Refractory headache in a 45 year female patient with history of migraine , not responding to triptans. No fever , no vomiting, no neck rigidity, no photophobia, no reeling. Bp is 140/90. Patient is not willing for CT brain
Reading File
Finding Sources
Finding Sources
Searching PubMed
refractory migraine treatment triptan failure
Finding Sources
Finding Sources
Searching PubMed
refractory migraine acute treatment emergency
Reading File
Finding Sources
Reading Article
PMID: 40715902
Reading File
Finding Sources
Loading Image
Searching the Web
refractory migraine not responding triptans treatment options 2025 guidelines
Reading Article
PMID: 40929517
Now I have a thorough picture. Let me compile the full clinical response.
Refractory Migraine - Triptan-Resistant, 45F with BP 140/90
Clinical Context First
This presentation is likely Status Migrainosus (migraine attack lasting >72 hours and not responding to usual therapy) or a severe refractory migraine attack. The absence of fever, neck stiffness, vomiting, photophobia, and focal neuro signs makes a sinister secondary cause (meningitis, SAH) less likely, and her known migraine history is reassuring. However, the elevated BP (140/90) should be noted - it may be pain-related hypertension (secondary to the headache itself) and needs monitoring.
Patient declining CT brain: With the clinical picture described (known migraineur, no red flag signs), this is clinically acceptable for now. However, it is important to document the conversation, explain the rationale for imaging, and revisit if the headache character changes or worsens.
Step 1 - Verify: Why Did Triptans Fail?
Before escalating, consider:
- Medication overuse headache (MOH): If she has been using triptans >10 days/month for >3 months, they can paradoxically worsen and perpetuate headache. In this case, triptans should be withdrawn, not escalated.
- Wrong triptan / wrong route: Oral triptans have slow onset (1-2 hrs). If not tried, subcutaneous sumatriptan (onset ~20 min) or intranasal zolmitriptan may still work.
- Taken too late: Triptans work best in the early/prodromal phase, not during established headache.
- Hypertension concern: BP of 140/90 is a relative caution for triptans (cardiovascular risk). This makes the case for triptan-free rescue options stronger.
Step 2 - Immediate Rescue Therapy Options
Since triptans have failed (or are now less appropriate given BP), the following are evidence-based options:
A. Dopamine Antagonists / Antiemetics (First-Line Rescue - AHS 2025 Level A)
These are the backbone of emergency migraine treatment. They work on central dopaminergic pathways:
| Drug | Dose | Notes |
|---|---|---|
| Metoclopramide | 10 mg IV/IM | Good evidence; also helps any nausea |
| Prochlorperazine | 10 mg IV | Strong evidence for pain relief; monitor for akathisia - give diphenhydramine 25mg IV alongside |
| Chlorpromazine | 12.5-25 mg IV | Effective but causes sedation/orthostatic hypotension |
The 2025 AHS updated ED guideline now includes metoclopramide + diphenhydramine as a Level A recommendation (must offer).
B. NSAIDs - Parenteral (Strong Option)
- Ketorolac 15-30 mg IV/IM - rapidly effective, non-vasoconstricting, safe with elevated BP. This is a strong choice here given the cardiovascular caution with triptans.
- If oral: Naproxen sodium 500-1000 mg or Ibuprofen 400-600 mg can be tried if not already used.
C. Corticosteroids - To Prevent Recurrence
- Dexamethasone 8-10 mg IV - does not abort the acute headache but significantly reduces the chance of headache recurrence within 24-72 hours. Best used as an adjunct.
D. Magnesium Sulfate
- IV Magnesium sulfate 1-2 g IV over 15-20 minutes
- Particularly useful in migraine with aura (AAFP evidence-based)
- Also has the added benefit of mild antihypertensive effect, which may be useful in this patient with BP 140/90.
E. Valproate Sodium (IV)
- Sodium valproate 500-1000 mg IV over 15-20 minutes
- Moderate evidence; commonly used in refractory migraine. Contradictory trial data but widely used in practice. Avoid in women of childbearing age unless contraception is confirmed (teratogenic).
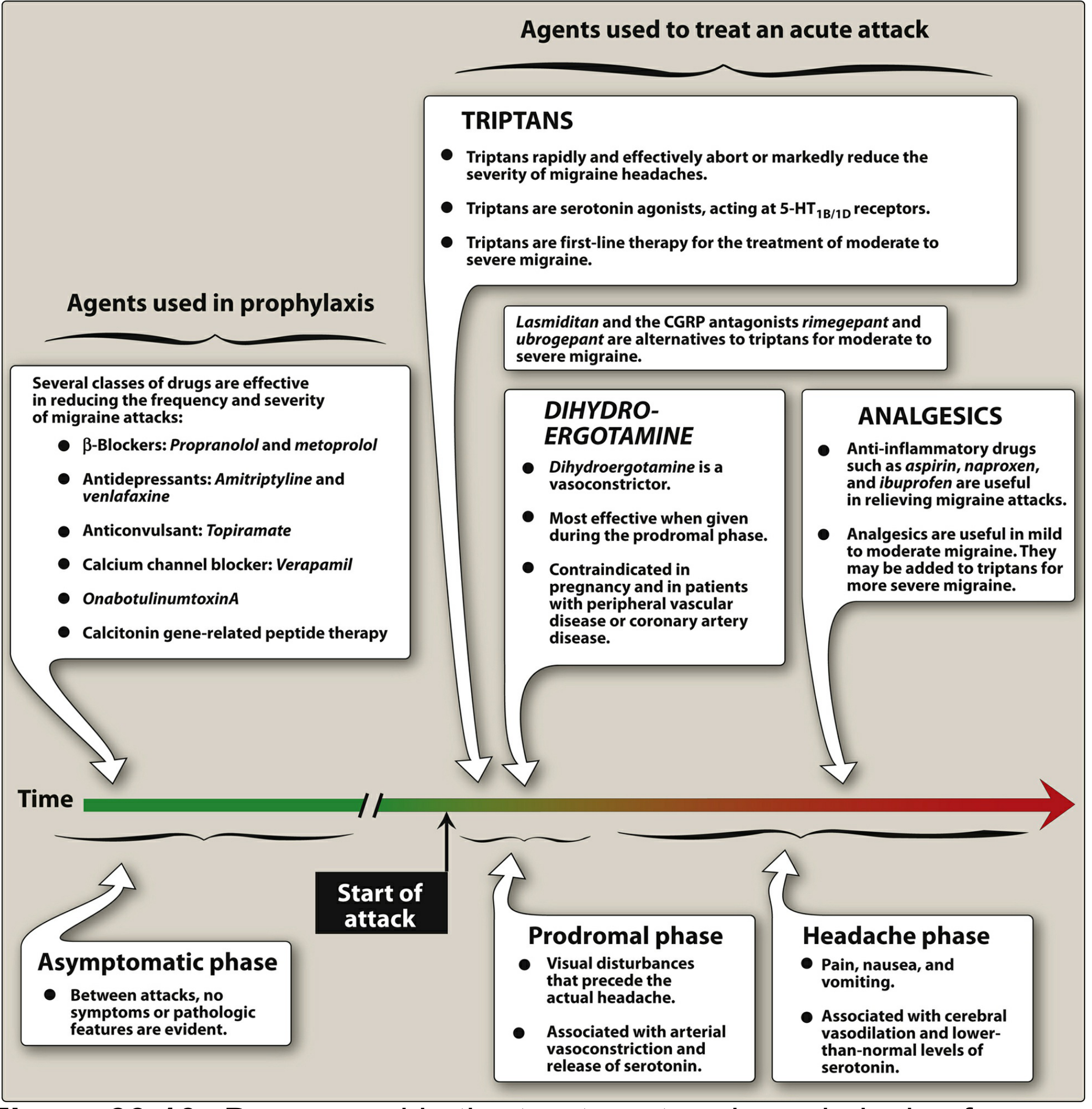
Step 3 - Triptan Alternatives (Newer Agents for Outpatient Use)
Since this patient has a known pattern of triptan non-response, consider switching drug class entirely:
| Agent | Class | Notes |
|---|---|---|
| Lasmiditan 50-200 mg oral | Ditan (5-HT1F agonist) | No vasoconstriction - safe in cardiovascular risk patients. Controlled substance. No driving for 8 hrs. |
| Rimegepant 75 mg ODT | CGRP antagonist (gepant) | Oral; suitable even with CV risk; also approved for prevention |
| Ubrogepant 50-100 mg oral | CGRP antagonist (gepant) | Avoid with strong CYP3A4 inhibitors |
These are FDA-approved alternatives specifically indicated for patients with contraindications or intolerance to triptans. - Lippincott Illustrated Reviews: Pharmacology, p. 1322-1323
Step 4 - Address the BP 140/90
- BP at 140/90 in a patient in pain is often secondary (pain-driven) and may resolve with adequate analgesia.
- Do not use triptans or ergot derivatives (DHE) in uncontrolled hypertension.
- Recheck BP once pain is controlled.
- If BP remains elevated after pain control, initiate antihypertensive management. Of note, propranolol and metoprolol (beta-blockers) are first-line for both migraine prophylaxis AND hypertension - so they serve a dual purpose here.
Step 5 - Migraine Prophylaxis (Preventive Therapy)
Given the severity and refractoriness, this patient needs preventive therapy regardless:
First-line options (dual benefit for HTN too):
- Propranolol 40-160 mg/day or Metoprolol 50-200 mg/day - first choice, also treats her hypertension
Other proven options:
- Topiramate 25-100 mg/day (weight loss is a side effect - may be beneficial)
- Amitriptyline 10-75 mg/night (if no contraindications)
- Venlafaxine 37.5-150 mg/day
CGRP-targeted prevention (for frequent/refractory cases):
- Erenumab, Galcanezumab, Fremanezumab (monthly/quarterly SC injections) - monoclonal antibodies
- Rimegepant or Atogepant (oral gepants) - also approved for prevention
- Consider referring to a neurologist/headache specialist for these
Step 6 - Red Flags to Reassess - Warn the Patient
Despite not meeting criteria now, revisit CT/MRI if any of the following appear:
- "Thunderclap" onset or worst-ever headache
- New neurological deficit (weakness, speech difficulty, visual loss)
- Headache worsening with position changes, Valsalva, or cough
- Fever develops or neck stiffness appears
- No response to any treatment after 48-72 hours
Document the patient's refusal of CT brain and that she was counseled on red flag symptoms.
Summary Algorithm for This Patient
Refractory migraine + BP 140/90 + Triptan failure
|
v
1. IV/IM Metoclopramide 10mg OR Prochlorperazine 10mg IV
(+ Diphenhydramine 25mg to prevent akathisia)
+
2. IV Ketorolac 30mg
+
3. IV Dexamethasone 8-10mg (to prevent recurrence)
|
v
If aura present or partial response:
4. IV Magnesium sulphate 1-2g over 15-20 min
|
v
No response after 60 min:
5. IV Sodium valproate 500-1000mg
|
v
Discharge planning:
- Oral gepant (rimegepant/ubrogepant) or lasmiditan as future acute Rx
- Start propranolol for prophylaxis (dual benefit for HTN)
- Neurology referral for CGRP monoclonal antibody consideration
- Headache diary, medication overuse check
Key References
- Lippincott Illustrated Reviews: Pharmacology, pp. 1322-1324 (Migraine acute and prophylactic therapy)
- AHS 2025 Guideline Update - Acute Treatment of Migraine in the Emergency Department (Robblee et al., Headache, Dec 2025) - establishes metoclopramide + diphenhydramine as Level A
- ACP 2025 Guideline - Pharmacologic Treatments for Acute Episodic Migraine (Annals of Internal Medicine, March 2025)
- Weant & Gregory, "Pharmacotherapy Management of Acute Migraine in the Emergency Department," Adv Emerg Nurs J, 2025 [PMID: 40929517]
- Mayers et al., "Status Migrainosus - A Narrative Review," Curr Neurol Neurosci Rep, 2025 [PMID: 40715902]
Clinical Note on CT Refusal: This is acceptable in a known migraineur with no new red flags. The 140/90 BP warrants monitoring. If she continues to present with refractory attacks or any red flag develops, CT/MRI Brain becomes non-negotiable regardless of patient preference.
This is a shared conversation. Sign in to Orris to start your own chat.