Gross anatomy of liver
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative surgical textbooks. Let me compile the full answer.
Gross Anatomy of the Liver
Overview
The liver is the largest solid organ in the body, weighing approximately 1,500 g in adults. It sits in the right upper quadrant (hypochondrium), beneath the diaphragm, protected by the rib cage. Its surface is reddish-brown in colour and covered by visceral peritoneum (serosa), beneath which lies a fibrous sheath called Glisson's capsule. At the porta hepatis, the capsule extends along portal tracts into the parenchyma, carrying branches of the hepatic artery, portal vein, and bile ducts.
Surfaces
| Surface | Relations |
|---|---|
| Diaphragmatic (superior) | Smooth, dome-shaped, related to diaphragm and separated from pleura/lung |
| Visceral (inferior) | Bears impressions of stomach, duodenum, right kidney, right adrenal, hepatic flexure of colon |
Ligaments and Peritoneal Reflections
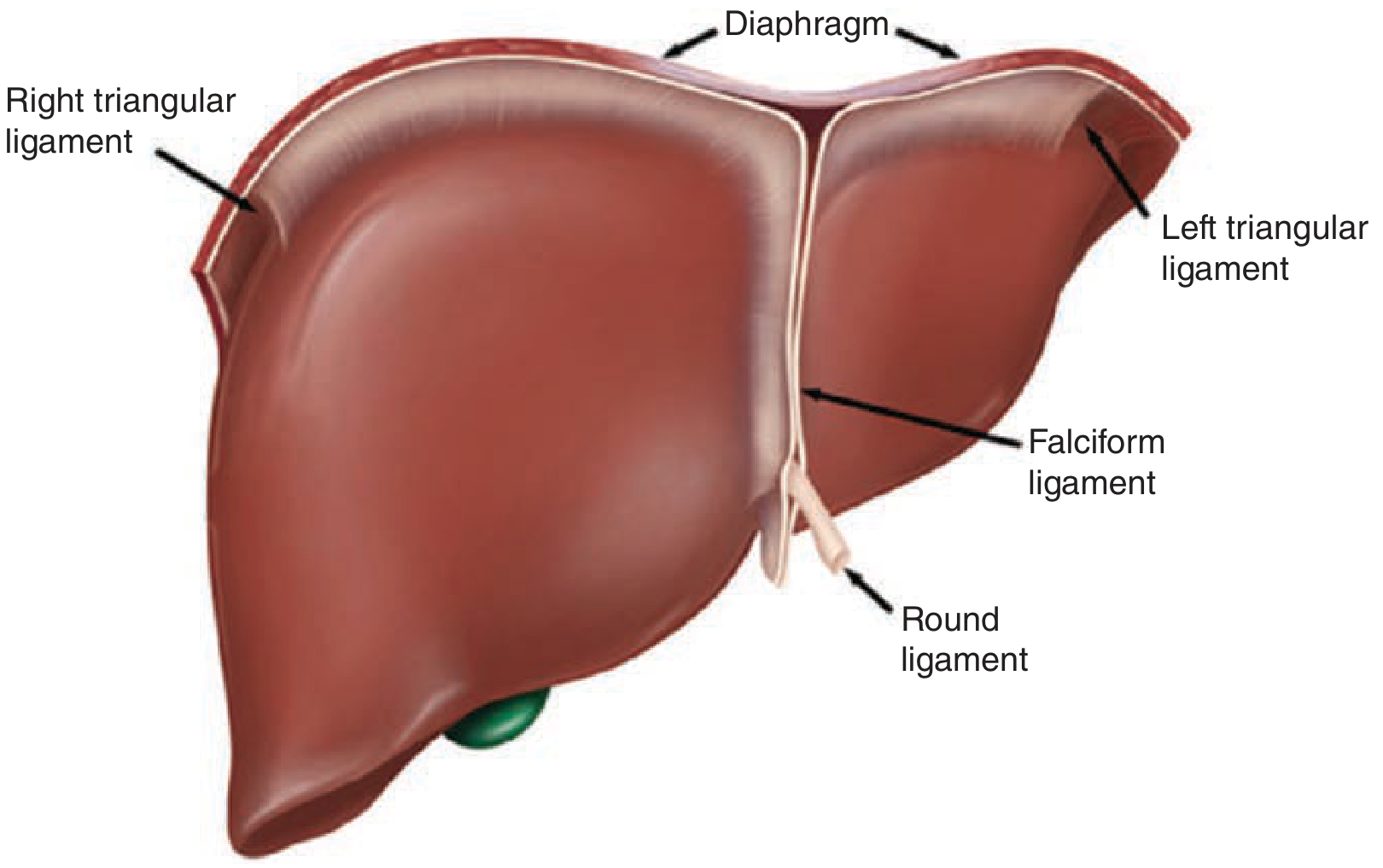
- Falciform ligament - remnant of the umbilical vein; runs from the umbilicus cephalad onto the liver's anterior surface, anchoring it to the anterior abdominal wall. Divides the left lateral from the left medial segment along the umbilical fissure.
- Round ligament (ligamentum teres) - the obliterated umbilical vein, located along the free edge of the falciform ligament; enters the left hepatic hilum.
- Ligamentum venosum (Arantius' ligament) - the obliterated ductus venosus; lies deep between the caudate lobe and left lateral segment.
- Right triangular ligament - anchors the right lobe to the right hemidiaphragm and right retroperitoneum (over the right kidney).
- Left triangular ligament - anchors the left lobe to the left hemidiaphragm.
- Coronary ligaments - extend anteriorly from the triangular ligaments; the right also anchors to the peritoneum over the right kidney.
- Lesser omentum (gastrohepatic and hepatoduodenal ligaments) - connects the liver to the stomach and duodenum; its right free edge is the porta hepatis, containing the common bile duct (right, anterior), hepatic artery proper (left, anterior), and portal vein (posterior).
The foramen of Winslow (epiploic foramen) lies posterior to the porta hepatis and connects the greater and lesser peritoneal sacs. Clamping the hepatoduodenal ligament here controls hepatic inflow - the Pringle maneuver.
Lobes (Traditional Anatomical Division)
Classically, the liver is divided into right and left lobes by the falciform ligament on the anterior surface. Two additional smaller lobes are visible on the visceral surface:
- Caudate lobe (posterior, segment I) - lies anterior to the IVC, to the left, and has three subsegments: Spiegel lobe, paracaval portion, and caudate process.
- Quadrate lobe - between the gallbladder fossa and the falciform ligament anteriorly; corresponds to segment IVB.
Note: The falciform ligament does NOT separate the functional right and left halves. The true surgical (functional) division is Cantlie's line (see below).
Couinaud's Segmental Anatomy
The most important surgical framework is Couinaud's segmental anatomy (1950s), which divides the liver into 8 functionally independent segments based on portal, arterial, and biliary supply:
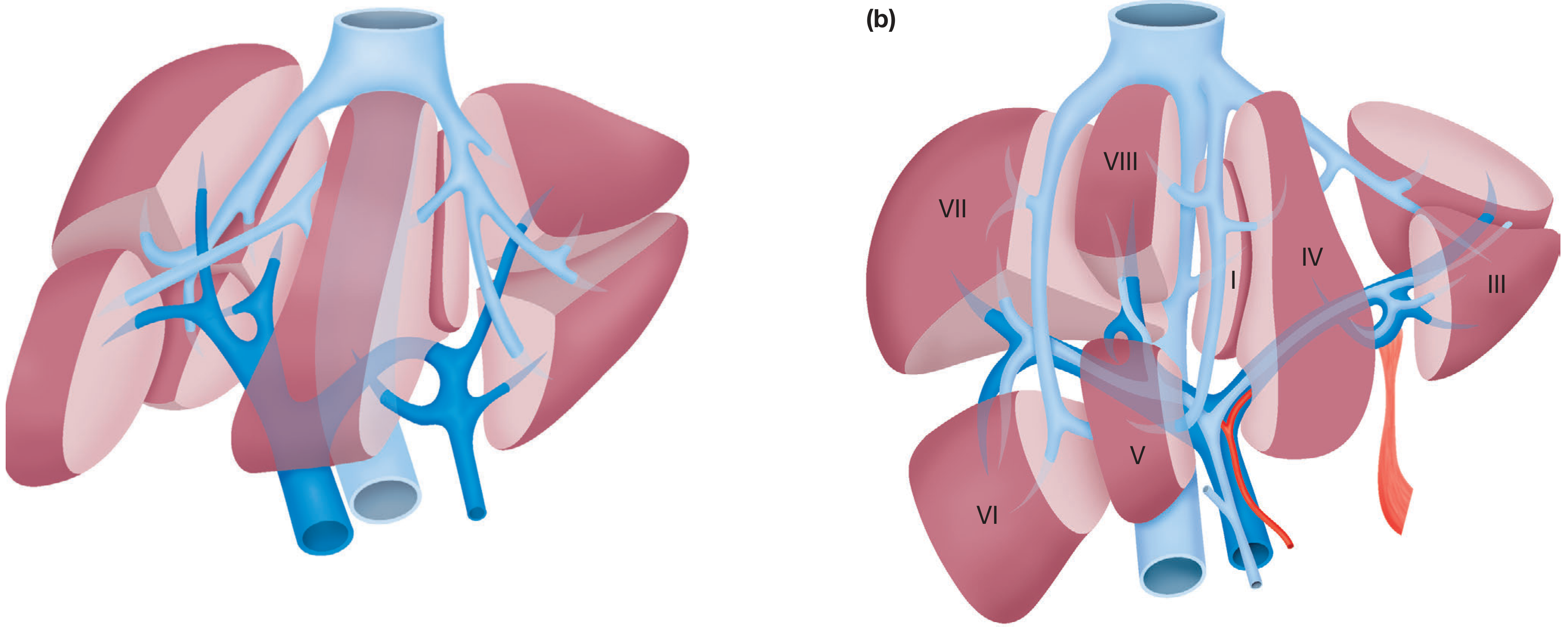
- Segment I - Caudate lobe (posterior, receives supply from both right and left systems)
- Segments II and III - Left lateral section (left lateral segment)
- Segment IV - Left medial segment (IVA = cephalad; IVB = caudad, adjacent to gallbladder)
- Segments V and VIII - Right anterior section
- Segments VI and VII - Right posterior section
Segments are numbered clockwise from the caudate lobe. Each segment is an independent unit with its own portal vein branch, hepatic artery branch, bile duct, and hepatic vein tributary - allowing anatomical resections.
Cantlie's Line (Principal Plane)
An imaginary parasagittal plane from the gallbladder fossa to the IVC. It contains the middle hepatic vein and divides the liver into the right half (segments V-VIII) and left half (segments I-IV) of approximately equal size. This is the true surgical midplane.
Blood Supply
The liver has a dual blood supply:
- Portal vein: ~75-80% of blood flow (nutrient-rich, but less oxygen)
- Hepatic artery: ~20-25% of blood flow (oxygen-rich)
Hepatic Artery
- Arises from the celiac trunk (which also gives left gastric and splenic arteries)
- Celiac trunk → common hepatic artery → gastroduodenal artery + hepatic artery proper
- Hepatic artery proper → right and left hepatic arteries
- "Classic" anatomy is present in only ~76% of individuals
Common arterial variants (24%):
| Variant | Frequency |
|---|---|
| Replaced/accessory right hepatic artery from SMA | 10-15% |
| Replaced/accessory left hepatic artery from left gastric | 3-10% |
| Both replaced right + left hepatic arteries | ~1-2% |
| Completely replaced common hepatic artery from SMA | ~1-2% |
Portal Vein
- Formed by the union of the superior mesenteric vein and splenic vein behind the neck of the pancreas
- Runs in the posterior aspect of the hepatoduodenal ligament
- Divides into right and left portal vein branches at the hilum
- Supplies nutrient-rich blood from the gut, spleen, and pancreas
Venous Drainage (Hepatic Veins)
Three main hepatic veins drain directly into the inferior vena cava (IVC) just below the diaphragm:
| Vein | Fissure | Separates |
|---|---|---|
| Right hepatic vein | Right fissura | Right posterolateral sector (VI, VII) from right anterolateral sector (V, VIII) |
| Middle hepatic vein | Main fissura (Cantlie's line) | Right liver from left liver |
| Left hepatic vein | Left fissura | Left posterior (II) from left anterior sectors (III, IV) |
The caudate lobe (segment I) drains separately via multiple small veins directly into the IVC - making it unique and surgically significant in Budd-Chiari syndrome.
Biliary Drainage
- Bile flows from hepatocytes → bile canaliculi → bile ductules → right and left hepatic ducts
- Right hepatic duct - Right anterior duct (enters above hilar plate) + right posterior duct (dives behind right portal vein)
- Left hepatic duct - Longer extrahepatic course before giving segmental branches
- Right + Left hepatic ducts → Common hepatic duct → (joined by cystic duct) → Common bile duct
- 30-40% of cases have a non-standard hepatic duct confluence (accessory or aberrant ducts)
The gallbladder sits adherent to segments IVB and V.
Porta Hepatis
The porta hepatis (hilum of the liver) is the transverse fissure on the visceral surface through which the following structures enter or exit:
| Structure | Position |
|---|---|
| Common bile duct | Right, anterolateral |
| Hepatic artery proper | Left, anterior |
| Portal vein | Posterior (largest) |
| Lymphatics and autonomic nerves | Accompany the above |
Innervation
- Parasympathetic: Left vagus (anterior hepatic branch) and right vagus (posterior hepatic branch)
- Sympathetic: Greater thoracic splanchnic nerves via the celiac ganglia
- The right phrenic nerve contribution explains referred pain to the right shoulder and scapula in liver/biliary disease
Lymphatic Drainage
- Superficial lymphatics drain to hepatic nodes at the porta hepatis, then to celiac nodes
- Deep lymphatics follow hepatic veins upward to posterior mediastinal nodes, or downward with portal structures to porta hepatis nodes
Embryology (Brief)
- Hepatic diverticulum buds from the foregut at 3-4 weeks' gestation into the ventral wall of the primitive midgut
- Bipotential hepatoblasts invade the septum transversum and differentiate into hepatocytes and cholangiocytes
- The umbilical vein becomes the round ligament (ligamentum teres) after birth
- The ductus venosus becomes the ligamentum venosum
Summary
| Feature | Key Points |
|---|---|
| Weight | ~1,500 g |
| Position | Right hypochondrium, under diaphragm |
| Covering | Glisson's capsule (fibrous); visceral peritoneum |
| Surgical lobes | Right (60-70%): segments V-VIII; Left (+ caudate): segments I-IV |
| Functional division | Cantlie's line (gallbladder fossa to IVC) |
| Segments | 8 (Couinaud), numbered clockwise from caudate |
| Blood supply | Portal vein (75-80%) + hepatic artery (20-25%) |
| Venous drainage | Right, middle, left hepatic veins into IVC |
| Hilum contents | CBD (right), hepatic artery (left), portal vein (posterior) |
| Key ligament | Falciform (ant. abdominal wall), hepatoduodenal (porta hepatis) |
Sources: Schwartz's Principles of Surgery, 11th Ed. | Bailey and Love's Short Practice of Surgery, 28th Ed. | Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.