Medical writting
S
- What is the condition/diagnosis? (e.g., a rare disease, unusual presentation, unexpected outcome)
- Patient details - age, sex, presenting complaint, history, key investigations, treatment, and outcome
- Do you have real case data, or should I draft a template/fictional case for a specific condition?
Psoriasis
plaque psoriasis clinical management
Clinical Case Report: Plaque Psoriasis
Title
Abstract
1. Introduction
2. Case Presentation
2.1 Patient Information
- Age/Sex: 34-year-old male
- Occupation: Office administrator
- Ethnicity: South Asian
- Chief Complaint: Itchy, scaly skin lesions over elbows, knees, and lower back for 3 years
2.2 History of Present Illness
- Psychological stress (workplace)
- Prior use of oral prednisolone for an unrelated condition (prescribed by a general practitioner 6 months ago), after cessation of which lesions acutely worsened
2.3 Past Medical History
- No known chronic illnesses
- No prior hospitalization
- No history of streptococcal throat infection
2.4 Family History
- Father diagnosed with psoriasis
2.5 Medication History
- Topical over-the-counter moisturizers (partial relief)
- Brief course of oral prednisolone (5 mg/day for 2 weeks) - discontinued 6 months ago; followed by flare
2.6 Social History
- Non-smoker; occasional alcohol consumption
- Moderate psychological stress at work
2.7 Review of Systems
- No fever, joint swelling, or ocular redness
- No recent sore throat or upper respiratory tract infection
3. Physical Examination
- Multiple well-demarcated erythematous plaques of varying sizes (2-10 cm), covered with thick, adherent, silvery-white scale
- Distribution: bilateral elbows (extensor surfaces), bilateral knees (extensor surfaces), lumbosacral region
- Auspitz sign: Positive (pinpoint bleeding upon removal of scale)
- Koebner phenomenon: Present (new lesion along a scratch line on the forearm)
- Scalp: scaling plaques along the posterior hairline
- Nails: two fingernails showing pitting; no onycholysis
4. Investigations
| Investigation | Result |
|---|---|
| Complete Blood Count (CBC) | Within normal limits |
| Liver Function Tests (LFT) | Normal |
| Renal Function Tests (RFT) | Normal |
| Fasting Blood Glucose | Normal |
| Lipid Profile | Normal |
| Anti-streptolysin O (ASO) titre | Negative |
| HIV screening | Negative |
| KOH preparation (from lesion scraping) | No fungal hyphae seen |
| Skin Biopsy (punch biopsy, elbow lesion) | Parakeratosis, acanthosis, elongated rete ridges, Munro microabscesses (neutrophils in stratum corneum), dilated tortuous dermal capillaries - consistent with psoriasis |
5. Diagnosis
5.1 Differential Diagnosis Considered
| Condition | Distinguishing Feature |
|---|---|
| Seborrhoeic dermatitis | Greasy scale in seborrheic areas; no Auspitz sign |
| Tinea corporis | Annular border, KOH positive for hyphae |
| Eczema/Atopic dermatitis | Flexural distribution, lichenification; no silvery scale |
| Secondary syphilis | Generalized rash including palms/soles, positive serology |
| Pityriasis rosea | Herald patch, self-limiting course |
| Lichen planus | Violaceous flat-topped papules with Wickham striae |
6. Management
6.1 Patient Education
- Nature of psoriasis explained as a chronic relapsing disease - not contagious
- Avoidance of triggers: stress management, avoidance of skin trauma, smoking cessation counseling
- Counseled explicitly against oral or systemic corticosteroids - systemic steroids are contraindicated as they can precipitate life-threatening generalized pustular psoriasis upon withdrawal
6.2 Topical Therapy (First-line)
-
Clobetasol propionate 0.05% ointment (ultra-high potency corticosteroid) applied once daily to plaques on trunk and extremities for 4 weeks, then tapered. Meta-analysis data shows 68-89% of patients achieve clear or near-clear improvement with clobetasol.
-
Calcipotriene (vitamin D analog) ointment 0.005% applied once daily to same plaques on alternate days with clobetasol (combination approach). Combination topical steroids + calcipotriene provides increased efficacy with fewer side effects compared to either agent alone.
-
Scalp: Clobetasol propionate 0.05% solution applied to scalp plaques nightly.
-
Emollients/Moisturizers: Applied liberally twice daily to all affected areas to reduce scaling and pruritus.
6.3 Systemic Therapy (Consideration for Non-responders)
- Methotrexate 7.5-15 mg weekly oral dose - effective for widespread disease not responding to topical therapy; requires baseline LFT, CBC, hepatitis screening
- Acitretin (systemic retinoid) - for widespread or palmar-plantar psoriasis resistant to topical treatment
- Narrowband UVB (NB-UVB) phototherapy - highly effective; can accelerate clearance in fewer sessions
6.4 Biologic Therapy (for Moderate-Severe/Refractory Disease)
- Etanercept (anti-TNF, subcutaneous) - especially valuable in psoriatic arthritis
- Adalimumab (anti-TNF, subcutaneous) - effective for moderate-severe psoriasis
- Ustekinumab (anti-IL-12/23, subcutaneous) - significantly reduces signs and symptoms
7. Follow-up and Outcome
8. Discussion
9. Conclusion
References
- Fitzpatrick's Dermatology in General Medicine, 9th Edition. McGraw-Hill.
- Textbook of Family Medicine, 9th Edition (Rakel). Elsevier.
- Afifi T, et al. Topical therapies for psoriasis: evidence-based review. Am J Clin Dermatol. 2005.
- Nast A, et al. Topical corticosteroid therapy for psoriasis. J Dtsch Dermatol Ges. 2007.
- Gottlieb AB, et al. Ustekinumab for psoriatic arthritis. N Engl J Med. 2009.
- Choon SE, et al. Asia-Pacific consensus on management of generalized pustular psoriasis. J Dermatol. 2024 Dec. (PMID: 39390737)
Note: This is a fictional illustrative case created for educational and medical writing purposes. Patient details are entirely fictitious. Dosages and treatment protocols should be verified against current local guidelines before clinical application.
Create an infographic showing the stepwise psoriasis treatment algorithm
A clean, professional medical infographic titled "Psoriasis Treatment Algorithm" showing a stepwise vertical flowchart with 4 steps/levels: STEP 1 - MILD DISEASE (BSA less than 10%, PASI less than 10): Blue box at top. Contents: Topical Corticosteroids (e.g. Clobetasol 0.05%), Vitamin D Analogues (Calcipotriene), Combination Topical Therapy, Emollients & Moisturizers, Salicylic Acid (keratolytic). Arrow pointing down labeled "Inadequate Response at 8-12 weeks" STEP 2 - MODERATE DISEASE (BSA 10-30%, PASI 10-20): Green box. Contents: Narrowband UVB Phototherapy (NB-UVB), PUVA Phototherapy, Continue optimized topical therapy. Arrow pointing down labeled "Inadequate Response" STEP 3 - MODERATE-SEVERE DISEASE: Orange box. Contents: Methotrexate (7.5-25mg/week oral), Cyclosporine (short-term), Acitretin (systemic retinoid), Apremilast (PDE4 inhibitor). Arrow pointing down labeled "Inadequate Response or Contraindications" STEP 4 - SEVERE / REFRACTORY DISEASE: Red box. Contents: Biologic Therapy - Anti-TNF: Adalimumab, Etanercept, Infliximab; Anti-IL-17: Secukinumab, Ixekizumab; Anti-IL-23: Ustekinumab, Risankizumab Side panel with red warning box: "AVOID systemic corticosteroids - risk of rebound pustular psoriasis" Bottom section: Assessment Tools: PASI Score, BSA%, DLQI (Quality of Life). Color coded severity bar on the left side from green (mild) to red (severe). Clean white background, modern medical style, icons for pills, injection syringes, UV light. Title at top in dark navy blue bold text.
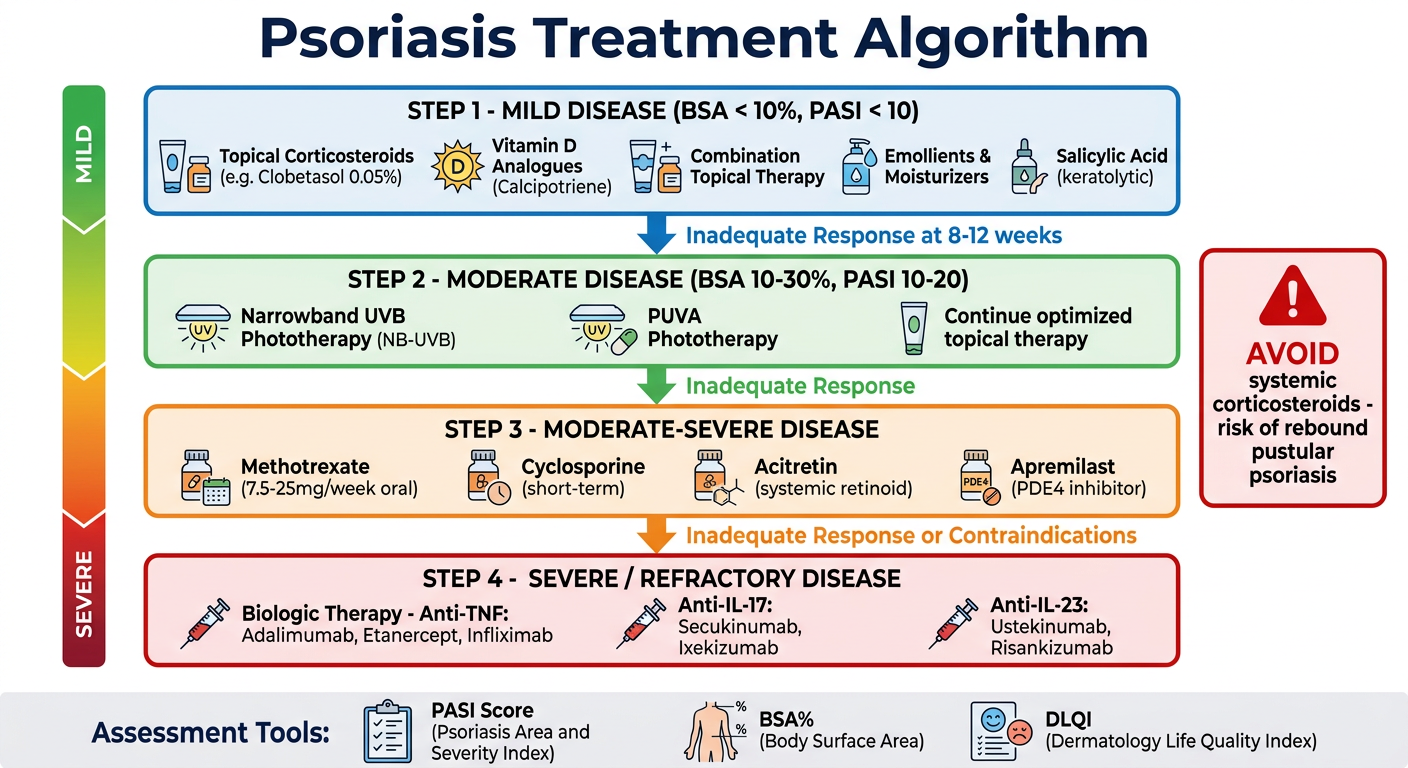
- Step 1 (Mild) - Topical agents: corticosteroids, calcipotriene, combination therapy
- Step 2 (Moderate) - Phototherapy: NB-UVB and PUVA
- Step 3 (Moderate-Severe) - Systemic agents: methotrexate, cyclosporine, acitretin, apremilast
- Step 4 (Severe/Refractory) - Biologic therapy: anti-TNF, anti-IL-17, anti-IL-23 agents
- Warning panel - Avoid systemic corticosteroids (risk of rebound pustular psoriasis)
- Assessment tools - PASI, BSA%, and DLQI at the bottom