A 53 year old male presented with Intermediate uvetis(Snow ball Opacitis) Uncontrolled hypertension IC bleed Mantau neg S.ACE nrml Left sided hemi sensory symptoms Improvement with steroids since 2 years
Reading File
Finding Sources
Finding Sources
Searching PubMed
sarcoidosis intermediate uveitis neurosarcoidosis
Reading File
Reading File
Finding Sources
Searching PubMed
neurosarcoidosis stroke intracranial hemorrhage
Reading File
Reading File
Reading Article
PMID: 39812656
Reading Article
PMID: 40835467
Finding Sources
Finding Sources
Searching the Web
neurosarcoidosis normal serum ACE negative Mantoux intracranial hemorrhage hemi-sensory diagnosis 2024
Loading Image
Here is a thorough clinical analysis of this case.
Clinical Diagnosis: Neurosarcoidosis (Probable/Definite)
This presentation is a textbook-level case of neurosarcoidosis masquerading with seronegative findings - one of its most diagnostically challenging forms.
Clinicopathological Correlation
Why Each Feature Points to Neurosarcoidosis
| Feature | Relevance |
|---|---|
| Intermediate uveitis with snowball opacities | Classic ocular sarcoidosis; snowball formation in the context of systemic disease is called intermediate uveitis (not pars planitis, which requires the inflammation to be idiopathic) |
| Intracranial hemorrhage (IC bleed) | Rare but recognized; caused by granulomatous cerebral vasculitis - Focke et al. 2025 systematic review of 29 cases confirmed cerebral vasculitis as a severe NS manifestation |
| Left-sided hemi-sensory symptoms | Right parietal/thalamic granuloma or vasculitic infarct/hemorrhage; focal neurological deficits occur with parenchymal sarcoid granulomas |
| Uncontrolled hypertension | May be secondary to sarcoidosis renal/vascular involvement, or a contributing factor to the IC bleed |
| Mantoux negative | Expected - negative tuberculin test is actually a diagnostic indicator in sarcoidosis, reflecting T-cell anergy; helps exclude TB as a cause |
| Serum ACE normal | Does NOT rule out sarcoidosis - serum ACE has limited sensitivity (~60%) and specificity; it can be normal in up to 40% of sarcoidosis cases and is frequently normal in neurosarcoidosis |
| Improvement with steroids x2 years | Strong supportive evidence - sarcoidosis is steroid-responsive; the granulomatous inflammation and vasculitis both respond to glucocorticoids |
The "Seronegative" Trap
Both a normal serum ACE and a negative Mantoux are frequently misinterpreted as arguing against sarcoidosis. The textbooks are explicit on this:
"Neither the tuberculin skin test, urinary calcium levels, nor the blood concentration of angiotensin-converting enzyme definitively establishes the diagnosis, and each has limited sensitivity and specificity."
- Bradley and Daroff's Neurology in Clinical Practice
Serum ACE is produced by epithelioid cells in granulomas but reflects total granuloma burden - isolated or limited neurosarcoidosis can have a completely normal level. Similarly, the negative Mantoux reflects T-cell anergy in sarcoidosis, not absence of disease - it is sometimes listed as a positive diagnostic indicator for sarcoidosis.
Mechanism of IC Bleed in Neurosarcoidosis
Intracranial hemorrhage in neurosarcoidosis occurs via granulomatous cerebral vasculitis:
- Sarcoid granulomas infiltrate the walls of pial and parenchymal vessels
- This causes transmural inflammation, weakening the vessel wall
- Combined with uncontrolled hypertension, this significantly increases hemorrhagic risk
A 2026 case report (PMID: 40835467) described a patient with recurrent intracerebral hemorrhages and infarctions due to NS where serum ACE was normal, but CSF ACE was elevated and brain biopsy showed "multinucleated giant cell infiltration and epithelial granuloma formation in thickened pial vessel walls." Treatment with IV methylprednisolone stopped recurrence.
The 2025 systematic review (PMID: 39812656) confirmed that motor symptoms and focal neurological deficits are significantly more frequent in NS with vasculitis vs. NS without it.
Histopathology of Neurosarcoidosis
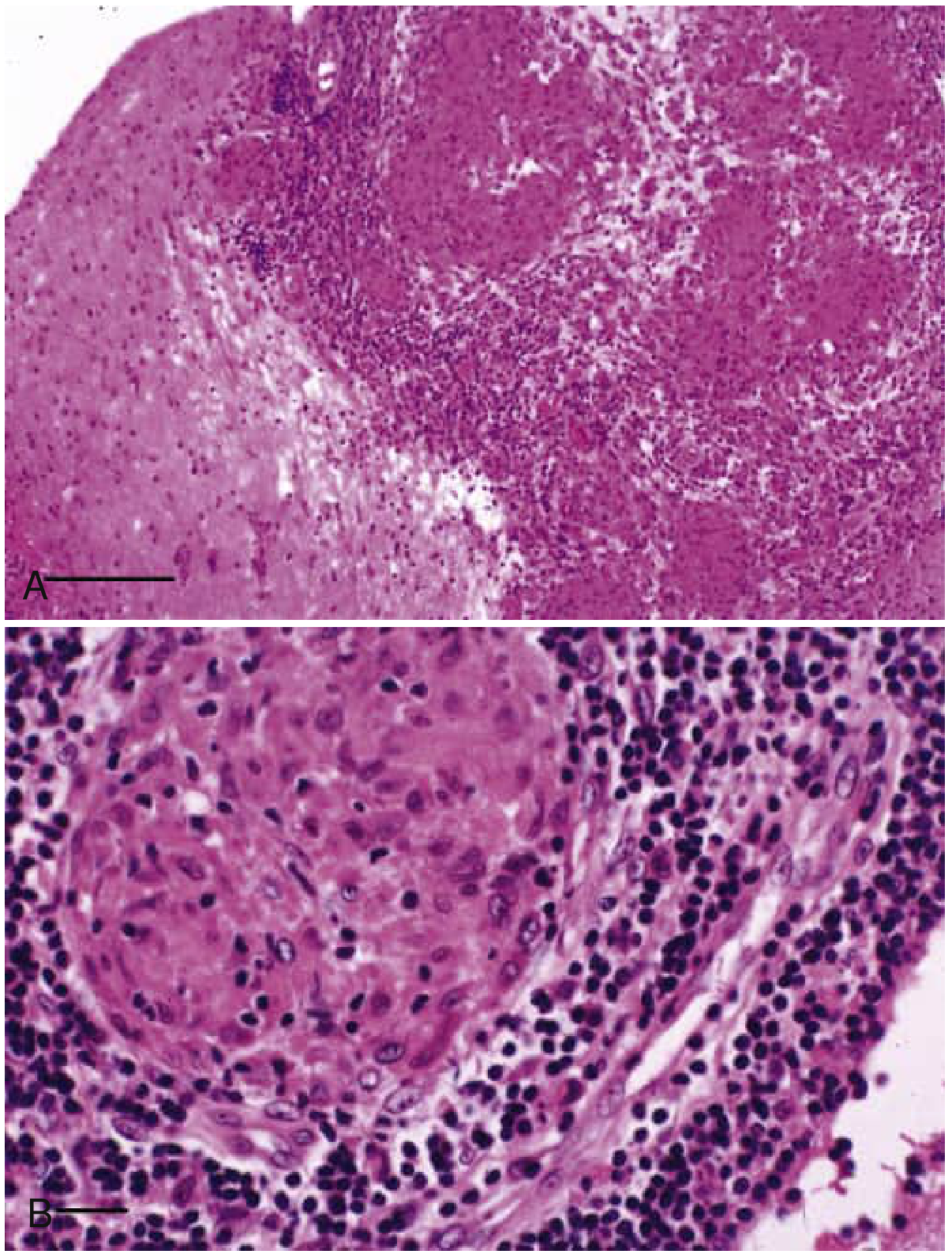
Fig: Brain biopsy in neurosarcoidosis. (A) Dense granulomatous inflammation involving leptomeninges. (B) Virchow-Robin space involvement by epithelioid histiocytes - the hallmark non-caseating granuloma. - Bradley and Daroff's Neurology in Clinical Practice
Diagnostic Workup to Confirm
Since serum ACE and Mantoux are negative/normal, confirm via:
- CSF analysis - elevated protein, lymphocytic pleocytosis; crucially, CSF ACE may be elevated even when serum ACE is normal (as in the 2026 case above); check CSF CD4:CD8 ratio (>5 supports sarcoidosis)
- MRI brain with gadolinium - look for leptomeningeal enhancement, periventricular white matter lesions, cranial nerve enhancement, Virchow-Robin space infiltration
- Whole-body FDG-PET or gallium scan - detects subclinical systemic granulomatous involvement that guides biopsy site
- High-resolution CT chest - hilar lymphadenopathy or pulmonary infiltrates even if CXR is normal
- Serum calcium, 24-hr urinary calcium - hypercalcemia/hypercalciuria supports sarcoidosis
- Conjunctival or accessible tissue biopsy - non-caseating granulomas confirm diagnosis even from clinically unaffected tissue
- MRI vessel wall imaging or DSA - characterize the cerebral vasculitis component
Differential Diagnoses to Exclude
- Multiple sclerosis - intermediate uveitis and left hemi-sensory symptoms can occur; but MS does not cause IC hemorrhage, and steroid response over 2 years fits better with a progressive granulomatous disease than relapsing-remitting MS
- CNS vasculitis (primary PACNS) - no ocular findings, no systemic disease
- CNS lymphoma - check LDH, CSF cytology, no steroid-dependent improvement over 2 years
- Tuberculosis - negative Mantoux and normal ACE not conclusive for TB exclusion either; but TB uveitis with IC bleed is very rare; QuantiFERON-Gold preferred over Mantoux
Management
First-line: Oral prednisolone 1 mg/kg/day, tapered per response - already showing benefit
Blood pressure control is mandatory and urgent given the IC bleed risk from the combined hypertension + vasculitis
Second-line (steroid-refractory/dependent): Methotrexate, mycophenolate mofetil
Third-line (refractory): Infliximab, cyclophosphamide
Surgical: Focal enlarging granulomas may be excised; VP shunt if hydrocephalus develops
Blood pressure control is mandatory and urgent given the IC bleed risk from the combined hypertension + vasculitis
Second-line (steroid-refractory/dependent): Methotrexate, mycophenolate mofetil
Third-line (refractory): Infliximab, cyclophosphamide
Surgical: Focal enlarging granulomas may be excised; VP shunt if hydrocephalus develops
Key Teaching Points
- Normal serum ACE does not exclude neurosarcoidosis - sensitivity is ~60%, and isolated NS often has normal levels; check CSF ACE instead
- Negative Mantoux supports, not refutes, sarcoidosis - it reflects T-cell anergy
- IC hemorrhage in sarcoidosis is rare but real - caused by granulomatous vasculitis; recent literature (2025-2026) highlights this as an under-recognized manifestation
- Intermediate uveitis with snowball opacities in the context of a systemic disease = intermediate uveitis (not pars planitis) - the term "pars planitis" is reserved for idiopathic cases only
- Steroid response over 2 years is a strong clinical anchor for a granulomatous etiology
Sources: Kanski's Clinical Ophthalmology 10th Ed., p.464-465; Bradley and Daroff's Neurology in Clinical Practice; Focke et al., J Neurol 2025 [PMID: 39812656]; Saito et al., Intern Med 2026 [PMID: 40835467]
Does HRCT chest or CSF ACE helps
Finding Sources
Finding Sources
Searching PubMed
neurosarcoidosis CSF ACE diagnosis sensitivity specificity
Reading File
Finding Sources
Searching PubMed
neurosarcoidosis diagnosis biomarkers CSF serum ACE lysozyme
Reading File
Finding Sources
Reading Article
PMID: 42159491
Loading Image
Finding Sources
Here is the direct, evidence-based answer:
HRCT Chest in Neurosarcoidosis - Does It Help?
Short answer: Yes, often - but a negative HRCT does not rule out isolated neurosarcoidosis
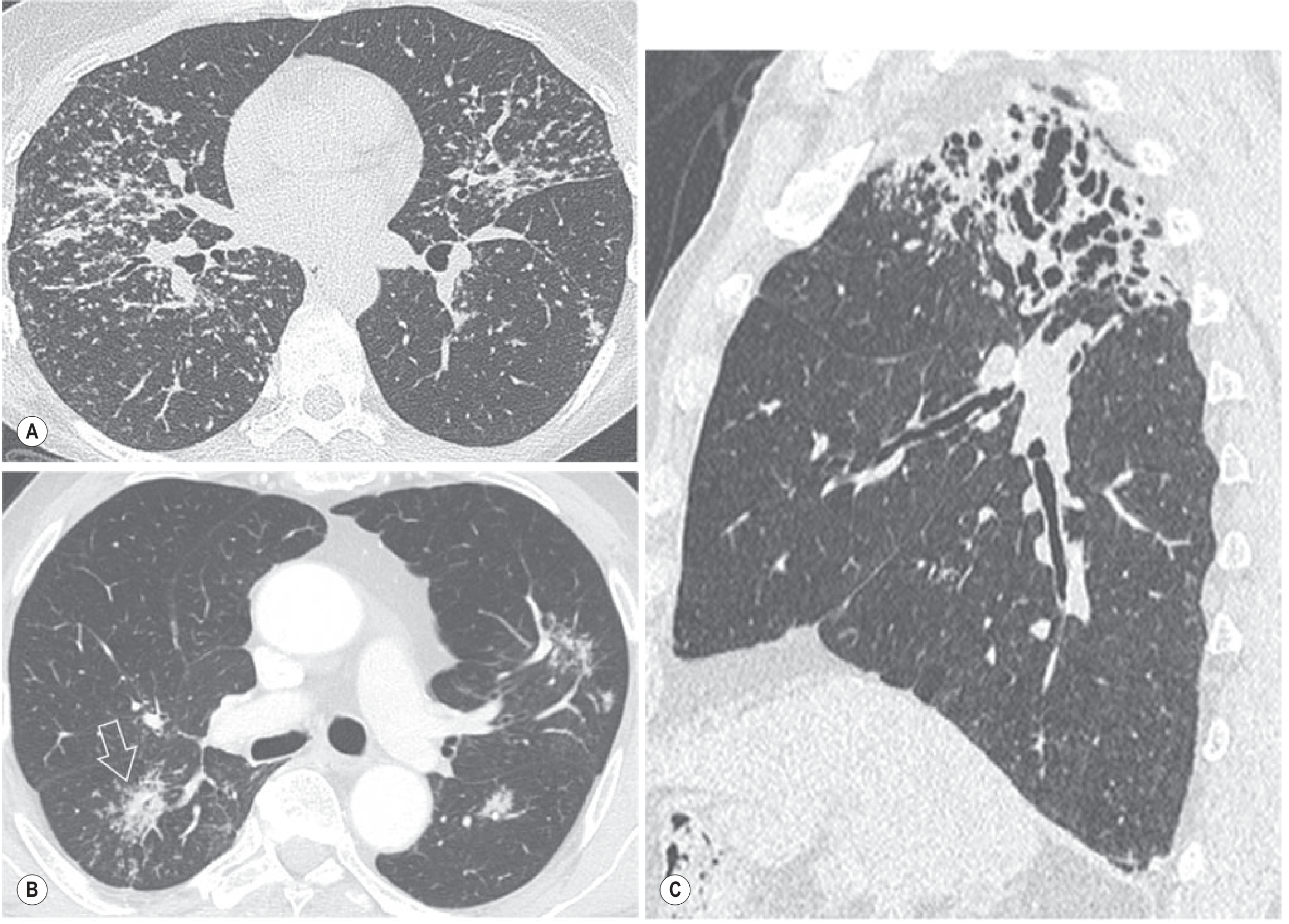
What HRCT can show
HRCT has remarkable sensitivity and specificity for pulmonary sarcoidosis when disease is present. The classical triad to look for:
| HRCT Finding | Significance |
|---|---|
| Bilateral hilar + mediastinal lymphadenopathy | Most common initial finding; highly suggestive |
| Perilymphatic nodules (2-4 mm) along bronchovascular bundles, fissures, septa | Pathognomonic pattern - perilymphatic distribution is sarcoidosis' signature |
| Upper/mid lobe predominance | Distinguishes from hypersensitivity pneumonitis (lower-mid) |
| Galaxy sign (confluent nodules) | Highly specific for sarcoidosis |
| Air trapping | Reflects small airways disease |
The critical caveat for this patient
Isolated neurosarcoidosis (5-10% of NS cases) can have a completely normal HRCT chest. Sarcoid may affect the nervous system before or without any pulmonary involvement. So:
- HRCT positive → confirms systemic sarcoidosis → provides a safe, accessible biopsy site (bronchoscopy + BAL + transbronchial biopsy) → upgrades diagnosis from "possible" to "probable/definite"
- HRCT negative → does NOT exclude sarcoidosis → move to FDG-PET/gallium scan (detects subclinical granulomatous activity in lymph nodes, skin, muscle) and CSF analysis
CSF ACE - Does It Help?
Short answer: Yes - it is more informative than serum ACE in neurosarcoidosis, but still imperfect
Why CSF ACE > serum ACE in NS
| Parameter | Serum ACE | CSF ACE |
|---|---|---|
| Sensitivity in neurosarcoidosis | ~21-40% (very low) | ~55% (moderate) |
| Specificity | ~97% | High |
| Reflects | Total body granuloma burden | Intrathecal granulomatous inflammation |
| Normal in isolated NS? | Frequently | Less commonly |
| Affected by ACE inhibitors | Yes (falsely low) | Yes |
The 2026 study by Daly et al. (PMID: 42159491) measuring serum ACE in sarcoid optic neuropathy (a neuro-ophthalmic form of NS) found sensitivity of only 21.4% with specificity of 97% - confirming that a normal serum ACE in NS means almost nothing clinically.
CSF ACE is more useful because it is produced locally by activated macrophages within CNS granulomas, so it can be elevated even when serum levels are normal. The 2026 hemorrhagic NS case (PMID: 40835467) reported normal serum ACE but elevated CSF ACE - it was the test that clinched the diagnosis before brain biopsy.
Additional CSF findings to look for simultaneously
Do not send CSF for ACE alone. A full CSF panel adds diagnostic weight:
| CSF Parameter | Expected in NS |
|---|---|
| Protein | Elevated (most common finding) |
| Cells | Lymphocytic pleocytosis |
| CSF ACE | Elevated (if NS active in CNS) |
| CSF CD4:CD8 ratio | >5 (supportive) |
| Oligoclonal bands | May be present |
| Glucose | Usually normal (unlike TB/fungal) |
| Cytology | Rules out lymphoma (critical in this age group) |
Practical Algorithm for This Patient
Serum ACE normal + Mantoux negative
↓
Do not stop here
↓
HRCT Chest ──► Positive → Bronchoscopy + BAL + biopsy → Histology
│
└──► Negative → FDG-PET whole body
↓
CSF (protein, cells, ACE, CD4:CD8, cytology)
↓
MRI brain + gadolinium (leptomeningeal enhancement?)
↓
Vessel wall MRI / DSA (characterize vasculitis)
↓
If still negative: conjunctival/accessible tissue biopsy
Bottom line
- HRCT chest: Order it first - if positive, it provides both diagnostic confirmation and the safest biopsy route. A normal result does not exclude disease in this patient.
- CSF ACE: Definitely send it, but as part of a full CSF panel - not in isolation. Its sensitivity is moderate but it captures what serum ACE misses in isolated NS. It is currently the most accessible intrathecal biomarker for NS.
Sources: Grainger & Allison's Diagnostic Radiology; Bradley and Daroff's Neurology in Clinical Practice; Daly et al., J Neuroophthalmol 2026 [PMID: 42159491]; Saito et al., Intern Med 2026 [PMID: 40835467]
Mri brain
Finding Sources
Finding Sources
Searching PubMed
neurosarcoidosis MRI brain findings diagnosis
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.