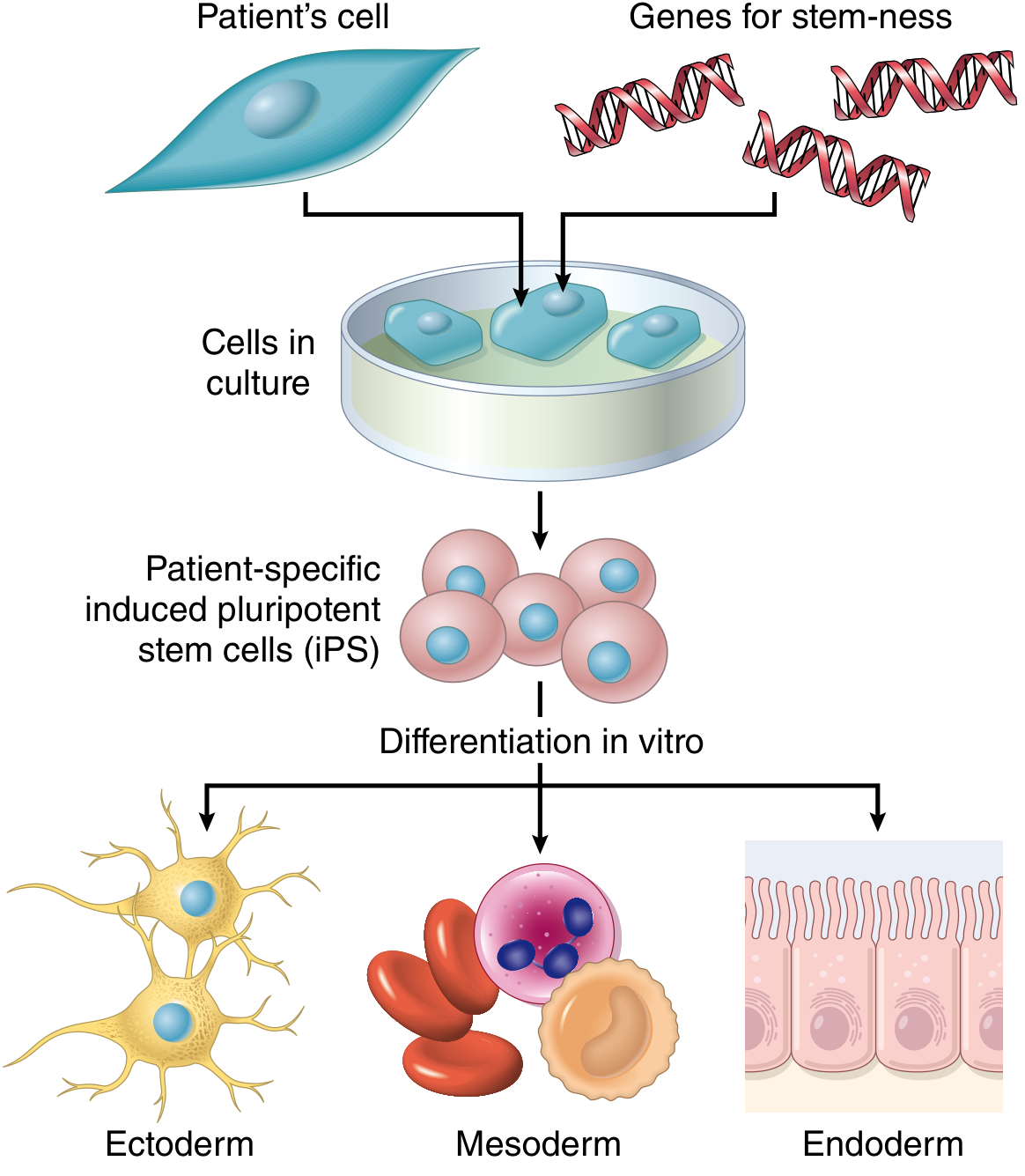
C. Induced Pluripotent Stem Cells (iPSCs) - The Game-Changer
Discovered in 2006 (mice) and 2007 (humans) by Yamanaka and Takahashi (Nobel Prize 2012). A handful of transcription factors (Oct-3/4, Sox2, Klf4, c-Myc - the "Yamanaka factors") are introduced into adult somatic cells (e.g. fibroblasts), reprogramming them back to a pluripotent, embryonic-like state.
Why iPSCs matter clinically:
- Patient-derived - avoids immunologic rejection
- No ethical controversy (no embryo destruction)
- Can be differentiated into virtually any tissue
- Used as disease avatars - patient-derived iPSCs can model genetic diseases in vitro and screen for therapeutics (e.g., generating insulin-secreting β-cells for a diabetic patient)
- Robbins & Cotran Pathologic Basis of Disease, p. 43-44
- Sabiston Textbook of Surgery, p. 1026
4. Cell Therapy Approaches in Regenerative Medicine
Historical Milestones (Established Therapies)
-
Blood transfusion and blood product transfusion
-
Solid organ transplantation
-
In vitro fertilization
-
Bone marrow / hematopoietic stem cell transplantation (the oldest and most well-established stem cell therapy)
-
CAR T-cell therapy for hematologic malignancies - now FDA-approved and in routine clinical use
-
Goldman-Cecil Medicine, p. 328
Emerging / Experimental Approaches
1. Bone Marrow-Derived Stem/Progenitor Cells
Initially thought to transdifferentiate into organ-specific cells (heart, nerve, liver). This transdifferentiation likely does not occur significantly in practice. Clinical benefit appears to come from a paracrine effect - engrafted cells secrete growth factors that augment endogenous tissue repair, improve vascularization, and modulate inflammation. Despite numerous trials, no mesenchymal stromal cell therapies are currently FDA-approved in the US (as of the textbook date).
2. Extracellular Vesicles (EVs)
- EVs (exosomes, microparticles, apoptotic bodies) are secreted by cells and carry lipids, proteins, mRNA, and microRNAs
- Many stem cells may exert their regenerative benefit via EV-mediated paracrine signaling
- Potential advantages over direct cell therapy: reduced cost, easier manufacturing, lower immunogenicity
- Can be engineered for targeted drug delivery
3. Tissue-Specific Stem Cell Activation
- Several organs once thought non-regenerative (brain, pancreas, kidney) do have limited intrinsic regenerative capacity
- Research focuses on isolating and expanding these native progenitors, or stimulating endogenous repair in vivo
4. Tissue Engineering & Scaffolds
- Combines cells with biocompatible scaffolds (biopolymers, decellularized extracellular matrices) to construct functional tissues
- Decellularization: donor organs are stripped of all cells, leaving the ECM scaffold; the patient's own cells are then seeded onto this scaffold to create an immunologically compatible organ
- Goldman-Cecil Medicine, p. 330; Sabiston Textbook of Surgery, p. 1030
5. Clinical Applications - What Has Actually Reached Patients
| Application | Status | Notes |
|---|---|---|
| Bone marrow transplant (HSC) | Standard of care | Leukemia, lymphoma, aplastic anemia |
| CAR T-cell therapy | FDA-approved | Hematologic malignancies |
| Skin substitutes (Integra, Epicel, Apligraf, Recell) | FDA-approved | Burns, chronic ulcers |
| Tissue-engineered bladder | Bench-to-bedside (limited) | First permanent implanted bioengineered organ |
| Tissue-engineered trachea, urethra, vagina | Clinical trials / limited use | |
| Mesenchymal stromal cell therapies | No US FDA approval yet | Many trials ongoing |
| iPSC-derived therapies | Preclinical / early trials | Age-related macular degeneration (most advanced) |
- Sabiston Textbook of Surgery, p. 1030-1031
6. Key Challenges
| Challenge | Details |
|---|---|
| Immunologic rejection | Most stem cells express HLA antigens; iPSCs solve this for autologous use |
| Tumorigenesis | ESCs and iPSCs can form teratomas; incomplete differentiation risks tumor formation |
| Functional integration | Introducing replacement cells and getting them to functionally connect within damaged tissue remains difficult |
| Ethical debate | Largely centered on ESC use (embryo destruction) |
| Manufacturing scale-up | Expanding and quality-controlling cells for clinical use is costly and complex |
| Regulatory pathway | Complex FDA/EMA regulatory landscape for cell and gene therapy products |
7. The Bigger Picture
Regenerative medicine sits at the intersection of cell biology, genetics, biomaterials science, and surgery. The field's trajectory is shaped by:
- iPSC technology enabling patient-specific, rejection-free cell therapies
- Genome editing (CRISPR) allowing correction of disease-causing mutations before cell transplantation
- 3D bioprinting and organ-on-a-chip platforms for building complex tissue architectures
- Organoids as models for drug discovery and personalized medicine
The most clinically mature area remains hematopoietic stem cell transplantation and its derivative, CAR T-cell therapy. The next wave - myocardial regeneration, islet cell replacement for T1DM, neural repair after stroke - remains largely in trial stages, with the immunologic and functional integration challenges yet to be fully solved.
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.), Ch. 1
- Goldman-Cecil Medicine (International Ed.), Ch. 34
- Sabiston Textbook of Surgery (21st ed.), Ch. 50
- Recent systematic review literature (PubMed, 2024-2026): 95 active systematic reviews/meta-analyses on regenerative medicine therapies available
This is a shared conversation. Sign in to Orris to start your own chat.